Klebsiella Hospital Infection Control and Prevention
- Why Klebsiella Spreads So Easily in Hospitals
- Hand Hygiene: The Single Most Effective Prevention
- Contact Precautions: Gowns and Gloves Explained
- The CAUTI Prevention Bundle
- The VAP Prevention Bundle
- Environmental Cleaning and Terminal Disinfection
- Active Surveillance Cultures and Outbreak Investigation
- Antimicrobial Stewardship: Protecting Antibiotics for the Future
- Key Research Papers
- Connections
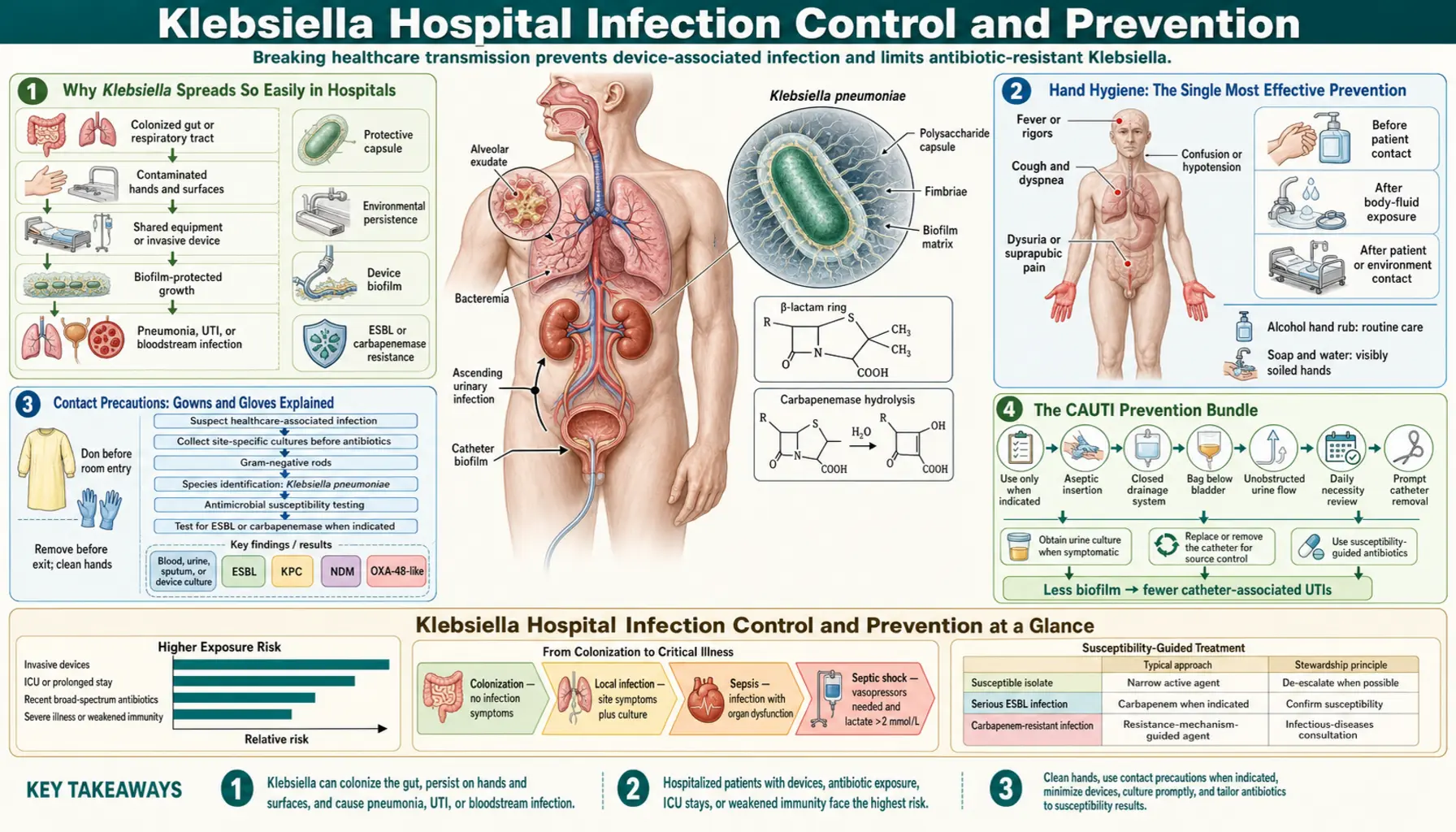
Why Klebsiella Spreads So Easily in Hospitals
If you or a family member is in the hospital, it can be alarming to hear that a bacteria called Klebsiella pneumoniae is circulating on the ward. Understanding exactly why this organism thrives in healthcare settings helps make sense of all the precautions you will see staff carrying out around the clock.
Klebsiella pneumoniae produces a thick, sugar-based outer coating called a polysaccharide capsule. This capsule does two important things: it protects the bacterium from the body's immune system, and it allows it to survive drying out. Most bacteria die within minutes when they land on a dry surface such as a bedrail, call button, or IV pole. Klebsiella can survive for days to weeks on these surfaces, quietly waiting for a new host.
Healthcare workers' hands are the main highway between patients. A nurse or doctor may touch a contaminated bedrail, then touch a patient's central line or urinary catheter port within seconds. Studies using fluorescent markers have shown that a single contaminated surface can spread to 14 or more other sites within 30 minutes during normal clinical care.
Several patient-level factors also make hospital patients unusually vulnerable:
- Invasive devices — urinary catheters, central venous lines, and ventilator tubes bypass the body's normal skin and mucous-membrane defenses.
- Broad-spectrum antibiotic exposure — killing off the normal bacterial flora of the gut and skin creates ecological space for Klebsiella to colonize in large numbers.
- Immune suppression — chemotherapy, organ transplant drugs, high-dose steroids, and critical illness all blunt the defenses that would normally keep a colonizing bacterium from causing disease.
- Prolonged hospitalization — the longer a patient stays, the more surfaces and staff they encounter and the higher their cumulative exposure risk.
Outbreak investigations at major medical centers have traced single transmission chains back months using whole-genome sequencing, revealing that one colonized patient admitted to the ICU can seed an entire ward if hand hygiene and contact precautions slip.
Hand Hygiene: The Single Most Effective Prevention
Among all infection control measures ever studied in hospitals, proper hand hygiene has the strongest, most consistent evidence behind it. The World Health Organization estimates that if every healthcare worker cleaned their hands at every required moment, healthcare-associated infections would fall by at least 50 percent. For Klebsiella specifically, outbreak investigations routinely identify lapses in hand hygiene as the key contributing factor.
The Five Moments of Hand Hygiene
The WHO framework describes five specific moments when healthcare workers must perform hand hygiene:
- Before touching a patient — even before adjusting pillows or taking a pulse.
- Before a clean or aseptic procedure — inserting a needle, changing a dressing, or accessing a catheter port.
- After body fluid exposure risk — after removing gloves, after contact with secretions or wounds.
- After touching a patient — even if the contact appeared minor.
- After touching patient surroundings — bedrails, IV pumps, call buttons, and bedside tables in the patient's zone all count.
Alcohol Gel vs. Soap and Water
Alcohol-based hand rub (the gel dispensers you see at every room entrance) is the preferred method in most situations because it is faster, gentler on skin, and more effective at killing Klebsiella than a quick soap-and-water rinse. A thorough alcohol rub takes about 20 to 30 seconds and kills 99.99 percent of the bacterial load on hands.
Soap and water is preferred when hands are visibly soiled with blood or body fluids, and it is essential after caring for patients with Clostridioides difficile (because spores resist alcohol). For Klebsiella, either method is effective when performed correctly.
What You Can Do as a Patient or Family Member
You have every right to ask — politely but directly — whether a healthcare worker has cleaned their hands before touching you. Research shows that patient empowerment significantly improves compliance. Many hospitals have patient safety programs that explicitly encourage this. You can also ask visitors to use the hand gel at the room entrance every time they arrive and before they leave.
Compliance Monitoring
Hospitals track hand hygiene compliance through direct observation audits, electronic counting systems on dispensers, and video monitoring in some units. Rates below 80 percent are associated with significantly higher rates of healthcare-associated infections. High-performing infection control programs target 90 percent or above and give ward teams real-time feedback.
Contact Precautions: Gowns and Gloves Explained
When a patient is found to be colonized or infected with Klebsiella pneumoniae — especially drug-resistant strains like ESBL-producers or carbapenem-resistant Klebsiella (CRE-Kp) — the hospital places them on contact precautions. A sign outside the room notifies everyone who enters. This section explains what that means in plain language for patients and families.
What Staff Must Do
Before entering the room, every healthcare worker puts on a disposable gown and gloves. These are removed and discarded before leaving the room — not in the hallway — to prevent carrying the organism outside the patient's zone. If gloves are removed and the worker then touches a surface in the room, they must re-glove before touching the patient again.
The gown protects the worker's clothing from picking up Klebsiella that has settled on sheets and rails. Even casual contact — leaning against the bedrail while adjusting an IV line — can transfer enough bacteria to seed another patient room.
Single Room or Cohorting
The gold standard is a single room with its own bathroom. Private rooms dramatically reduce cross-transmission because the environmental reservoir stays contained. When single rooms are unavailable — a common reality in busy hospitals — patients colonized with the same organism may be cohorted (placed together in a shared bay) so that staff caring for them do not simultaneously care for unexposed patients.
During outbreak situations, some hospitals go further and dedicate specific nursing staff to cohorted patients, completely separating them from the nursing team caring for unaffected patients on the same floor.
What Contact Precautions Mean for Patients Day-to-Day
Being on contact precautions can feel isolating. Visitors must gown and glove before entering, which creates a physical barrier that can feel dehumanizing. Patients on precautions are less likely to receive spontaneous check-ins from staff, which research has shown can delay recognition of clinical deterioration.
Good infection control programs actively work against this. Staff are encouraged to make the same frequency of patient contact — just in appropriate PPE. Families are briefed on gowning technique so they can visit comfortably. Patients should feel empowered to use the call bell freely; being on contact precautions does not mean being abandoned.
Visitor Guidance
- Put on the gown and gloves from the cart outside the door before entering.
- Do not sit on the bed or use the bathroom in the patient's room.
- Remove and discard PPE inside the room before leaving.
- Clean hands with alcohol gel immediately after removing gloves.
- Limit the number of visitors at one time to reduce traffic in and out of the room.
The CAUTI Prevention Bundle
CAUTI stands for catheter-associated urinary tract infection. The urinary catheter — the thin tube inserted through the urethra into the bladder to drain urine — is the most common route by which Klebsiella enters the urinary tract in hospitalized patients. Klebsiella is one of the top three organisms isolated from CAUTIs in intensive care units worldwide.
A prevention "bundle" is a package of evidence-based steps that, when all applied together, produce better results than any single measure alone. The CAUTI bundle has five core components:
1. Indication Review: Does This Patient Need a Catheter?
The safest catheter is the one that was never inserted. Before placing a urinary catheter, nurses and doctors should verify that there is a genuine medical reason — such as urinary obstruction, the need for precise fluid monitoring in a critically ill patient, or perioperative use during certain surgeries. Convenience — making it easier to manage incontinence or avoid frequent toileting — is not an acceptable indication and significantly increases infection risk.
2. Aseptic Insertion Technique
Insertion is a sterile procedure. The clinician uses sterile gloves, a sterile drape, and sterile lubricant. The urethral meatus is cleaned with antiseptic. Using a pre-packaged sterile catheter insertion kit — a standard practice in most hospitals — reduces the risk of contamination during the procedure itself.
3. Maintaining a Closed Drainage System
Once the catheter is in place, the drainage tubing and collection bag form a closed system. Breaking that seal — to obtain a urine sample incorrectly, to unkink tubing carelessly — introduces bacteria. Urine samples should be drawn through the designated sampling port with a sterile needle, not by disconnecting the bag. The collection bag must be kept below the level of the bladder at all times to prevent urine backflow.
4. Daily Removal Assessment
Every day the nursing team should formally ask: does this patient still need the catheter? Studies consistently show that when hospitals implement a daily "stop order" — an automatic prompt to reassess catheter necessity — catheter days drop by 20 to 40 percent and CAUTI rates fall proportionally. Removing the catheter as soon as it is no longer needed is the most powerful CAUTI prevention step of all.
5. Catheter Care and Securement
The catheter should be secured to the thigh to prevent it moving in and out of the urethra — movement drags bacteria up the outside of the tube toward the bladder. The perineal area around the catheter entry site should be cleaned with soap and water during daily bathing; routine antiseptic cleaning of the meatus has not been shown to reduce infections and is not recommended.
The VAP Prevention Bundle
VAP — ventilator-associated pneumonia — is the most severe form of hospital-acquired pneumonia. It develops in patients who are breathing through a mechanical ventilator, a machine that delivers air through a tube inserted down the throat into the trachea (windpipe). Klebsiella pneumoniae is consistently among the top organisms isolated from VAP in ICUs, particularly in hospitals where carbapenem-resistant strains have emerged.
The VAP bundle is a package of four core interventions that together reduce VAP incidence by 50 to 70 percent when implemented reliably:
1. Head-of-Bed Elevation (30–45 Degrees)
When a ventilated patient lies flat, secretions from the mouth and throat pool at the back of the airway and slowly trickle down around the ventilator tube into the lungs — a process called micro-aspiration. Keeping the head of the bed elevated at 30 to 45 degrees uses gravity to keep those secretions above the tube cuff. Staff check and document the bed angle at every shift handover. If you are visiting a ventilated family member in the ICU and you notice the bed is flat, it is appropriate to alert a nurse.
2. Oral Care with Chlorhexidine
The mouth of a ventilated patient rapidly becomes colonized with bacteria — including Klebsiella — because normal swallowing and speaking, which naturally clear the mouth, are suppressed. Chlorhexidine oral rinse applied every 6 to 12 hours reduces the bacterial load in the oropharynx and significantly reduces VAP rates in cardiac surgery patients; evidence is somewhat more mixed in medical ICU patients but the practice remains a standard bundle component.
3. Subglottic Secretion Drainage
Modern ventilator tubes have a small extra channel just above the inflated cuff that sits in the trachea. Using gentle suction through this channel every few hours removes the pool of secretions that accumulates above the cuff — the secretions that would otherwise slowly leak around it into the lungs. Meta-analyses show this single intervention reduces VAP incidence by approximately 45 percent.
4. Spontaneous Awakening and Breathing Trials
The longer a patient remains on the ventilator, the greater the cumulative infection risk. Paired daily spontaneous awakening trials (reducing sedation to see if the patient can be awakened) and spontaneous breathing trials (reducing ventilator support to see if the patient can breathe on their own) significantly shorten time on the ventilator and therefore time at risk for VAP. These trials are now standard practice in most ICUs and have transformed how critical care sedation is managed.
Environmental Cleaning and Terminal Disinfection
Because Klebsiella can survive on surfaces for weeks, environmental cleaning is not just housekeeping — it is a direct infection control intervention. Multiple outbreak investigations have documented patient-to-patient transmission traced entirely to contaminated room surfaces after a previous patient was discharged.
Daily Cleaning During Admission
High-touch surfaces in an isolation room — bedrails, call bell, overbed table, IV pole, light switches, door handles, and toilet surfaces — should be cleaned with a hospital-grade disinfectant at least once daily, and more frequently in ICUs. The choice of disinfectant matters: quaternary ammonium compounds (common general-purpose hospital disinfectants) are effective against Klebsiella. Bleach-based sporicidal agents are added when C. difficile is also present.
Terminal Disinfection After Discharge
Terminal disinfection refers to the thorough cleaning and disinfection of a room after the patient leaves — before the next patient is admitted. For rooms that housed a patient with drug-resistant Klebsiella, standard terminal disinfection alone may not be sufficient. Studies have shown that manual cleaning misses 30 to 40 percent of surfaces even when staff follow protocols carefully.
Two adjunctive technologies have strong evidence:
- Hydrogen peroxide vapor (HPV) — a machine fills the sealed room with vaporized hydrogen peroxide, which penetrates under furniture, into mattress folds, and around fixtures. HPV reduces the bacterial burden on surfaces by 99.9 percent or more and has been shown in randomized trials to reduce subsequent patient acquisition of resistant organisms.
- UV-C light robots — robotic devices that emit intense ultraviolet-C light damage bacterial DNA, killing organisms on all exposed surfaces within about 20 minutes. Multiple studies support their use as an adjunct to manual cleaning in high-risk rooms.
Copper Surfaces
Copper and copper alloys have intrinsic antimicrobial properties — bacteria landing on copper surfaces are killed within hours, not days. Clinical trials replacing commonly touched surfaces (bedrails, IV pole handles, call buttons, tray tables) with solid copper alloy have demonstrated significant reductions in surface contamination and in healthcare-associated infection rates. While the upfront cost has limited widespread adoption, copper surfaces are increasingly being used in new hospital construction and renovation.
Mattresses and Equipment
Mattress covers must be intact — any cracks or tears allow bacteria to penetrate the foam core, which cannot be effectively disinfected. Shared equipment such as blood pressure cuffs, stethoscopes, and infusion pumps are important vectors; ideally each patient on contact precautions has dedicated equipment that does not leave their room. If equipment must be shared, it must be disinfected between each patient use.
Active Surveillance Cultures and Outbreak Investigation
Many patients carry Klebsiella pneumoniae — including drug-resistant strains — without being sick from it. This is called colonization. A colonized patient has no symptoms but can still spread the organism to others. Active surveillance means proactively testing patients to find these invisible carriers before they become a transmission source.
Rectal Screening Swabs
The gut is the main reservoir of Klebsiella in colonized patients. A simple swab of the rectal area — processed on a selective culture plate or by rapid PCR — can detect carbapenem-resistant Klebsiella (CRE-Kp) within hours to a day. The swab is quick, painless, and non-invasive.
Who Gets Screened?
Screening protocols vary by hospital and local epidemiology, but common criteria include:
- Patients transferred from facilities in countries or regions with high CRE-Kp prevalence (parts of Southern and Eastern Europe, the Middle East, South Asia).
- Patients transferred from other hospitals, especially ICUs.
- Patients who have been hospitalized abroad within the past 12 months.
- All patients admitted to ICUs at hospitals where CRE-Kp has been identified.
- Contacts of a newly identified CRE-Kp case on the same ward.
Rapid PCR Testing
Traditional culture takes 48 to 72 hours. Rapid PCR assays can detect the most important carbapenemase genes (KPC, NDM, OXA-48, VIM, IMP) directly from a rectal swab within 3 to 5 hours. This speed matters enormously: a patient may spend two full nursing shifts in a shared bay before culture results return, during which transmission continues. Rapid PCR allows same-day isolation decisions.
Whole-Genome Sequencing in Outbreaks
When a cluster of cases is identified on a ward, public health laboratories can perform whole-genome sequencing (WGS) on the bacterial isolates from each patient. Because every bacterial cell replicates its genome with occasional random mutations, strains that are closely related share almost identical genomes. WGS can determine with high confidence whether cases share a common transmission chain — and can sometimes identify a specific environmental source or a specific healthcare worker's hands as the amplifier.
WGS-guided outbreak investigations have transformed infection control in the last decade. Several notable outbreaks at major hospitals — including at the NIH Clinical Center and at a UK neonatal unit — were only fully understood and controlled after WGS revealed hidden transmission links that conventional epidemiology had missed.
Antimicrobial Stewardship: Protecting Antibiotics for the Future
Every time a broad-spectrum antibiotic is prescribed — especially carbapenems — it exerts selective pressure on bacteria throughout the hospital environment and in the patient's own gut flora. Organisms that happen to carry resistance genes survive and multiply while sensitive competitors are killed off. This is precisely how carbapenem-resistant Klebsiella (CRE-Kp) strains have emerged and spread globally.
Antimicrobial stewardship programs (ASPs) exist specifically to counter this. An ASP is a coordinated, institution-wide effort to ensure that antibiotics are prescribed only when truly needed, at the right dose, for the right duration, and with the narrowest spectrum appropriate for the infection.
How Stewardship Programs Work
At most hospitals, the ASP team includes infectious disease physicians, clinical pharmacists, and microbiologists who review antibiotic prescriptions on a daily basis. They use several strategies:
- Prospective audit and feedback — the ASP team reviews prescriptions and contacts the treating team to discuss opportunities to de-escalate or stop antibiotics, explaining the reasoning rather than simply overriding the prescriber.
- Prior authorization — prescribers must obtain ASP approval before initiating certain high-risk antibiotics (carbapenems, newer agents like ceftazidime-avibactam) except in life-threatening emergencies.
- De-escalation — once culture results return and the specific organism and its sensitivities are known, the team recommends switching from a broad-spectrum agent to the narrowest effective option.
- Duration limits — automatic 72-hour stop orders prompt a formal reassessment of whether antibiotic therapy should continue. Shorter courses have been shown to be as effective as longer ones for many common infections while generating far less resistance.
Restricting Carbapenems
Carbapenems are often called the antibiotic "last resort" for serious gram-negative infections. Their overuse is the primary driver of carbapenem-resistant Klebsiella. Hospitals with active carbapenem restriction programs — requiring infectious disease or ASP sign-off before use — have demonstrated sustained reductions in CRE-Kp incidence. This is not about rationing care; it is about ensuring carbapenems remain effective for patients who genuinely need them.
What Patients and Families Can Do
Antimicrobial stewardship is not only a hospital program — it extends to patients and families. You can help protect antibiotics by:
- Asking your doctor whether an antibiotic is truly necessary for your condition, and if so, which one is most targeted to your specific infection.
- Completing the prescribed course — stopping early because you feel better is not safer; it can leave partially resistant organisms behind.
- Never taking leftover antibiotics or antibiotics prescribed for someone else.
- Supporting your care team if they suggest de-escalating from a powerful antibiotic to a more specific one once your culture results are back — this is good medicine, not cutting corners.
Key Research Papers
The following peer-reviewed studies form the evidence base for modern Klebsiella pneumoniae hospital infection control and prevention practices.
- Tacconelli et al. (2014) — Contact precautions and CRE transmission: Randomized evidence on the impact of contact precautions on patient acquisition of resistant gram-negative organisms. — Search PubMed
- Cassini et al. (2019) — Burden of healthcare-associated infections: European-wide prevalence study quantifying the burden of hospital-acquired infections including Klebsiella-caused infections and deaths attributable to antimicrobial resistance. — Search PubMed
- Davido et al. (2017) — CAUTI bundle outcomes in ICU: Prospective cohort study demonstrating reduction in catheter-associated urinary tract infections with structured bundle implementation in a French medical ICU. — Search PubMed
- Wittekamp et al. (2018) — Selective decontamination and infection control: Large multicenter randomized trial comparing strategies for reducing ICU-acquired infections from gram-negative pathogens including carbapenem-resistant Klebsiella. — Search PubMed
- Birgand et al. (2018) — WGS in hospital outbreak investigation: Demonstrates how whole-genome sequencing changed understanding of CRE-Kp transmission dynamics in a French teaching hospital and guided targeted interventions. — Search PubMed
- Karampatakis et al. (2020) — Environmental survival of Klebsiella: Documents the duration of K. pneumoniae survival on hospital surfaces and the implications for terminal disinfection protocols and cleaning frequency. — Search PubMed
- Anderson et al. (2017) — UV-C robot disinfection RCT: Large multicenter randomized trial (Benefits of Enhanced Terminal Room Disinfection) demonstrating that UV-C light disinfection after standard manual cleaning significantly reduces acquisition of resistant organisms from prior-room patients. — Search PubMed
- Magill et al. (2018) — National HAI prevalence survey: Updated CDC point-prevalence survey of healthcare-associated infections in US hospitals, providing contemporary data on the distribution of pathogens including Klebsiella across infection types. — Search PubMed
- Thaden et al. (2017) — Outcomes of CRE-Kp bloodstream infections: Retrospective cohort study showing excess mortality and cost attributable to carbapenem-resistant versus carbapenem-susceptible K. pneumoniae bacteremia, supporting the case for aggressive prevention. — Search PubMed
- Septimus & Schweizer (2016) — Decolonization strategies: Review of chlorhexidine bathing and mupirocin decolonization bundled with active surveillance for reducing transmission of multidrug-resistant organisms in hospital settings. — Search PubMed
Connections
- All Bacteria
- Klebsiella Pneumoniae Overview
- Klebsiella Treatments Hub
- Beta-Lactam and Aminoglycoside Treatment
- ESBL, CRE, and Carbapenem Resistance
- Hospital-Acquired Pneumonia and UTI
- Klebsiella Symptoms Hub