Pertussis Treatment: Azithromycin and Macrolide Antibiotics
Whooping cough is treated primarily with macrolide antibiotics — a class that includes azithromycin, clarithromycin, and erythromycin. Antibiotics can dramatically shorten how long you are contagious, protect household members, and in early cases may reduce the severity and duration of coughing. Understanding when and how to use them is essential for protecting yourself, your family, and your community.
- The Critical Window — Why Timing Matters
- Azithromycin — First-Line Choice
- Why Azithromycin Is Preferred Over Erythromycin in Infants
- Clarithromycin — An Alternative Option
- Erythromycin — The Historical Standard
- TMP-SMX — For Macrolide-Intolerant Patients
- Post-Exposure Prophylaxis
- Hospital Management of Infants
- Isolation Period and Returning to School or Work
- Key Research Papers
- Connections
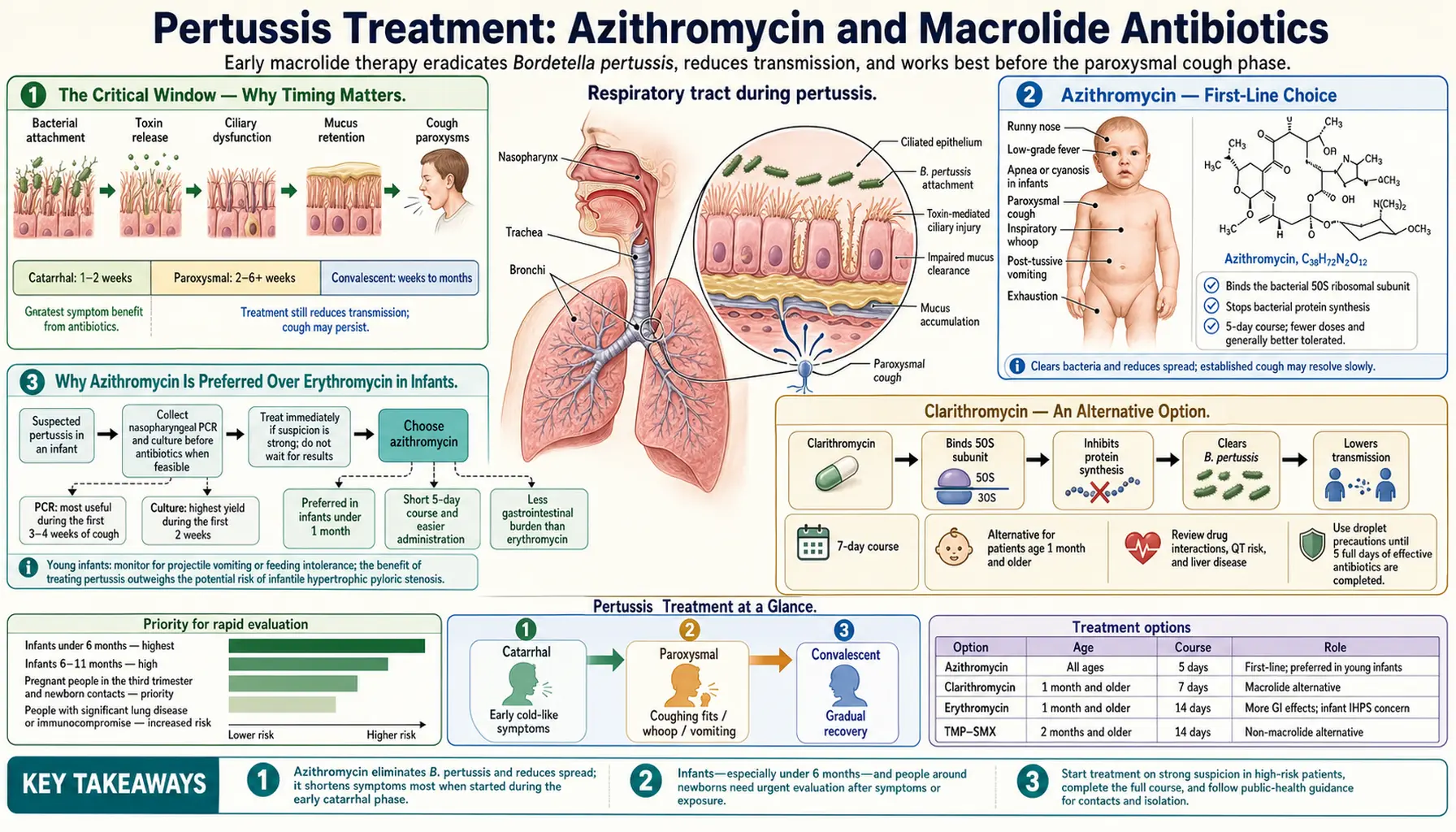
The Critical Window — Why Timing Matters
Pertussis has three stages, and antibiotics behave very differently depending on when they are started. During the first stage — called the catarrhal phase — which lasts about one to two weeks, the bacteria are actively multiplying and spreading within your airways. If you receive antibiotics during this stage, they can eliminate the bacteria, reduce how long you are infectious, and may prevent the worst coughing from developing at all.
Once you enter the second stage — the paroxysmal phase — the violent coughing fits are already established. By this point the toxins that trigger the cough have already done their damage to the airway lining, and antibiotics will not make the cough go away faster or reduce its severity. However, antibiotic treatment during this later phase is still very worthwhile: it stops you from spreading the disease to others and clears the bacteria so household contacts and close contacts can also be treated prophylactically.
The practical challenge is that most people do not recognize pertussis in its early, treatable stage. What feels like an ordinary cold — runny nose, mild cough — is actually the catarrhal phase. By the time the characteristic "whoop" and paroxysms are obvious, the window to prevent serious illness has already closed. This is why a high index of suspicion and rapid testing are so important, especially in households with infants.
Azithromycin — First-Line Choice
Azithromycin (brand name Zithromax, also available as generic Z-Pack) is the antibiotic recommended first by the CDC and the American Academy of Pediatrics for treating pertussis in most patients. Its advantages include once-daily dosing, a short five-day course, and excellent tolerability compared to older options.
Dosing for adults: 500 mg on Day 1, then 250 mg on Days 2 through 5. Total course = 5 days.
Dosing for children (1 month and older): 10 mg per kilogram of body weight on Day 1 (maximum 500 mg), then 5 mg/kg on Days 2 through 5 (maximum 250 mg/day). Total course = 5 days.
Dosing for infants under 1 month: 10 mg/kg/day for 5 days. This is an age group that requires careful monitoring (see the section on infant safety below).
Azithromycin is a macrolide antibiotic — it works by binding to the bacterial ribosome and blocking protein synthesis. For Bordetella pertussis, this prevents the bacteria from producing the toxins and adhesins that allow it to attach to and damage respiratory cells.
The short course and once-daily dosing improve the likelihood that patients (especially children and parents of young infants who are running on little sleep) will actually complete the full antibiotic course.
Why Azithromycin Is Preferred Over Erythromycin in Infants
This distinction is one of the most clinically important pieces of information for new parents and pediatricians. Erythromycin — which was the standard treatment for pertussis for decades — is now avoided in babies under one month of age because of a serious risk.
Erythromycin given to newborns and young infants is associated with infantile hypertrophic pyloric stenosis (IHPS), a condition in which the muscular valve at the outlet of the stomach (the pylorus) becomes abnormally thickened and narrowed. Infants with IHPS develop projectile vomiting, become unable to keep feedings down, and require surgical correction. The association was first recognized in population studies and has been confirmed by multiple subsequent analyses.
Azithromycin has a much better safety record in newborns and is now preferred for infants of all ages. While azithromycin also carries a small reported association with IHPS (since it acts on the same motilin receptor), the risk appears considerably lower than with erythromycin. Parents and clinicians should be aware of this history and ask which antibiotic is being prescribed when a newborn needs pertussis treatment.
Clarithromycin — An Alternative Option
Clarithromycin (brand name Biaxin) is another macrolide antibiotic with effectiveness against Bordetella pertussis that is comparable to azithromycin. It is recommended as a second choice when azithromycin is unavailable, not tolerated, or when there are specific clinical reasons to prefer it.
Dosing for children 1 month and older: 15 mg/kg/day divided into two doses (given every 12 hours), maximum 1 g/day. Total course = 7 days.
Dosing for adults: 500 mg twice daily for 7 days.
Clarithromycin is not recommended for infants under 1 month because safety data in that age group are insufficient. The twice-daily dosing and longer course (7 days vs. 5 days for azithromycin) make adherence slightly more challenging. Clarithromycin also has more drug interactions than azithromycin because it is a stronger inhibitor of the liver enzyme CYP3A4, which breaks down many common medications. Your pharmacist can check for interactions with other drugs you take.
Erythromycin — The Historical Standard
Erythromycin was the first-choice treatment for whooping cough from the 1950s through the 1990s and remains in use in some low-resource settings where it is valued primarily for its very low cost. However, it has largely been replaced by azithromycin in high-income countries for several reasons.
Dosing: 40–50 mg/kg/day divided into four doses (given every 6 hours), maximum 2 g/day. Total course = 14 days.
A 14-day four-times-daily regimen has much lower adherence rates than azithromycin's 5-day once-daily course. Erythromycin also causes significant gastrointestinal side effects — nausea, stomach cramping, and diarrhea — in a large proportion of patients because it stimulates gut motility through motilin receptors.
Most importantly, erythromycin must be avoided in newborns and infants under 1 month because of the association with infantile hypertrophic pyloric stenosis described above. If erythromycin is the only available macrolide, the clinical benefit in a confirmed pertussis case must be weighed against this risk, and parents should be counseled to watch for signs of IHPS (projectile vomiting, inability to feed).
TMP-SMX — For Macrolide-Intolerant Patients
Trimethoprim-sulfamethoxazole (TMP-SMX, brand names Bactrim and Septra) is the recommended alternative for patients who cannot take macrolide antibiotics — for example, patients with macrolide allergy or those on medications with dangerous macrolide interactions.
Adult dosing: One double-strength (DS) tablet (160 mg TMP / 800 mg SMX) twice daily for 14 days.
Pediatric dosing: 8 mg of the TMP component per kilogram per day, divided into two doses every 12 hours, for 14 days.
Important restriction: TMP-SMX is not recommended for infants under 2 months of age. In very young babies, the sulfonamide component can displace bilirubin from protein binding sites and cause it to deposit in the brain — a condition called kernicterus, which causes permanent neurological damage. Macrolides are therefore the only option for this youngest and most vulnerable age group.
TMP-SMX is also important in the context of emerging antibiotic resistance. If B. pertussis strains with macrolide resistance are encountered, TMP-SMX remains effective because it targets a completely different bacterial pathway (folate synthesis).
Post-Exposure Prophylaxis
One of the most impactful steps in controlling pertussis is treating everyone exposed to a confirmed case — not just the sick person. This is called post-exposure prophylaxis (PEP).
The CDC recommends PEP for:
- All household members of a confirmed pertussis case, regardless of vaccination status
- Close contacts of a case who are themselves high-risk or who have contact with high-risk individuals (infants under 12 months, pregnant women in the third trimester, people with compromised immune systems)
- Healthcare workers with unprotected exposure to a pertussis case
The same antibiotic regimens used for treatment are used for prophylaxis — the drugs, doses, and courses are identical. The critical time window for PEP is within 21 days of exposure; after 21 days from exposure, prophylaxis is unlikely to prevent disease. However, even outside this window, treating exposed individuals is still beneficial to prevent them from spreading the disease to others.
Vaccination does not eliminate the need for PEP. Even fully vaccinated contacts should receive antibiotics if a baby under 12 months lives in or regularly visits their household, because vaccinated people can still carry and transmit the bacteria, and infants are at the highest risk for severe illness and death.
Hospital Management of Infants
Infants under 12 months — and especially those under 3 months — account for the overwhelming majority of pertussis deaths. Hospital admission is strongly considered for any infant with confirmed or suspected pertussis, because these babies can deteriorate rapidly.
In the hospital, key management elements include:
- Continuous monitoring: Pulse oximetry (oxygen saturation) and cardiorespiratory monitoring to detect apnea (pauses in breathing), which is common and dangerous in young infants with pertussis
- Oxygen supplementation: Provided as needed when saturations drop during coughing paroxysms
- Suctioning: Gentle nasopharyngeal suctioning to clear secretions that infants cannot clear themselves
- Feeding modifications: Small, frequent feeds reduce the risk of vomiting triggered by coughing; in severe cases, nasogastric feeding may be required
- PICU consideration: Infants with apnea, hypoxia requiring high-flow oxygen, or a white blood cell count above 30,000 cells per microliter should be evaluated for pediatric intensive care admission. Extreme leukocytosis (WBC above 50,000–100,000) is a marker of severe disease associated with pulmonary hypertension and a high fatality rate
- Isolation precautions: Standard droplet precautions, including gowns and masks, for all healthcare personnel entering the room
Systemic corticosteroids and bronchodilators (like albuterol) have been studied in pertussis and do not improve outcomes — they are not recommended as routine treatment. The primary interventions are supportive care and antibiotics.
Isolation Period and Returning to School or Work
Pertussis is highly contagious from the very beginning of symptoms through the paroxysmal stage. Understanding when it is safe to return to normal activities protects others, especially infants and immunocompromised people who may be in your workplace, school, or daycare.
If you are treated with antibiotics: You should stay home and away from others until you have completed at least 5 full days of appropriate antibiotic therapy. After 5 days of azithromycin, you are no longer considered contagious.
If you are not treated with antibiotics: You remain potentially contagious for 21 days after the onset of cough. This is a long time — three weeks — which is why antibiotic treatment is strongly encouraged even in later stages of illness.
Schools, daycares, and workplaces may require documentation from a healthcare provider confirming that you have completed antibiotics or that the 21-day period has elapsed before allowing return. If you work with infants, young children, pregnant women, or immunocompromised patients, check with your employer about specific return-to-work policies.
Key Research Papers
- Tiwari T, et al. Recommended antimicrobial agents for the treatment and postexposure prophylaxis of pertussis. MMWR Recomm Rep. 2005;54(RR-14):1-16. — Search PubMed
- Altunaiji S, et al. Antibiotics for whooping cough (pertussis). Cochrane Database Syst Rev. 2007;(3):CD004404. PMID 17636756
- Langley JM, et al. Azithromycin is as effective as and better tolerated than erythromycin estolate for the treatment of whooping cough. Pediatrics. 2004;114(1):e96-101. — Search PubMed
- Lebel MH, et al. Comparison of azithromycin and erythromycin estolate for the treatment of infant pertussis. Pediatr Infect Dis J. 2001;20(5):545-6. — Search PubMed
- Mahon BE, et al. Effectiveness of pertussis vaccines for children: a meta-analysis. Pediatrics. 2014;133(2):278-85. — Search PubMed
- Kilgore PE, et al. Pertussis: Microbiology, Disease, Treatment, and Prevention. Clin Microbiol Rev. 2016;29(3):449-86. PMID 27029594
- Carbonetti NH. Pertussis leukocytosis: mechanisms, clinical implications and treatment considerations. Curr Opin Infect Dis. 2016;29(3):257-64. — Search PubMed
- Villani P, et al. Effectiveness of early azithromycin treatment in pertussis. J Infect. 2003;47(1):52-5. — Search PubMed
- Cherry JD. Epidemic pertussis in 2012. N Engl J Med. 2012;367:785-787. — Search PubMed
- American Academy of Pediatrics. Pertussis. In: Red Book: 2021 Report of the Committee on Infectious Diseases. 2021:547-558.
- Centers for Disease Control and Prevention. Pertussis Treatment. cdc.gov/pertussis/clinical/treatment.html. Reviewed 2022.
Connections
- All Bacteria
- Treatment & Prevention — Overview
- DTaP & Tdap Vaccines
- Waning Immunity and Antibiotic Resistance
- Symptoms & Whooping Cough
- Bordetella Pertussis — Main Page
- Pneumonia