Pertussis Resurgence: Waning Immunity and Vaccine Challenges
Pertussis was nearly eliminated in the United States by the 1970s. Today it circulates continuously and sparks large outbreaks every three to five years. Understanding why this happened — and what it means for you and your family — requires looking at how vaccine immunity changes over time, how the bacteria itself is evolving, and what researchers are working on to close the gap.
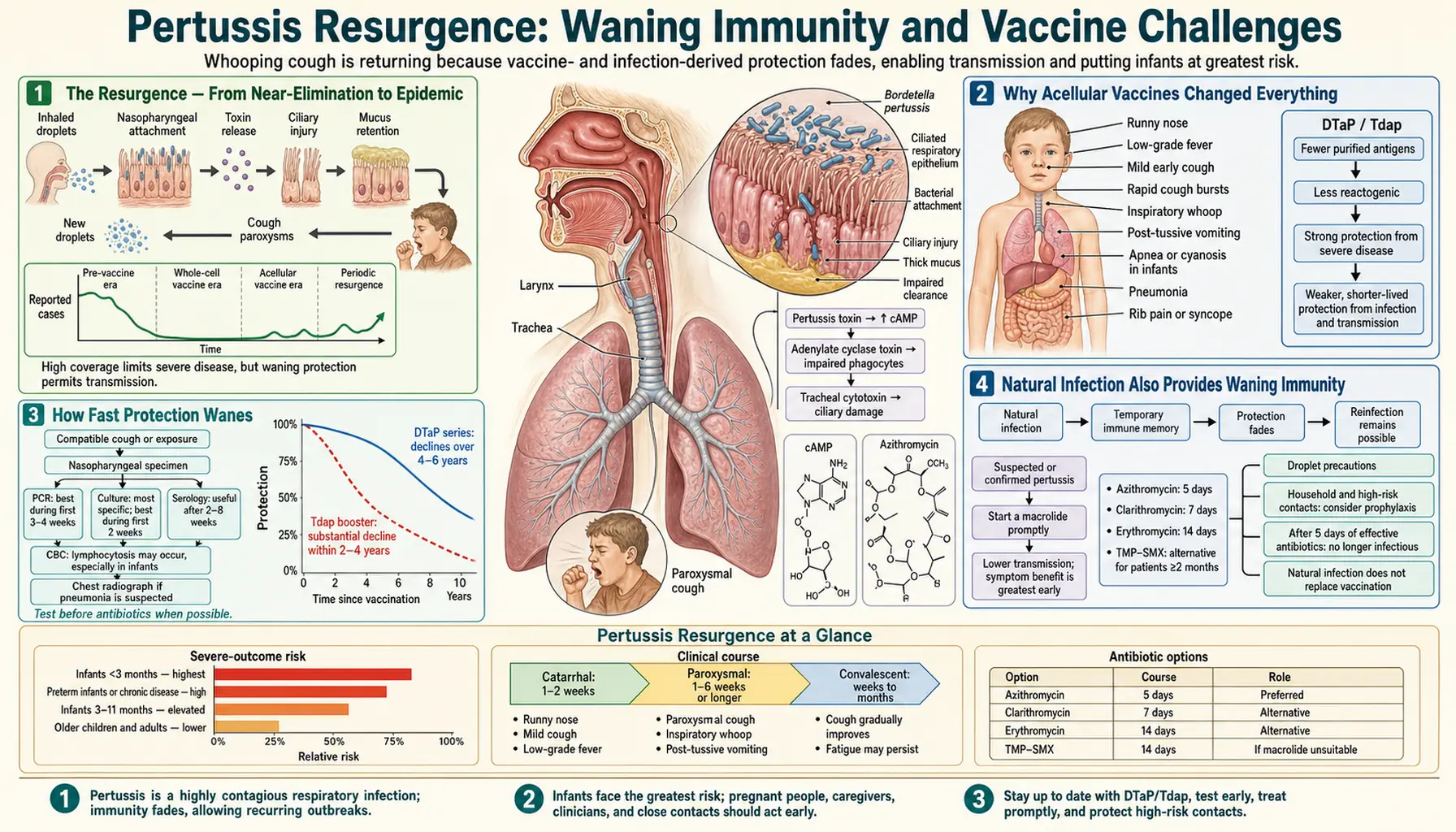
- The Resurgence — From Near-Elimination to Epidemic
- Why Acellular Vaccines Changed Everything
- How Fast Protection Wanes
- Natural Infection Also Provides Waning Immunity
- Antigenic Evolution — Pertactin-Deficient Strains
- Macrolide Resistance — Rare But Emerging
- The Epidemiological Cycle — Outbreaks Every 3–5 Years
- Research Directions — Can We Do Better?
- What You Can Do Now
- Key Research Papers
- Connections
The Resurgence — From Near-Elimination to Epidemic
The numbers tell a striking story. In the late 1970s and early 1980s, when whole-cell pertussis vaccines were in universal use and vaccination rates were high, the United States reported just 1,000 to 2,000 cases per year. Deaths were vanishingly rare.
By 2012, reported cases reached 48,277 — the highest annual total since 1955. California alone saw over 9,000 cases in 2010 and declared a pertussis epidemic. Washington state reported 2,520 cases in the first six months of 2012. Outbreaks occurred in every US state. Similar resurgences were documented in Australia, the United Kingdom, the Netherlands, and other countries that had switched to acellular vaccine formulations.
Crucially, these outbreaks were not primarily driven by unvaccinated populations. Studies consistently showed that the majority of school-age cases occurred in children who had received all five recommended DTaP doses. The vaccine was no longer protecting children as long as had been assumed.
Why Acellular Vaccines Changed Everything
The United States switched from the older whole-cell pertussis vaccine (wP) to the newer acellular pertussis vaccine (aP) between 1991 and 1997. This decision was driven by genuine safety concerns — the whole-cell vaccine caused fever, local pain, and in rare cases more serious adverse events including febrile seizures and hypotonic-hyporesponsive episodes.
Acellular vaccines contain only 2–5 purified pertussis proteins, in contrast to the hundreds of antigens in killed whole bacteria. The safety improvement was real and substantial. However, the immunological trade-off that came with it was not fully appreciated until the outbreaks of the 2010s made it undeniable.
Research in baboon models — primates that develop pertussis disease closely resembling the human illness — demonstrated the core problem. Baboons vaccinated with aP were protected from developing disease, but when exposed to Bordetella pertussis, they could still become colonized and transmit the bacteria to unvaccinated cage-mates. Baboons vaccinated with the older wP formulation resisted colonization far more effectively.
The mechanism lies in the type of immune response generated. The wP vaccine stimulates a broad Th1/Th17 pattern of immunity including mucosal responses in the respiratory tract — the first line of defense against a bacterium that infects airways. The aP vaccine primarily generates a Th2-biased antibody response that reduces disease severity but is less effective at preventing the bacteria from establishing itself in the first place.
How Fast Protection Wanes
Multiple large studies have measured how quickly DTaP and Tdap protection fades, and the findings are consistent and concerning:
- In the first year after the fifth DTaP dose (given at age 4–6 years), effectiveness against laboratory-confirmed pertussis is high — roughly 85–95%.
- Each subsequent year, effectiveness drops by approximately 9–12%.
- By age 11–12, a child who received their last DTaP at age 4–6 may have protection as low as 25–40% — which is why the Tdap booster at 11–12 years is important but also explains why pertussis still circulates in middle-school populations where Tdap has been given.
- Studies of Tdap protection in adolescents show a similar decline. In one large Kaiser Permanente study, effectiveness 1 year after Tdap was about 70%, falling to roughly 45% by 2 years and approaching baseline by 4–5 years.
This rate of waning is dramatically faster than most parents and even many clinicians expect. When people think of vaccines lasting "10 years" or longer, they are often thinking of the durability of the older whole-cell vaccine or of well-characterized vaccines for other diseases. For acellular pertussis, the protection window is measured in years, not decades.
Natural Infection Also Provides Waning Immunity
A common misconception is that getting whooping cough itself provides lifelong immunity — and that therefore natural infection is somehow "better" than vaccination for long-term protection. This is not accurate.
Studies of natural immunity after pertussis infection estimate that protection lasts approximately 4 to 20 years, depending on the individual and the severity of the initial illness. This wide range reflects the difficulty of measuring immunity precisely, but the central finding is clear: natural infection does not provide permanent protection.
Adults who had whooping cough as children — or even as adults — can get it again. In fact, adults are increasingly recognized as an important reservoir of pertussis infection, often presenting with only a prolonged, persistent cough rather than the dramatic whooping that characterizes pediatric cases. Because adults do not look sick enough to be tested, they may spend weeks unknowingly transmitting pertussis to infants and young children in their households.
Antigenic Evolution — Pertactin-Deficient Strains
While waning immunity is the primary driver of the pertussis resurgence, the bacteria itself has also been evolving in ways that may reduce vaccine effectiveness.
Pertactin (PRN) is one of the surface proteins included in most US acellular pertussis vaccines. It helps the bacteria adhere to respiratory epithelial cells and is a target for vaccine-induced antibodies. Beginning in the early 2000s and accelerating through the 2010s, B. pertussis strains that have lost pertactin expression began appearing in clinical isolates.
By 2013, pertactin-deficient strains accounted for more than 80% of US clinical isolates submitted to the CDC. Similar trends were observed in France, Australia, Finland, and the UK — all countries that have used acellular vaccines. This strongly suggests that vaccine-induced selective pressure is driving the evolution of pertactin-deficient strains, since these strains have no survival disadvantage in a population where anti-pertactin antibodies are common.
Whether pertactin-deficient strains are actually more capable of escaping vaccine immunity in practice is still debated. The other antigens in acellular vaccines — particularly pertussis toxin and filamentous hemagglutinin — are still present in circulating strains, and the vaccines may retain meaningful effectiveness against these strains through antibodies to non-pertactin targets. But the evolution is a signal worth watching.
Macrolide Resistance — Rare But Emerging
Macrolide antibiotics — azithromycin, clarithromycin, and erythromycin — are the first-line treatment for pertussis (see the Antibiotic Treatment page). For decades, B. pertussis was uniformly susceptible to macrolides. That began to change in the early 2000s.
Macrolide-resistant B. pertussis has been identified in Iran, China, and France, and sporadic cases have been reported in other countries. The resistance mechanism involves point mutations in the 23S ribosomal RNA gene — the same target site where macrolides bind to block bacterial protein synthesis. Bacteria with these mutations are completely resistant to all macrolides, not just one.
Globally, resistant strains remain uncommon — representing a small fraction of isolates in most surveillance systems. However, the precedent is concerning. Widespread macrolide use for respiratory infections broadly (not just pertussis) creates selection pressure that could amplify resistant strains over time.
The good news is that trimethoprim-sulfamethoxazole (TMP-SMX) remains effective against macrolide-resistant strains because it targets an entirely different bacterial pathway. If macrolide resistance is suspected — for example, in a patient who was treated with azithromycin but is not improving — culture with susceptibility testing and switching to TMP-SMX is the appropriate response.
Clinicians in regions with higher resistance prevalence — particularly Iran and China — should maintain a higher index of suspicion for resistance and consider susceptibility testing routinely.
The Epidemiological Cycle — Outbreaks Every 3–5 Years
Pertussis does not behave like diseases with stable, durable herd immunity. Instead, it follows a predictable cyclical pattern in which cases gradually accumulate in the background, then periodically surge into recognized outbreaks, before subsiding again — not because the bacteria has been eliminated, but because the pool of susceptible individuals has temporarily been reduced by infection and boosted immunity.
Even before the acellular switch, pertussis followed roughly 3–5 year epidemic cycles in the United States. The switch to aP vaccines and the faster waning of immunity have likely contributed to making these cycles more pronounced. The 2010 California epidemic, the 2012 national outbreak, and subsequent surges in 2014 and 2019 fit this pattern.
The implication for public health is sobering: pertussis is not a disease that can be eliminated under the current vaccination paradigm. It will continue to circulate, continue to infect vaccinated people whose immunity has waned, and continue to pose lethal risk to unprotected infants. Outbreak-level surges are expected to continue every several years absent a fundamental change in vaccine technology or strategy.
Research Directions — Can We Do Better?
The scientific community is actively working on multiple fronts to address the limitations of current pertussis vaccines:
- Mucosal vaccines: Vaccines delivered directly to the respiratory tract (as nasal sprays or inhaled formulations) could generate the secretory IgA response in the airways that is missing from injectable acellular vaccines. This type of immune response would directly prevent colonization and transmission. Several candidates are in preclinical and early clinical development.
- Live attenuated pertussis vaccines: Weakened but live B. pertussis strains that could be given intranasally to mimic natural infection are under investigation. A nasal live-attenuated vaccine could generate strong mucosal immunity without causing disease. BPZE1 is the most advanced candidate, with phase 2 trial data showing safety and immunogenicity.
- Return to whole-cell vaccines: Some researchers and public health experts have called for reconsidering wP vaccines for the primary childhood series, arguing that the safety issues were overestimated and the durability benefit is substantial. Several low-income countries never switched from wP and maintain lower pertussis burden as a result. In high-income countries, a hybrid approach — wP for infants, aP for boosters — has been discussed.
- Novel adjuvants: Adding newer adjuvants (immune system stimulants) to the acellular formulation could potentially shift the immune response toward a more Th1/Th17 pattern similar to wP, extending the duration and breadth of protection without returning to the whole-cell approach.
- Maternal vaccination as a bridge: Expanding access to and uptake of Tdap during pregnancy is the intervention with the clearest near-term impact on infant mortality, while longer-lasting vaccine solutions are developed.
What You Can Do Now
While researchers work toward better vaccines, there are concrete steps that protect you and the people around you today:
- Get a Tdap booster if you have not had one in the last five to ten years. Ask your primary care provider or pharmacist — it is available at most pharmacies without an appointment. Most adults only need to ask once; the booster is then due with every Td cycle.
- During pregnancy, get Tdap at 27–36 weeks of every pregnancy — not just your first. This is the most effective way to protect your newborn before they can be vaccinated. Talk to your OB or midwife at your third-trimester appointments.
- Ensure grandparents and other caregivers have received Tdap before spending extended time with a new baby. You are not being overprotective — pertussis kills infants, and this is preventable.
- Do not dismiss a prolonged cough in yourself or an older child. A cough lasting more than two to three weeks — especially with nighttime paroxysms, post-tussive vomiting, or gasping — should be evaluated for pertussis, even in vaccinated individuals. Ask for a PCR test.
- Seek antibiotic treatment promptly if pertussis is suspected or confirmed — even if your cough is already established. Antibiotics during the paroxysmal phase reduce transmission to others and protect the people you live with.
Key Research Papers
- Warfel JM, Zimmerman LI, Merkel TJ. Acellular pertussis vaccines protect against disease but fail to prevent infection. Proc Natl Acad Sci USA. 2014;111(2):787-92. PMID 24277828
- Cherry JD. Epidemic pertussis in 2012. N Engl J Med. 2012;367(9):785-7. — Search PubMed
- Witt MA, et al. Unexpectedly limited durability of immunity following acellular pertussis vaccination. Clin Infect Dis. 2012;54(12):1730-5. PMID 22423127
- Klein NP, et al. Waning protection after fifth dose of acellular pertussis vaccine in children. N Engl J Med. 2012;367(11):1012-9. PMID 22970945
- Tartof SY, et al. Waning immunity to pertussis following 5 doses of DTaP. Pediatrics. 2013;131(4):e1047-52. — Search PubMed
- Pawloski LC, et al. Prevalence and molecular characterization of pertactin-deficient Bordetella pertussis in the United States. Clin Vaccine Immunol. 2014;21(2):119-25. — Search PubMed
- Bouchez V, et al. Characterization and phylogenetic analyses of complete Bordetella pertussis genome sequences. BMC Genomics. 2018;19(1):478. — Search PubMed
- Bodilis H, et al. Multi-drug resistant Bordetella pertussis. Emerg Infect Dis. 2012;18(4):675-7. — Search PubMed
- Kilgore PE, et al. Pertussis: Microbiology, Disease, Treatment, and Prevention. Clin Microbiol Rev. 2016;29(3):449-86. PMID 27029594
- Patel M, et al. Epidemiology of pertussis in the United States. Pediatrics. 2021;147(3):e2020008946. — Search PubMed
- Misegades LK, et al. Association of childhood pertussis with receipt of 5 doses of pertussis vaccine by time since last vaccine dose. JAMA. 2012;308(20):2126-32. — Search PubMed
Connections
- Treatment & Prevention — Overview
- DTaP & Tdap Vaccines
- Antibiotic Treatment
- Symptoms & Whooping Cough
- Bordetella Pertussis — Main Page
- All Bacteria