Whooping Cough: The Three Stages of Pertussis
- The 100-Day Cough Name
- Stage 1: Catarrhal Phase
- Stage 2: Paroxysmal Phase
- Why Vaccinated People Often Don't Whoop
- Stage 3: Convalescent Phase
- Complications During the Paroxysmal Stage
- How Pertussis Looks Different in Teens and Adults
- Lymphocytosis: The Blood Count Clue
- When to See a Doctor
- Key Research Papers
- Connections
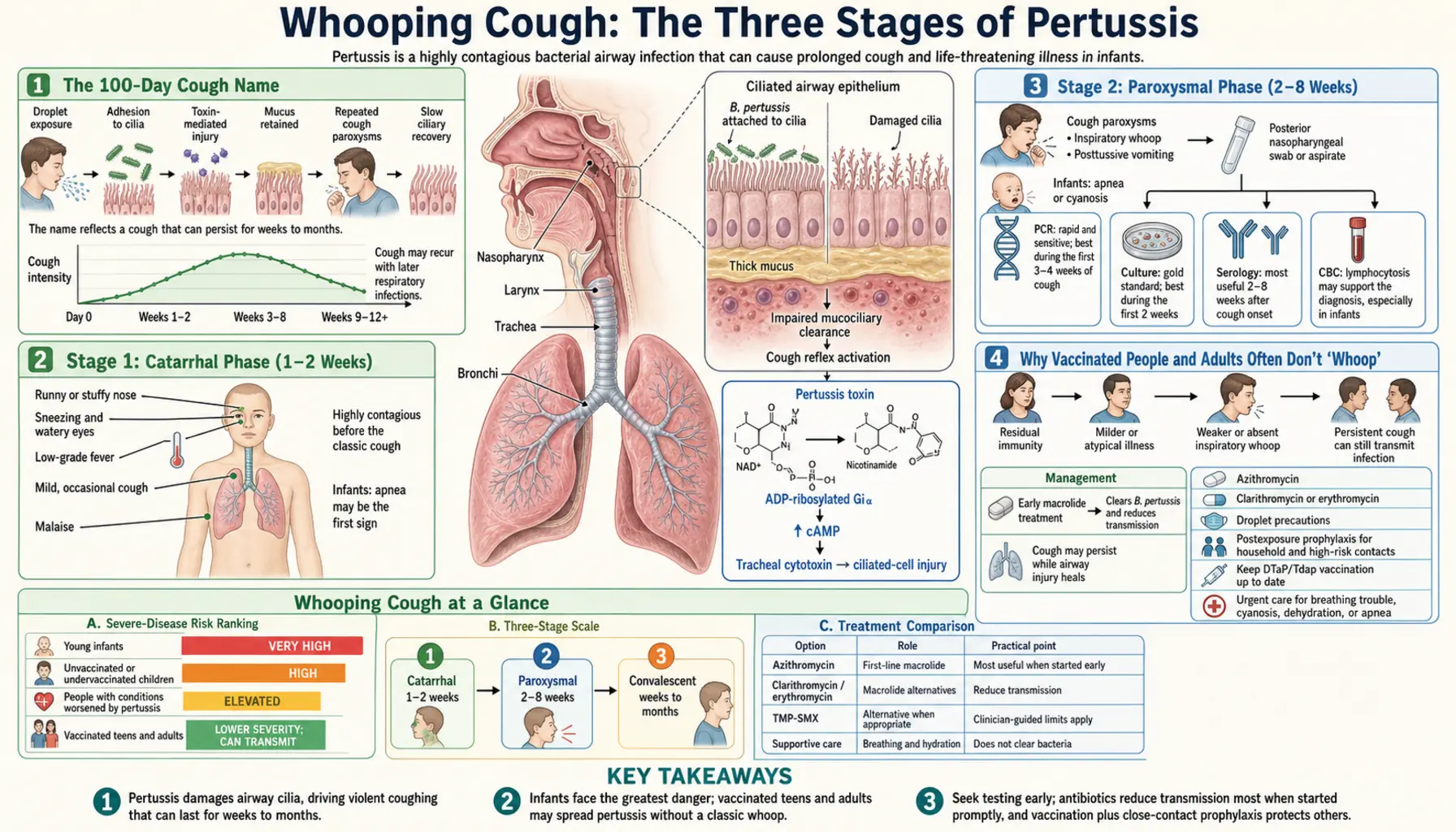
The 100-Day Cough Name
In China, whooping cough has been called "bai ri ke" — the hundred-day cough — for centuries. It is not an exaggeration. From the first sniffle to full recovery, the illness in an unvaccinated adult or teenager routinely lasts 10–14 weeks. Even in vaccinated people who get a milder version, the cough frequently persists for 6–8 weeks.
The reason the cough lasts so long is that Bordetella pertussis physically damages the cilia lining the airways. These tiny hair-like projections normally beat in coordinated waves to sweep mucus and particles up and out of the lungs. After a pertussis infection, even when the bacteria are killed by antibiotics or cleared by the immune system, the cilia take weeks to months to fully regrow and function normally. Until they do, the airway remains hypersensitive, and almost anything — cold air, laughing, exercise, another respiratory virus, even a sudden smell — can trigger another violent coughing fit.
Understanding the three distinct stages of pertussis helps explain why the disease is so often misdiagnosed, why antibiotics are only helpful in the first two weeks, and why some symptoms are so much more dangerous than others.
Stage 1: Catarrhal Phase (1–2 Weeks)
The catarrhal phase is named for the thick mucus (catarrh) that characterizes it. In practice, it looks almost exactly like a common cold:
- Runny nose (rhinorrhea), often clear and watery
- Mild, intermittent cough that gradually increases in frequency
- Watery, red eyes (conjunctival injection)
- Possibly a low-grade fever — but fever is often absent or minimal
- General feeling of being unwell, but not acutely ill
The deceptive mildness of this stage is what makes pertussis so dangerous from a public health standpoint. The infected person feels well enough to go to work, school, or social gatherings — and this is precisely when they are most contagious. Bacterial counts in the nasopharynx peak in the catarrhal phase, before coughing is even severe. Studies have shown that most infants who develop serious pertussis were infected by a parent, sibling, or other household contact who thought they just had a lingering cold.
Antibiotics given in the catarrhal phase can shorten or even abort the illness. This is the treatment window that matters — but it is almost never used, because no one yet suspects pertussis.
Stage 2: Paroxysmal Phase (2–8 Weeks)
The transition from catarrhal to paroxysmal stage is unmistakable once it happens. The cough changes character completely. Instead of a single cough, the person experiences a paroxysm: a sudden, uncontrollable burst of many rapid coughs — sometimes 10 to 30 or more in a single exhalation — until all the air is gone from the lungs.
Then comes the defining moment: the person takes a desperate gasping breath through a partially closed larynx (voice box), and the air rushing through produces the characteristic high-pitched, crowing "whoop" sound that gives the disease its name. Many patients describe the sensation as feeling like they are choking or suffocating during the paroxysm.
Key features of the paroxysmal phase include:
- Post-cough vomiting: The forceful coughing frequently triggers the gag reflex. Infants and young children often vomit after coughing fits, which can contribute to dehydration and weight loss.
- Cyanosis: Turning blue or purple around the lips and face during severe paroxysms due to oxygen deprivation. This is an emergency in any infant.
- Frequency: Paroxysms may occur 10–30+ times per day, often clustering at night.
- Exhaustion after attacks: After a particularly severe paroxysm, the person may look dazed, limp, and exhausted. In young children, this can be alarming to witness.
- Between attacks, the person appears relatively normal: This is actually an important diagnostic clue — pertussis patients often look surprisingly well between coughing episodes.
A complete blood count (CBC) drawn during the paroxysmal phase typically shows a striking rise in lymphocytes — often 10,000–30,000/μL in teenagers and adults, and potentially much higher in infants. This lymphocytosis is a direct effect of pertussis toxin on the immune system.
Why Vaccinated People and Adults Often Don't "Whoop"
A common and clinically important misconception is that if there is no "whoop," the person does not have pertussis. This is wrong, and it causes the disease to be missed in exactly the populations most likely to spread it to infants.
The classic whooping sound requires two things: a large enough volume of airway to create turbulent airflow, and a forceful enough inspiratory effort to produce the sound. Young children with smaller, more compliant airways and greater respiratory effort relative to their size are most likely to produce the classic whoop.
Vaccinated older children, teenagers, and adults have:
- Partial immunity that blunts the severity of the paroxysms
- Larger airways where turbulent flow is less pronounced
- A pattern that often presents instead as a prolonged, dry, hacking cough lasting 3–12 weeks
In this population, pertussis is routinely misdiagnosed as bronchitis, post-nasal drip, asthma, or a lingering viral upper respiratory infection. Studies have shown that pertussis is the cause in approximately 20–30% of adults with a cough lasting more than 3 weeks in areas with active pertussis circulation. Many see multiple doctors before the correct diagnosis is made — if it is made at all.
Stage 3: Convalescent Phase (Weeks to Months)
The convalescent (recovery) phase begins when the paroxysms gradually become less frequent and less severe. This improvement is welcome but slow. The cough typically takes 10–12 weeks from the start of illness to fully resolve in adults and older children, and in some people can persist for 4–6 months.
The most frustrating aspect of the convalescent phase is that the airway remains irritable long after the bacteria are gone. Any respiratory irritant can trigger a full return of paroxysmal coughing — another respiratory infection (especially a common cold), cold air, exercise, smoke, strong odors, or even laughing hard. Many patients report being taken by surprise months after the original illness when a new cold triggers paroxysms again.
During this phase, the person is generally no longer contagious (after completing antibiotic treatment or after 3 weeks of cough onset). The continuing cough is from ciliary damage and airway hypersensitivity, not from active bacterial infection. No further antibiotic treatment is helpful at this stage.
Complications During the Paroxysmal Stage
The violent, prolonged paroxysms of the second stage create mechanical stress throughout the body and can lead to a range of complications:
- Rib fractures: The force of severe coughing fits can fracture ribs, particularly in adults and elderly patients.
- Petechiae and subconjunctival hemorrhages: Tiny broken blood vessels appear as red dots under the eyes or on the face from the pressure of coughing.
- Syncope (fainting): Reduced blood flow to the brain during prolonged paroxysms can cause loss of consciousness.
- Hernias: Abdominal or inguinal hernias can develop or worsen from sustained coughing pressure.
- Urinary incontinence: Common in adult women during severe coughing fits.
- Pneumonia: The leading serious complication, occurring in about 1 in 100 cases overall and at much higher rates in infants. Can be caused by secondary bacterial infection or by direct pertussis bronchopneumonia.
- Encephalopathy: Rare but devastating brain damage from hypoxia during severe attacks or from pertussis toxin effects; more common in infants than older patients.
How Pertussis Looks Different in Teens and Adults vs Young Children
The clinical picture varies substantially by age group, and recognizing these differences is key to not missing the diagnosis:
Young unvaccinated children (classic disease): The full three-stage illness with classic paroxysms, the inspiratory whoop, post-cough vomiting, and possible cyanosis. Worst disease severity in this group among those who are unvaccinated.
Adolescents (most underdiagnosed group): Prolonged dry cough of 3–10 weeks duration. The whoop may or may not be present. Post-cough vomiting is less common. The cough is often worse at night. Most are vaccinated but their immunity has waned. They frequently have no fever and feel well otherwise, making them reluctant to see a doctor. Yet this group is a major reservoir driving infections in vulnerable infants.
Adults (frequently dismissed): Similar to adolescents — persistent cough of weeks to months, often without classic features. Multiple doctor visits before diagnosis. May be told they have bronchitis, allergies, or post-nasal drip. One large study found pertussis in 26% of adults with cough lasting over 2 weeks presenting to emergency departments during a local outbreak.
Lymphocytosis: The Blood Count Clue
One of the most distinctive laboratory findings in pertussis is lymphocytosis — an elevated count of lymphocytes (a type of white blood cell). This occurs because pertussis toxin blocks the receptors that lymphocytes need to enter lymph nodes and tissues, so they pile up in the bloodstream instead of going where they should.
In typical adult pertussis during the paroxysmal stage, a routine CBC may show:
- Total white blood cell count: 15,000–30,000/μL (normal upper limit roughly 11,000)
- Differential showing 60–80% lymphocytes (absolute lymphocyte count often exceeding 10,000/μL)
In severe infant cases, the numbers can be catastrophic:
- Total white cell count: 50,000–100,000/μL or higher
- Predominantly lymphocytes
This extreme lymphocytosis in infants is not just a laboratory curiosity — the excess lymphocytes accumulate in the small blood vessels of the lungs, causing pulmonary hypertension (high blood pressure in the lung circulation). This can lead to right-sided heart failure and is one of the primary mechanisms of death in severe infant pertussis. When a doctor sees a CBC showing a white cell count above 50,000/μL in a sick infant, pertussis should be at the top of the differential diagnosis.
When to See a Doctor
See a doctor promptly if:
- A cough has lasted more than 2 weeks, especially if it comes in bursts or is followed by vomiting
- You or your child has been in contact with someone confirmed to have pertussis
- An infant (especially under 6 months) has any new cough — don't wait to see if it gets worse
- The cough is followed by the "whoop" sound or by vomiting
- An infant stops breathing or turns bluish during a cough
- A cough is interfering significantly with sleep every night for more than a week
If you are prescribed antibiotics for pertussis, finish the full course even if you feel better. And if you are caring for an infant under 6 months, ask your doctor about preventive antibiotics (post-exposure prophylaxis) for everyone in the household who may have been exposed, and make sure your own Tdap booster is current.
Key Research Papers
- Cherry JD. The history of pertussis (whooping cough); 1906–2015: facts, myths, and misconceptions. Curr Epidemiol Rep. 2015;2(2):120–130. — Search PubMed
- Halperin SA. The control of pertussis — 2007 and beyond. N Engl J Med. 2007;356(2):110–3. — Search PubMed
- Guinto-Ocampo H, et al. Predicting pertussis in infants. Pediatr Emerg Care. 2008;24(1):16–20. — Search PubMed
- Carbonetti NH. Pertussis leukocytosis: mechanisms, clinical implications and treatment considerations. Curr Opin Infect Dis. 2016;29(3):257–64. — Search PubMed
- Mattoo S, Cherry JD. Molecular pathogenesis, epidemiology, and clinical manifestations. Clin Microbiol Rev. 2005;18(2):326–82. PMID 15831828
- Kilgore PE, et al. Pertussis: Microbiology, Disease, Treatment, and Prevention. Clin Microbiol Rev. 2016;29(3):449–86. PMID 27029594
- Liu BC, et al. Whooping cough in adults: a systematic review. J Clin Med. 2021;10(9):1988. — Search PubMed
- Bhatt KA, et al. Pertussis: what the practicing clinician needs to know. Cleve Clin J Med. 2022;89(4):218–225. — Search PubMed
- Patel M, et al. Epidemiology of pertussis in the United States. Pediatrics. 2021;147(3):e2020008946. — Search PubMed
- Witt MA, et al. Unexpectedly limited durability of immunity following acellular pertussis vaccination in pre-adolescents in a North American outbreak. Clin Infect Dis. 2012;54(12):1730–5. PMID 22423127
Connections
- Bordetella pertussis Symptoms Hub
- Pertussis in Newborns and Young Infants
- Diagnosing Pertussis: PCR, Culture, and Serology
- Whooping Cough — the full disease page around this staging — epidemiology and waning acellular-vaccine immunity, azithromycin treatment and post-exposure prophylaxis, infant complications, and Tdap in pregnancy.
- Treatment and Prevention of Pertussis
- Bordetella pertussis Overview
- Pneumonia
- All Bacteria Diseases