DTaP and Tdap Vaccines: Protecting Against Whooping Cough
Vaccination is the cornerstone of pertussis prevention. Two vaccines are in use today — DTaP for children and Tdap for adolescents and adults — and together they protect people across the lifespan. But immunity fades faster than most people realize, and understanding when boosters are needed — especially during pregnancy — can literally save an infant's life.
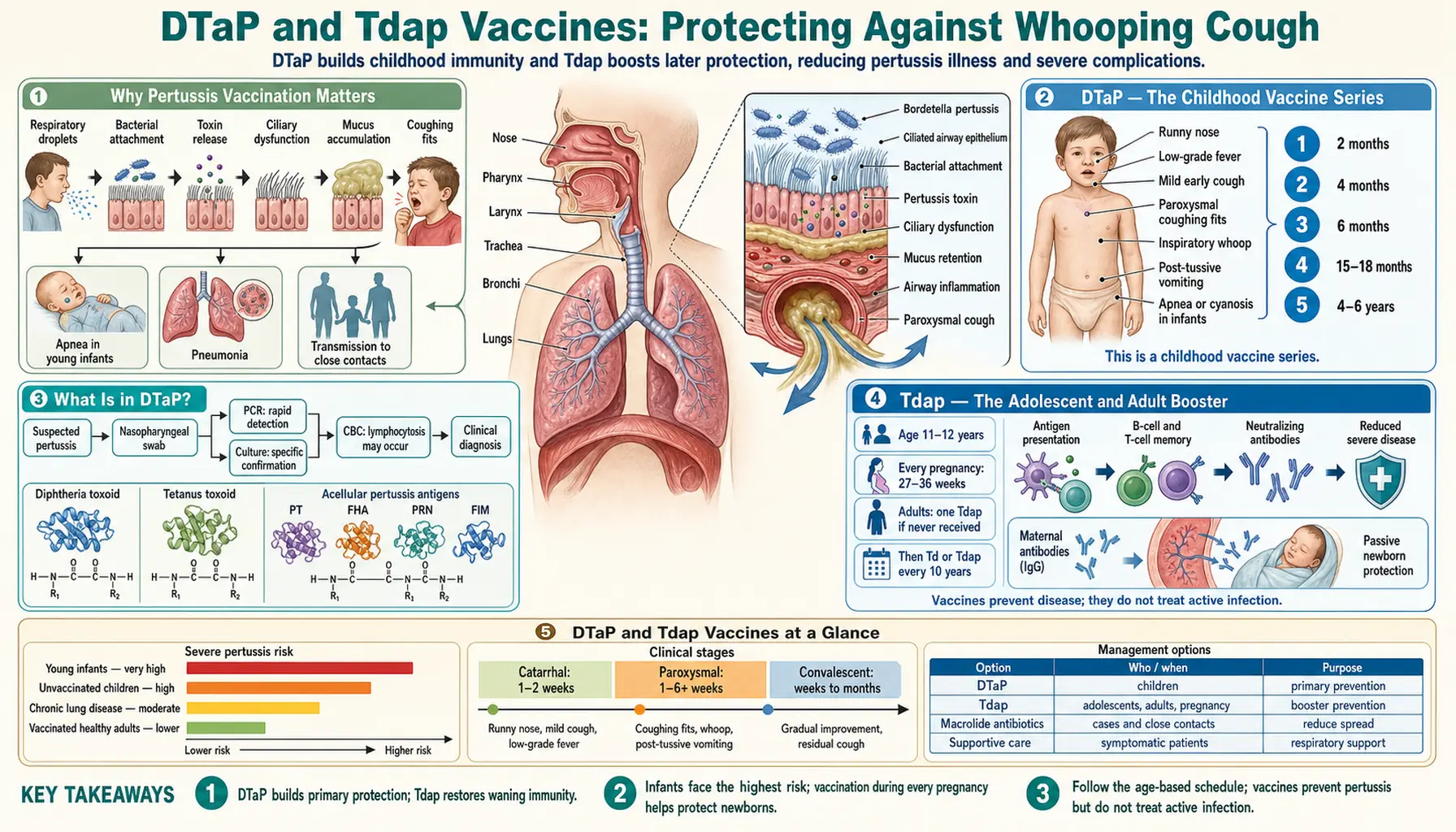
- Why Pertussis Vaccination Matters
- DTaP — The Childhood Vaccine Series
- What Is in DTaP?
- Tdap — The Adolescent and Adult Booster
- Tdap in Pregnancy — The Critical Strategy
- The Cocooning Strategy
- Healthcare Worker Tdap
- Acellular vs. Whole-Cell Vaccines — The Durability Trade-Off
- Vaccine Effectiveness Data
- Key Research Papers
- Connections
Why Pertussis Vaccination Matters
Before vaccines existed, pertussis was one of the most feared childhood diseases in the United States. In the pre-vaccine era, the country recorded between 150,000 and 260,000 cases every year, with an estimated 5,000 to 9,000 deaths annually — the vast majority in infants under 12 months who could not survive the violent, suffocating coughing fits or the pneumonia that followed.
The introduction of the whole-cell pertussis vaccine in the 1940s, combined into the DTP shot with diphtheria and tetanus toxoids, drove a more than 99% decline in reported cases over the following decades. At their lowest, annual US case counts fell below 1,000 in the late 1970s and 1980s, and pertussis deaths became rare.
However, pertussis has rebounded significantly since the late 1990s. The 2012 outbreak produced 48,277 reported cases — the highest since 1955. Multiple factors drive this resurgence, including waning vaccine immunity and changes in the vaccine formulation (discussed in detail in the Waning Immunity page), but the fundamental protection that vaccines provide remains real and important. Without ongoing vaccination, the disease would return to its pre-vaccine toll.
DTaP — The Childhood Vaccine Series
Children in the United States receive five doses of the DTaP vaccine as part of their routine immunization schedule:
- Dose 1: 2 months of age
- Dose 2: 4 months of age
- Dose 3: 6 months of age
- Dose 4: 15–18 months of age
- Dose 5: 4–6 years of age (before starting school)
Each letter in DTaP tells you something about the vaccine's contents. D stands for diphtheria toxoid. T stands for tetanus toxoid. The lower-case a stands for acellular — meaning the pertussis component uses purified pieces of the bacteria rather than the whole killed organism. And P stands for pertussis.
The five-dose schedule is designed around how the infant immune system develops. The first three doses build the foundation of immunity; the fourth dose at 15–18 months consolidates it; and the fifth dose before school entry restores protection that has naturally waned over the preceding years.
No single dose provides complete protection. A child who misses one or more doses is at significantly higher risk. If your child's schedule has fallen behind, talk to your pediatrician about a catch-up plan — it is never too late to get back on track.
What Is in DTaP?
The "acellular" pertussis component is fundamentally different from the older whole-cell pertussis vaccine that was used until the mid-1990s. Instead of containing killed whole bacteria — which carried all the bacterial proteins plus lipopolysaccharide (LPS), a potent stimulator of inflammation — acellular vaccines contain just two to five highly purified pertussis proteins.
The specific proteins included depend on the vaccine brand:
- Pertussis toxin (PT): Included in all DTaP vaccines. PT is the primary toxin responsible for many of pertussis's systemic effects, including immune system suppression. Neutralizing antibodies against PT are central to protection.
- Filamentous hemagglutinin (FHA): An adhesin — a protein the bacteria uses to stick to respiratory cells. Included in all US DTaP formulations.
- Pertactin (PRN): Another surface adhesin. Included in most formulations. Of particular concern because strains that have lost pertactin production are now common (see Waning Immunity page).
- Fimbriae types 2 and 3 (FIM 2/3): Hair-like structures used for attachment. Included in Daptacel (Sanofi) but not Infanrix (GSK).
The acellular approach produces fewer and milder side effects — less fever, redness, and soreness at the injection site — which improved vaccine acceptance among parents. However, the reduced immune stimulation also means the immunity generated does not last as long as the older whole-cell formulation.
Tdap — The Adolescent and Adult Booster
Tdap is essentially a reduced-dose version of DTaP. The lower-case letters are not a typo — they indicate that this formulation contains a lower quantity of diphtheria and pertussis antigens than the childhood DTaP. The full-dose formulation was not needed (and caused more side effects) in older immune systems that have already been primed by the childhood series.
In the United States, two Tdap brands are available: Adacel (Sanofi, approved for ages 10 through 64) and Boostrix (GSK, approved for ages 10 and older). Both are approved for a single dose in adolescents and adults.
The standard CDC recommendation is:
- One Tdap dose at age 11–12 years, ideally at the pre-teen well-child visit, replacing one Td (tetanus-diphtheria) booster
- Adults who have never received Tdap: one dose, followed by Td boosters every 10 years
- An additional Tdap can substitute for any Td booster if you are due for one and have not had Tdap recently
Adults who received only DTP (the older whole-cell formulation) as children did not receive the acellular pertussis component. A Tdap dose provides them with their first acellular pertussis vaccination as adults.
Tdap in Pregnancy — The Critical Strategy
Of all pertussis prevention strategies currently available, maternal Tdap vaccination during pregnancy has the strongest evidence base for protecting infants in their first months of life — before they can complete their own vaccine series.
The CDC recommends Tdap at 27 to 36 weeks of every pregnancy, not just the first. The reason this window matters so much is the biology of placental antibody transfer. During the third trimester — especially weeks 30 through 36 — the placenta actively and efficiently pumps maternal immunoglobulin G (IgG) antibodies across to the fetus. A mother vaccinated at 27–36 weeks generates a peak antibody response just in time for large amounts of pertussis-specific IgG to cross to her baby. The newborn then enters the world already carrying maternal antibodies that can neutralize the bacteria and its toxins.
Clinical trial data from the UK, where maternal Tdap was implemented as a national program after a 2012 outbreak, showed vaccine effectiveness of approximately 91% against laboratory-confirmed pertussis in infants under 3 months born to vaccinated mothers. These are infants who would otherwise have zero vaccine-derived protection at the age they are most vulnerable to dying from pertussis.
The vaccine is safe during pregnancy. Large studies have found no increased risk of preterm birth, low birth weight, stillbirth, or other adverse outcomes associated with maternal Tdap. The recommendation applies to each pregnancy — because maternal antibody levels wane over time, vaccination in one pregnancy does not reliably protect a baby born two or three years later.
The Cocooning Strategy
Before maternal vaccination was studied and widely recommended, public health authorities promoted a strategy called cocooning: vaccinating everyone who would be in close contact with the newborn — parents, siblings, grandparents, and other regular caregivers — in order to surround the baby with protected people who could not transmit the infection.
Cocooning is logistically challenging and, in practice, less effective than maternal vaccination. Studies have shown mixed results, in part because it is difficult to ensure that all contacts are vaccinated before the baby arrives, and in part because the infant's greatest risk often comes from parents, who may transmit the disease before their post-birth Tdap takes effect.
That said, cocooning still makes sense as a complementary strategy. If you are a new parent, grandparent, sibling, or caregiver who has not received Tdap within the last five to ten years, getting vaccinated before (or as soon as possible after) the baby arrives is a worthwhile step. Ask your primary care provider or pharmacist — Tdap is widely available.
Healthcare Worker Tdap
Healthcare workers are at elevated risk of exposure to pertussis and can easily transmit it to vulnerable patients — especially in newborn nurseries, NICUs, and pediatric units. A single unprotected healthcare worker with pertussis may expose dozens of patients and colleagues.
Most US hospital systems require Tdap as a condition of employment. The CDC Advisory Committee on Immunization Practices (ACIP) recommends that healthcare workers who have not received Tdap as an adult receive a single dose, regardless of prior Td vaccination history or interval since the last Td dose.
Healthcare settings have been the source of pertussis outbreaks on multiple occasions. In one notable NICU outbreak, an infected nurse transmitted pertussis to multiple newborns before the source was identified. Institutional Tdap requirements exist precisely to prevent such events.
Acellular vs. Whole-Cell Vaccines — The Durability Trade-Off
The United States switched from the whole-cell pertussis vaccine (wP) to the acellular pertussis vaccine (aP) beginning in 1991 for children 15 months and older, completing the transition by 1997 for all doses. Several other high-income countries made the same switch around the same time.
The whole-cell vaccine worked by exposing the immune system to entire killed Bordetella pertussis bacteria, including all their surface proteins, toxins, and the inflammatory lipopolysaccharide outer membrane. This broad immune stimulus generated strong, long-lasting immunity — but it also caused fever, significant local pain and swelling at the injection site, and in rare cases, more serious adverse events including febrile seizures. Public concern about these side effects drove demand for a safer alternative.
The acellular vaccines are far safer and better tolerated. Serious adverse events are extremely rare. However, research in animal models (particularly baboons, which develop pertussis disease similar to humans) has demonstrated that while aP vaccines prevent disease symptoms, they do not prevent airway colonization and transmission as effectively as wP. A baboon vaccinated with aP can still carry and shed the bacteria, silently spreading pertussis to unvaccinated contacts.
This difference in mucosal immunity — the ability to prevent the bacteria from colonizing the respiratory tract in the first place — is now understood to be central to the waning effectiveness seen in human populations. The immune system's response to aP is dominated by circulating antibodies that reduce disease severity, rather than the mucosal IgA responses that prevent colonization and transmission.
Vaccine Effectiveness Data
Real-world effectiveness estimates for DTaP and Tdap vary across studies, but the overall pattern is consistent: protection is strong shortly after vaccination and declines meaningfully over the following years.
- In the first year after completing the childhood DTaP series, effectiveness against laboratory-confirmed pertussis in children is approximately 85–95%.
- By 5 years after the last DTaP dose, effectiveness may decline to 70–80% — and for some studies looking at the fifth dose at ages 4–6, protection drops to roughly 25–40% by the time children are approaching middle school.
- After a Tdap booster in adolescents, effectiveness is high initially but wanes at a similar rate. Studies from Kaiser Permanente and other systems estimate about a 9% per year decline in effectiveness after Tdap.
- By 8–10 years after Tdap, a significant portion of adolescents and adults have limited protection remaining — which is why Td boosters every 10 years are recommended, and why substituting Tdap for one of those boosters matters.
These numbers are not an argument against vaccination — they are an argument for understanding its limits and not relying on vaccine-induced immunity to protect the most vulnerable newborns. The combination of maintaining vaccine schedules, boosting during pregnancy, and seeking prompt antibiotic treatment when pertussis is suspected remains the most effective strategy currently available.
Key Research Papers
- Witt MA, et al. Unexpectedly limited durability of immunity following acellular pertussis vaccination in pre-adolescents. Clin Infect Dis. 2012;54(12):1730-5. PMID 22423127
- Warfel JM, Zimmerman LI, Merkel TJ. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission. Proc Natl Acad Sci USA. 2014;111(2):787-92. PMID 24277828
- Amirthalingam G, et al. Effectiveness of maternal pertussis vaccination in England. Lancet. 2014;384(9953):1521-8. PMID 25037990
- Gall SA, et al. Maternal immunization with tetanus-diphtheria-pertussis vaccine. Obstet Gynecol. 2011;118(4):795-802. — Search PubMed
- Gkentzi D, et al. Maternal vaccination against pertussis. Arch Dis Child Fetal Neonatal Ed. 2017;102(5):F456-F463. — Search PubMed
- Klein NP, et al. Waning protection after fifth dose of acellular pertussis vaccine in children. N Engl J Med. 2012;367(11):1012-9. PMID 22970945
- Misegades LK, et al. Association of childhood pertussis with receipt of 5 doses of pertussis vaccine by time since last vaccine dose. JAMA. 2012;308(20):2126-32. — Search PubMed
- Kilgore PE, et al. Pertussis: Microbiology, Disease, Treatment, and Prevention. Clin Microbiol Rev. 2016;29(3):449-86. PMID 27029594
- Cherry JD. The history of pertussis vaccination. Curr Epidemiol Rep. 2015;2(2):120-130. — Search PubMed
- Plotkin SA. Complex correlates of protection after vaccination. Clin Infect Dis. 2013;56(10):1458-65. PMID 23386629
Connections
- All Bacteria
- Treatment & Prevention — Overview
- Antibiotic Treatment
- Waning Immunity and Antibiotic Resistance
- Pertussis in Infants
- Bordetella Pertussis — Main Page