Leucine for Sarcopenia Prevention
Sarcopenia — the age-related loss of muscle mass, strength, and function — is the single most reversible driver of frailty, falls, fractures, and loss of independence in older adults. The phenomenon of "anabolic resistance" characterized by Elena Volpi and colleagues explains why elderly muscle requires substantially more per-meal leucine to mount a comparable protein-synthesis response than young muscle does. The Bauer PROVIDE trial (and the broader PRO-AGE consensus) established that 30 g of high-quality protein per meal — or equivalent leucine-enriched whey supplementation — reliably restores anabolic signaling in the elderly. Leucine's direct metabolite HMB (beta-hydroxy-beta-methylbutyrate) has its own substantial trial literature in elderly muscle preservation. This deep-dive walks through the biology of anabolic resistance, the per-meal protein recommendations that emerged from the Bauer/PROT-AGE work, the role of leucine-enriched whey in clinical practice, and the HMB evidence base from the Steve Nissen and Jeff Wilson research programs.
Table of Contents
- What Sarcopenia Is and Why It Matters
- Anabolic Resistance — the Volpi Findings
- The Bauer PROVIDE Trial
- PROT-AGE Per-Meal Recommendations
- Leucine-Enriched Whey for the Elderly
- HMB — Leucine's Anti-Catabolic Metabolite
- The Wilson HMB Trial Series
- Resistance Exercise as the Required Co-Intervention
- Practical Clinical Protocols
- Contraindications and Special Populations
- Key Research Papers
- Connections
- Featured Videos
What Sarcopenia Is and Why It Matters
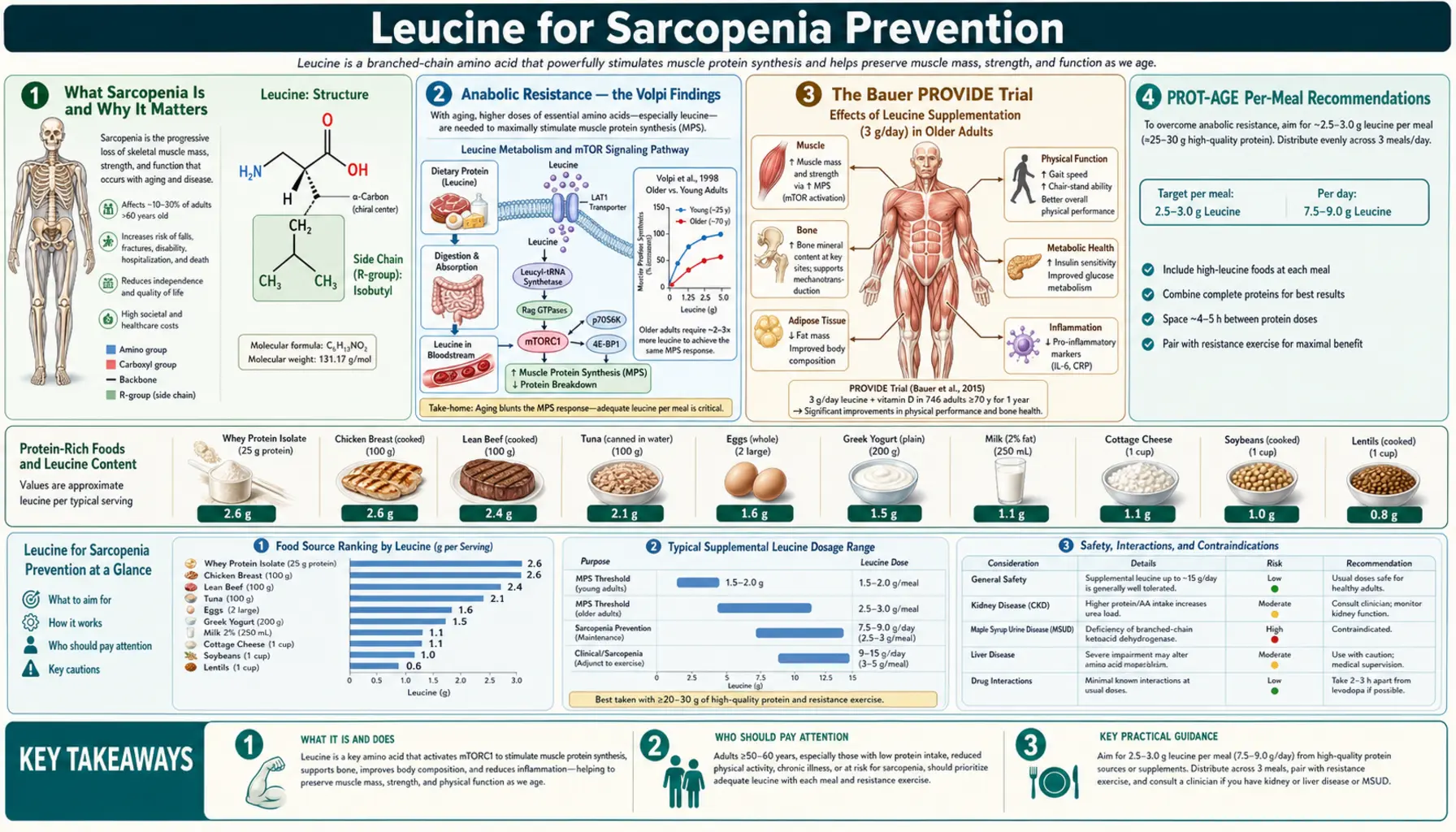
Sarcopenia is the involuntary loss of skeletal muscle mass, strength, and physical performance that accompanies aging. The European Working Group on Sarcopenia in Older People (EWGSOP2) consensus defines sarcopenia by three criteria: low muscle strength (the primary criterion, measured by grip strength <27 kg in men or <16 kg in women, or chair-stand time >15 seconds for 5 stands), low muscle quantity or quality (appendicular skeletal muscle mass index by DXA <7.0 kg/m² in men, <5.5 kg/m² in women), and low physical performance (gait speed ≤0.8 m/s).
The clinical consequences are large. Sarcopenic individuals have a doubled risk of falls, a tripled risk of fractures after a fall, a doubled risk of being unable to live independently, a doubled risk of post-surgical complications, and approximately a doubled all-cause mortality risk compared to non-sarcopenic peers of the same chronological age. The economic burden in the United States alone is estimated at $19 billion per year in direct healthcare costs (Janssen et al., 2004 estimates updated for inflation), and the personal cost in lost autonomy and quality of life is incalculable.
Trajectory: adults lose approximately 3–8% of muscle mass per decade after age 30, with the rate accelerating after age 60 and again after age 75. By age 80, a sedentary adult has typically lost 30–40% of the muscle mass they had at age 25. The loss is concentrated in the type II (fast-twitch) fibers that produce explosive power — the fibers most relevant to recovery from a stumble or fall — making the functional decline disproportionate to the mass loss.
The good news: sarcopenia is largely a disease of disuse and undernutrition, not a hardwired biological inevitability. Master athletes (60-, 70-, 80-year-olds who continue regular resistance training and maintain adequate protein intake) retain 80–90% of the muscle mass they had at age 30. Nursing-home residents who begin a resistance training program can build measurable muscle and strength even into their nineties. The biological capacity for adaptation persists; the modifiable input is the combination of mechanical loading and adequate amino acid stimulus.
Anabolic Resistance — the Volpi Findings
The phenomenon of "anabolic resistance" was systematically characterized by Elena Volpi's group at the University of Texas Medical Branch in a series of stable-isotope tracer studies in healthy young and elderly subjects beginning in the late 1990s. The core finding: an identical essential amino acid stimulus produces a smaller muscle protein synthesis response in older adults than in younger adults — even when the older adults are otherwise healthy, weight-stable, and free of inflammatory disease.
The Volpi 2000 paper (Journal of Clinical Endocrinology and Metabolism) demonstrated that a 40 g essential amino acid bolus produced approximately 50% less increase in muscle protein synthesis in older subjects (mean age 71) than in younger subjects (mean age 29). The blunted response was specific to the muscle — whole-body protein turnover did not differ between age groups, indicating that the defect was in the muscle's response to amino acids rather than in absorption or systemic delivery.
Mechanistically, anabolic resistance involves multiple converging defects. Reduced perfusion: insulin-mediated muscle vasodilation declines with age, reducing amino acid delivery to muscle tissue per unit of plasma amino acid concentration. Reduced mTORC1 signaling: at any given amino acid concentration, older muscle generates a smaller phosphorylation response in S6K1 and 4E-BP1. Reduced satellite cell pool: the muscle stem cells responsible for hypertrophy decline in number and activation capacity with age. Reduced ribosomal capacity: older muscle has fewer ribosomes per fiber and lower ribosome biogenesis in response to anabolic stimuli. Increased inflammation: low-grade chronic inflammation in older adults (the "inflammaging" phenomenon) elevates TNF-alpha and IL-6, both of which directly suppress mTORC1 signaling.
The Cuthbertson and Rennie 2005 FASEB Journal paper showed that the dose-response curve for anabolic resistance is shifted right and flattened: where young muscle reaches half-maximal MPS at approximately 1.5 g of leucine, old muscle requires approximately 2.5 g; where young muscle plateaus at approximately 2.5 g, old muscle requires approximately 3.5 g to plateau. The practical implication is that elderly anabolic resistance can be largely overcome by raising per-meal leucine, but the dose needed is meaningfully higher than for young muscle.
The Bauer PROVIDE Trial
The PROVIDE study (Bauer et al., JAMDA 2015) is the most influential single trial of leucine-enriched supplementation for sarcopenia. The design enrolled 380 sarcopenic older adults (mean age 77.7 years) and randomized them to receive either a leucine-enriched whey-based supplement (20 g whey protein, 3 g total leucine, 800 IU vitamin D, plus essential micronutrients) twice daily, or an isocaloric placebo, for 13 weeks. Neither group received structured exercise training.
Primary endpoints were change in appendicular muscle mass (by DXA) and change in handgrip strength. Secondary endpoints included Short Physical Performance Battery (SPPB) scores and chair-stand performance.
Results were striking. The supplement group gained mean 0.17 kg of appendicular muscle mass over 13 weeks while the placebo group lost mean 0.14 kg — a between-group difference of 0.31 kg favoring supplementation (p<0.01). Chair-stand time improved significantly more in the supplement group. Handgrip strength showed a non-significant trend favoring supplementation. The leucine-enriched whey was well-tolerated with no excess adverse events compared to placebo.
What makes PROVIDE compelling is that the muscle gain occurred without exercise training — the supplement alone produced a measurable anabolic response in sarcopenic elderly adults. This is the strongest single-trial evidence that nutritional intervention can independently shift the trajectory of sarcopenia. The effect size is modest in absolute terms but large in clinical significance — preventing the natural loss of 0.14 kg over 13 weeks projects to preventing approximately 1.1 kg of loss over 2 years, the difference between maintaining and falling below the sarcopenia diagnostic threshold for many elderly patients.
Subsequent trials have replicated the PROVIDE finding in different populations. The PROT-AGE and ESPEN expert groups have incorporated leucine-enriched whey-based nutritional supplementation into their consensus recommendations for sarcopenia management.
PROT-AGE Per-Meal Recommendations
The PROT-AGE study group consensus (Bauer et al., JAMDA 2013) issued the most influential per-meal protein recommendations for older adults, explicitly grounded in the leucine threshold biology. Their key recommendations:
- Total daily protein intake of 1.0–1.2 g per kg body weight per day for healthy older adults, with higher intake (1.2–1.5 g/kg/day) for older adults with acute or chronic illness, and up to 2.0 g/kg/day in severely ill or malnourished patients.
- Per-meal protein of 25–30 g, containing approximately 2.5–3.0 g of leucine, to reliably exceed the elderly anabolic threshold.
- Even protein distribution across meals rather than skewed distribution with most protein at dinner.
- Resistance exercise where possible, alone or in combination with protein supplementation, to sensitize muscle to leucine and amplify the response.
- Caution with renal disease — the protein recommendations apply to older adults with normal renal function or mild CKD; advanced CKD requires individualized intake based on renal function trajectory.
The shift from the legacy RDA of 0.8 g/kg/day to the PROT-AGE 1.0–1.2 g/kg/day is one of the most consequential evidence-based revisions in geriatric nutrition of the past two decades. The RDA was derived from nitrogen-balance studies in young, healthy subjects and substantially underestimates the protein needed for muscle maintenance in older adults with anabolic resistance. A 70 kg older adult on the legacy RDA would consume 56 g of protein per day; on the PROT-AGE recommendation, 70–84 g per day — the difference between sarcopenia progression and sarcopenia stability for many patients.
Practical translation: three meals of 25–30 g protein each, with a fourth small meal or snack of 15–20 g protein, reaches the PROT-AGE targets for most older adults. Sources include cottage cheese (28 g protein per cup), Greek yogurt (17 g protein per 6 oz container, often boosted with a scoop of whey for 27–32 g), 3–4 eggs at breakfast, 4 oz of chicken or fish, or a whey-protein smoothie. For older adults with reduced appetite, liquid supplements (Ensure, Boost, or specifically leucine-enriched products like Fortimel Compact Protein, Resource HiProtein, or HMB-enriched products) provide a practical workaround.
Leucine-Enriched Whey for the Elderly
Whey protein has become the dominant protein supplement form for elderly muscle preservation for several reasons. First, whey has the highest leucine percentage of any common food protein (approximately 10–11% of total amino acid mass), making it the most efficient route to reach the 2.5–3 g leucine threshold per gram of total protein. Second, whey is rapidly digested (peak plasma amino acids within 60–90 minutes), producing a sharp leucine peak that maximally engages the Sestrin2/mTORC1 cascade. Third, whey is liquid, easy to consume, and well-tolerated by older adults with reduced appetite or impaired chewing.
Commercial "leucine-enriched" products add free-form leucine (typically 1.5–3 g per serving) to the whey base, bringing total leucine per serving to 4–5 g and providing margin above the elderly threshold even if a portion of the bolus is diverted to splanchnic uptake or oxidation rather than reaching muscle. Common formulations include the Fresenius Kabi Fortimel/Fortifit product line, the Abbott Ensure Enlive product, and various clinical-nutrition formulations used in hospital settings.
Dosing considerations: most trials use twice-daily supplementation (typically morning and afternoon, or with the two lowest-protein meals of the day) to reliably hit the threshold three or four times daily. Single-daily-dose supplementation is less effective because it leaves two or three meals below the threshold. Timing relative to exercise is secondary in older adults — while young athletes obsess over the post-workout anabolic window, in elderly subjects the threshold issue dominates and timing has shown smaller effects in trials.
Cost and access: whey protein isolate retails at approximately $0.50–1.50 per 25 g serving in bulk form. Branded leucine-enriched clinical-nutrition products retail at $3–6 per serving. For older adults with adequate appetite, plain whey isolate from a reputable manufacturer (NSF Certified for Sport, USP Verified, or Informed Choice are quality marks) is typically the most cost-effective option. For older adults with reduced appetite who need calorie-and-protein-dense liquid nutrition, the branded clinical-nutrition products are worth the price differential.
HMB — Leucine's Anti-Catabolic Metabolite
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite produced from leucine in skeletal muscle and liver. Approximately 5% of dietary leucine is converted to HMB via the intermediate alpha-ketoisocaproate (KIC). Endogenous HMB production from a typical protein-rich diet is approximately 0.2–0.4 g per day. Trial doses of supplemental HMB are typically 3 g per day — an order of magnitude higher than endogenous production, requiring direct supplementation rather than dietary loading.
HMB's mechanism of action is distinct from leucine's. Where leucine acts primarily through mTORC1 to drive protein synthesis, HMB acts primarily on the catabolic side — it inhibits the ubiquitin-proteasome system that degrades muscle proteins and reduces autophagic flux of muscle proteins. The net result is reduced muscle protein breakdown rather than increased synthesis. The two effects (synthesis-driving leucine, breakdown-inhibiting HMB) are complementary, and in clinical trials the combination of leucine plus HMB produces larger effects on muscle balance than either alone.
HMB is available as two salt forms: calcium HMB (Ca-HMB), the original and most-studied form, and HMB free acid (HMB-FA), a newer form that produces faster and higher peak plasma levels. Both forms have been used in trials. The Wilson 2008 ISSN position statement on HMB supports 3 g/day dosing for muscle preservation in deconditioned populations, with stronger evidence for sustained-use protocols (8–12 weeks) than for acute single-dose effects.
The clinical populations with the strongest HMB evidence are critically ill ICU patients (where HMB reduces ICU-acquired muscle wasting), bed-rest models (where HMB attenuates disuse atrophy), and elderly subjects on hospital discharge regimens (where HMB accelerates functional recovery). For healthy young athletes, the HMB evidence is more mixed — HMB shows modest effects on strength and lean mass in untrained subjects but smaller and less consistent effects in trained athletes.
The Wilson HMB Trial Series
Jeff Wilson and the HMB research group at the University of Tampa have published one of the most influential trial series on HMB in resistance-trained populations. Their 2014 European Journal of Applied Physiology paper randomized 20 resistance-trained men to 12 weeks of HMB-FA (3 g/day) or placebo, all completing an identical periodized resistance training program. HMB-FA produced greater increases in lean mass (7.4 kg vs 2.1 kg), strength (1RM squat +77 kg vs +25 kg), and power output compared to placebo — large effects that surprised the field given the modest effects seen in untrained subjects.
The Wilson HMB-FA findings have been controversial because the effect sizes are larger than the broader HMB literature, and questions have been raised about subject selection, training program intensity, and replication. Subsequent independent trials by other groups have generally found smaller HMB effects in trained athletes. The contemporary consensus position is that HMB produces meaningful benefit in untrained, deconditioned, or elderly subjects but smaller and less reliable effects in already-trained athletes — consistent with HMB's mechanism of attenuating muscle breakdown, which has more room to improve in deconditioned states.
For elderly sarcopenia, the HMB evidence is more consistent. Multiple trials have shown that HMB supplementation (3 g/day) in older adults with mobility limitations or recent hospitalization improves muscle mass, gait speed, and functional outcomes compared to placebo. The Deutz 2013 trial in critically ill ICU patients showed that HMB attenuated ICU-acquired muscle loss measured by quadriceps cross-sectional area on ultrasound. The Berton 2015 trial in older adults during bed rest showed that HMB+vitamin D+arginine combination attenuated bed-rest-induced muscle atrophy.
Practical recommendation: for elderly sarcopenia, 3 g/day of HMB (typically as 1 g three times daily with meals) is supported by evidence and reasonably well-tolerated. The combination of leucine-enriched whey plus HMB is theoretically synergistic (synthesis-driving plus breakdown-inhibiting) and is used in some clinical protocols; head-to-head evidence for the combination over either alone is limited but biologically plausible.
Resistance Exercise as the Required Co-Intervention
Every credible sarcopenia treatment protocol includes resistance exercise. Nutritional intervention alone (the PROVIDE trial design without exercise) produces measurable but modest effects on muscle mass. The combination of leucine-enriched protein supplementation plus structured resistance training produces approximately 2–3 times the muscle and strength gains of either intervention alone — one of the largest interaction effects in geriatric medicine.
The mechanism of the exercise-nutrition synergy is multifactorial. Resistance exercise acutely sensitizes muscle to leucine for 24–48 hours, lowering the per-meal threshold and amplifying the MPS response. Chronic resistance training increases satellite cell number, ribosomal capacity, and capillary density — all of which raise the ceiling on the anabolic response. Resistance training also drives type II fiber hypertrophy, the fiber type most lost in sarcopenia and most relevant to functional recovery from falls.
Practical exercise prescription for elderly sarcopenia: progressive resistance training 2–3 times per week, targeting major muscle groups (legs, back, chest, shoulders, core), with 8–12 repetitions per set at 70–80% of one-repetition maximum, 2–3 sets per exercise. Machines are preferred over free weights for the deconditioned elderly because they reduce balance and skill demands and allow safer progressive overload. Pneumatic resistance machines (Keiser, HUR) are particularly well-suited to older populations because resistance can be adjusted in 0.5–1 lb increments.
The Fiatarone 1990 NEJM paper remains the landmark demonstration that even nonagenarian nursing home residents can build muscle and strength through resistance training. Subjects in their 80s and 90s nearly tripled their leg strength and doubled their gait speed over 8 weeks of high-intensity resistance training. The clinical implication is that "too old to train" is essentially never true — some training is always better than none, even in the oldest old.
Programs that combine structured resistance training with leucine-enriched protein supplementation have demonstrated reductions in fall risk, fracture risk, and progression to dependency over 1–2 year follow-up. The combination should be considered the standard of care for any older adult diagnosed with sarcopenia or at risk for it.
Practical Clinical Protocols
Translating the evidence into operational protocols:
- Asymptomatic older adult, age 60+, no diagnosed sarcopenia — baseline screening (grip strength, gait speed, chair-stand time). If borderline or low, implement PROT-AGE protein targets (1.0–1.2 g/kg/day, 25–30 g per meal), begin or continue resistance training 2–3 times per week. Re-screen annually.
- Diagnosed sarcopenia by EWGSOP2 criteria — full intervention: PROT-AGE protein targets, twice-daily leucine-enriched whey supplementation (20 g whey + 3 g free leucine per dose), structured resistance training 2–3 times per week supervised by a physical therapist or trainer, vitamin D repletion to serum 25(OH)D 30–50 ng/mL, optimization of any reversible contributors (hypothyroidism, hypogonadism in men, chronic infection, depression).
- Acute hospitalization or surgical recovery in older adult — high-protein enteral or oral nutrition (1.5–2.0 g/kg/day if renal function permits), HMB 3 g/day during the catabolic period, early mobilization, transition to resistance training as soon as medically appropriate.
- Frailty syndrome (low gait speed, exhaustion, weakness, low activity, weight loss) — high-leucine whey supplementation, vitamin D repletion, supervised resistance training, geriatric assessment for reversible contributors, advance care planning.
- Pre-surgical optimization (prehabilitation) in elderly patient — 4–6 weeks of high-protein nutrition (leucine-enriched whey) plus resistance training before elective surgery to enter the catabolic post-operative state from a position of strength. This is the most reliably effective intervention to reduce post-operative loss of function in elderly surgical patients.
The cost-effectiveness analyses of sarcopenia prevention protocols are highly favorable. The Bauer/PROVIDE supplement intervention alone costs approximately $3–5 per day; structured resistance training costs vary from free (home-based with bodyweight or resistance bands) to $30–50 per supervised session. Compared to the cost of a single hip fracture surgery and subsequent rehabilitation ($30,000–100,000+ including loss of independent living), the prevention math is overwhelming.
Contraindications and Special Populations
- Advanced chronic kidney disease — protein restriction may be prescribed to slow progression in pre-dialysis CKD stages 4–5. The trade-off against accelerated sarcopenia is real and should be discussed with the nephrologist. Ketoacid analogs of leucine that bypass the nitrogen burden have been tested in this setting and may provide a compromise for some patients.
- Maple syrup urine disease (MSUD) — rare inborn error of branched-chain alpha-keto acid dehydrogenase. Leucine and HMB are contraindicated; dietary leucine must be tightly restricted.
- Hepatic encephalopathy — aromatic amino acids and ammonia are the principal drivers, not leucine. BCAA supplementation (including leucine) is actually beneficial in this setting and has been used clinically.
- Active cancer — complex. mTORC1 signaling supports tumor growth in many cancers, and some oncologists prefer lower-protein diets during active treatment. Cachexia of advanced cancer simultaneously demands muscle preservation. Patient-specific input from the oncology team is required.
- Cognitive impairment that affects feeding — the practical problem is often getting any food eaten, not optimizing leucine. Liquid leucine-enriched supplements, finger foods rich in protein, and family-supported feeding are higher priorities than dose optimization.
- Severe dysphagia — thickened liquid leucine-enriched supplements, pureed high-protein foods, and speech-pathology evaluation for safe swallowing. Enteral nutrition (tube feeding) is appropriate for severe cases where oral intake is unsafe.
- End-stage frailty or terminal illness — the goal of nutrition shifts from sarcopenia prevention to comfort. Aggressive protein supplementation may be inappropriate when the natural trajectory is decline; palliative-care principles should guide intensity of nutritional intervention.
Key Research Papers
- Bauer JM et al. (2015). Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study. JAMDA. — PubMed
- Bauer J et al. (2013). Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. JAMDA. — PubMed
- Volpi E et al. (2000). Exogenous amino acids stimulate net muscle protein synthesis in the elderly. Journal of Clinical Endocrinology and Metabolism. — PubMed
- Cuthbertson D et al. (2005). Anabolic signaling deficits underlie amino acid resistance of wasting, aging muscle. FASEB Journal. — PubMed
- Cruz-Jentoft AJ et al. (2019). Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing. — PubMed
- Wilson JM et al. (2014). The effects of 12 weeks of beta-hydroxy-beta-methylbutyrate free acid supplementation on muscle mass, strength, and power in resistance-trained individuals. European Journal of Applied Physiology. — PubMed
- Wilson JM et al. (2013). International Society of Sports Nutrition Position Stand: beta-hydroxy-beta-methylbutyrate (HMB). Journal of the International Society of Sports Nutrition. — PubMed
- Nissen S et al. (1996). Effect of leucine metabolite beta-hydroxy-beta-methylbutyrate on muscle metabolism during resistance-exercise training. Journal of Applied Physiology. — PubMed
- Fiatarone MA et al. (1990). High-intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA. — PubMed
- Deutz NEP et al. (2013). Effect of beta-hydroxy-beta-methylbutyrate (HMB) on lean body mass during 10 days of bed rest in older adults. Clinical Nutrition. — PubMed
- Paddon-Jones D, Rasmussen BB (2009). Dietary protein recommendations and the prevention of sarcopenia. Current Opinion in Clinical Nutrition and Metabolic Care. — PubMed
- Rondanelli M et al. (2016). Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life in elderly with sarcopenia. American Journal of Clinical Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Sarcopenia leucine whey
- PubMed: Anabolic resistance in elderly
- PubMed: HMB and sarcopenia
- PubMed: PROT-AGE recommendations
- PubMed: Resistance training in elderly
Connections
- Leucine Benefits Hub
- Leucine Overview
- Muscle Protein Synthesis
- mTOR Activation
- Recovery and Exercise
- Vitamin D3 (Co-Intervention)
- Isoleucine
- Valine
- Creatine
- Collagen
- Geriatrics
- Osteoporosis
- Eggs
- Beef
- All Amino Acids