Isoleucine for Endurance Performance
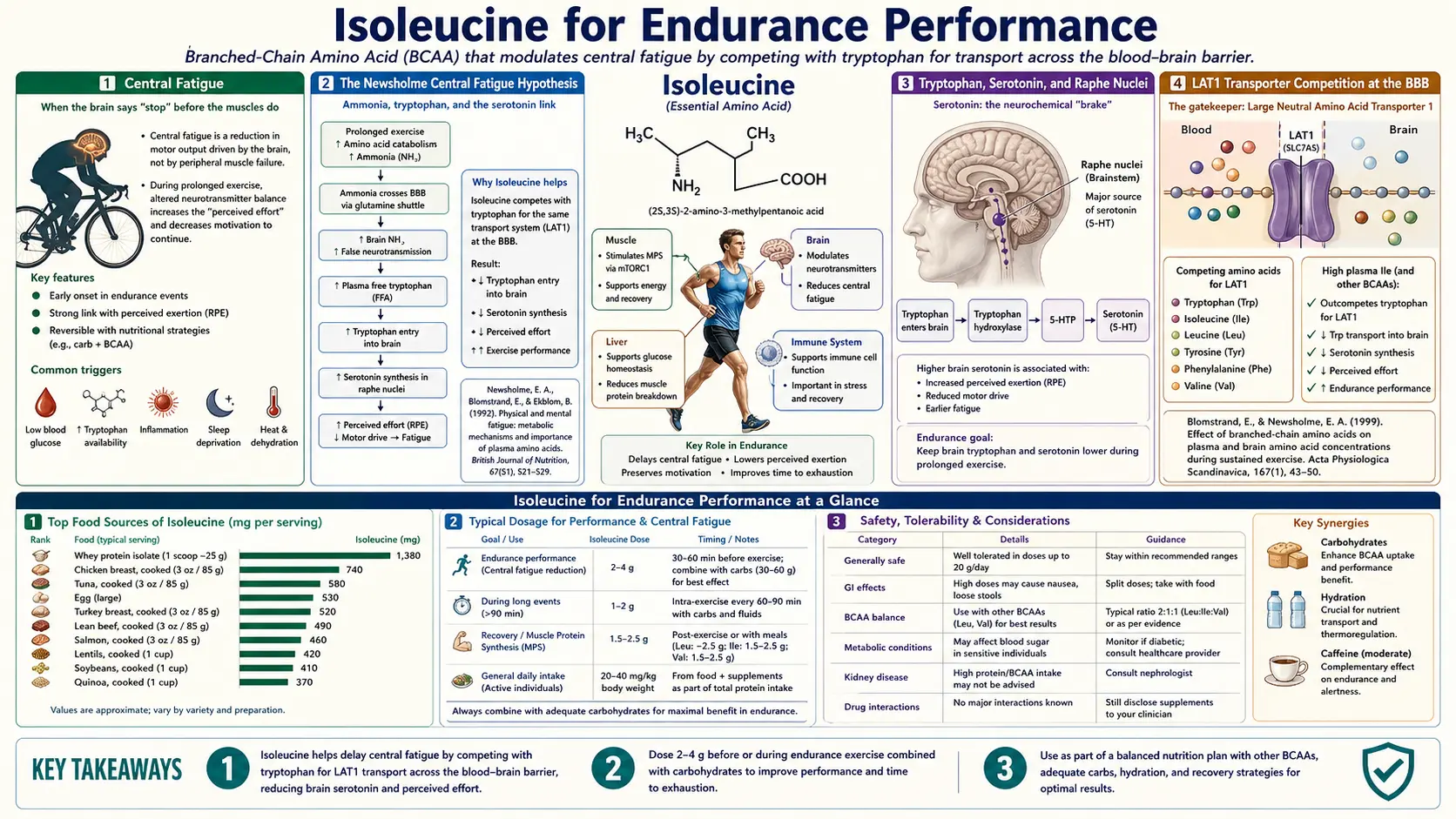
The case for BCAA supplementation in endurance athletes rests on a single elegant hypothesis: branched-chain amino acids and the aromatic amino acid tryptophan compete for the same transporter (LAT1) at the blood-brain barrier, so loading BCAAs in plasma can block tryptophan uptake into the brain, suppress serotonin synthesis in the raphe nuclei, and delay the onset of central fatigue during prolonged exercise. This is the Newsholme central fatigue hypothesis, first proposed in 1987 and tested in dozens of controlled trials over the following decades. The animal evidence is consistent; the human evidence is mixed. Where the BCAA-and-endurance story is most defensible is in long-duration events (marathon, ultra, multi-hour cycling) where glycogen depletion combines with rising plasma tryptophan to produce the "central" component of fatigue that performance-trained athletes recognize as distinct from peripheral muscle exhaustion. Isoleucine's specific contribution within the BCAA trio comes through its glucose-uptake effect (which sustains substrate delivery to working muscle as glycogen depletes) and its participation in the LAT1 competition that underlies the central fatigue mechanism.
Table of Contents
- Central Fatigue — What It Is and What It Is Not
- The Newsholme Central Fatigue Hypothesis
- Tryptophan, Serotonin, and the Raphe Nuclei
- The LAT1 Transporter Competition at the BBB
- Isoleucine's Specific Role — Glucose Plus Competition
- Timing and Dose for Endurance Events
- The Meta-Analysis Evidence Base
- Which Events Benefit Most
- Real-World Practice and Tradeoffs
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Central Fatigue — What It Is and What It Is Not
Fatigue during endurance exercise has two components. Peripheral fatigue is what most people think of: the muscles themselves cannot sustain the required power output. The substrate (glycogen) is depleted, the metabolic waste (lactate, hydrogen ions) has accumulated, the contractile apparatus is exhausted. Peripheral fatigue is what stops a sprinter at 100 meters or a power lifter on the eighth rep.
Central fatigue is different. It is the perception of effort and the willingness to continue, both generated by the central nervous system, that limits performance long before the muscles themselves are mechanically exhausted. The classic demonstration: at the point of perceived exhaustion in a 90-minute endurance bout, electrical stimulation of the working muscle still produces near-maximal contractions. The muscle is not yet exhausted; the brain has decided the cost is too high to continue. Central fatigue is a protective mechanism — it stops the organism before complete muscle failure, hyperthermia, or cardiovascular collapse occurs — but in the context of competitive sport, it is a limiter of performance that athletes legitimately try to push back against.
The central fatigue construct emerged from work in the 1980s and 1990s showing that the perception of effort, the rate of perceived exertion (RPE), and the "decision" to stop exercising do not track tightly with peripheral muscle metabolic state in prolonged endurance exercise. Instead, central neurochemistry — particularly the balance of serotonin and dopamine in the brain — appears to be the dominant determinant.
The clinical relevance: any intervention that delays or attenuates central fatigue can extend endurance performance even when peripheral substrate availability remains the rate-limiting concern. Caffeine works partly through this mechanism (adenosine receptor antagonism in the brain affects perceived effort). The BCAA central fatigue hypothesis posits a parallel intervention point through serotonin synthesis.
The Newsholme Central Fatigue Hypothesis
Eric Newsholme, an Oxford biochemist, first articulated the central fatigue hypothesis in 1987 and developed it over the following decade. The hypothesis has four steps:
- During prolonged endurance exercise, plasma free fatty acid (FFA) concentration rises as adipose tissue lipolysis is activated to provide energy substrate.
- Plasma FFAs and tryptophan both bind albumin. As FFAs rise, they displace tryptophan from albumin, increasing the concentration of free (unbound) tryptophan in plasma.
- At the same time, plasma BCAA concentration declines because muscle oxidation of BCAAs accelerates during prolonged exercise. The plasma ratio of free tryptophan to BCAAs (the fTrp:BCAA ratio) therefore rises.
- Free tryptophan competes with BCAAs for uptake across the blood-brain barrier via the LAT1 transporter. The rising fTrp:BCAA ratio drives increased tryptophan uptake into the brain, increasing serotonin synthesis in serotonergic neurons (particularly in the raphe nuclei), which then contributes to the central perception of fatigue.
The proposed therapeutic intervention is to maintain or increase plasma BCAA concentration during exercise — either through BCAA supplementation or through dietary protein intake before and during the event — to keep the fTrp:BCAA ratio low and limit tryptophan's access to the brain. The prediction is that BCAA supplementation should delay the onset of central fatigue and extend time to exhaustion in endurance trials.
Newsholme's hypothesis was the first physiologically coherent mechanism connecting amino acid metabolism to athletic endurance performance. It generated a large body of testing research, with mixed results in human trials. The animal data — particularly studies measuring direct brain serotonin levels in exercising rats — consistently supports the hypothesis. The human data is more variable, partly because measuring brain serotonin in exercising humans is difficult (it requires invasive techniques or pharmacologic surrogates), partly because the effect size of any single intervention is small relative to the natural variation in endurance performance, and partly because well-trained endurance athletes already eat protein-rich meals before competition and thus enter exercise with elevated baseline plasma BCAA.
Tryptophan, Serotonin, and the Raphe Nuclei
Tryptophan is the precursor for serotonin synthesis. The pathway: tryptophan → 5-hydroxytryptophan (by tryptophan hydroxylase, the rate-limiting enzyme, which is unsaturated under normal conditions and thus responsive to substrate concentration) → serotonin (by aromatic L-amino acid decarboxylase).
The dorsal and median raphe nuclei in the brainstem contain the majority of the brain's serotonergic cell bodies. Their axons project broadly to cortex, hippocampus, hypothalamus, and limbic structures, modulating mood, sleep, appetite, and — relevant here — the perception of effort and fatigue. Serotonin release in the cortex is associated with reduced motor drive and increased subjective fatigue; serotonin antagonists (used clinically for migraine and nausea) have been shown to enhance endurance performance in some trials, supporting the directionality of the central fatigue hypothesis.
Tryptophan availability is the most readily manipulable input to serotonin synthesis because tryptophan hydroxylase operates well below saturation under most physiological conditions. Increasing brain tryptophan concentration linearly increases serotonin synthesis over the relevant range. This is why plasma tryptophan dynamics matter for brain serotonergic activity, and why blocking tryptophan uptake at the blood-brain barrier through BCAA competition is a plausible intervention.
The clinical pharmacology around tryptophan and central fatigue includes mexazolam and other serotonin-modulating drugs, paroxetine and other SSRIs (which counterintuitively can be associated with reduced exercise capacity in some patients, consistent with the central serotonin model), and tryptophan-depletion paradigms used in psychiatric research (which can transiently improve fatigue tolerance in some experimental settings). The BCAA approach is the nutritional equivalent of these pharmacologic interventions: manipulate the tryptophan-to-BCAA balance to reduce brain tryptophan delivery during exercise.
The LAT1 Transporter Competition at the BBB
The L-type amino acid transporter 1 (LAT1, gene symbol SLC7A5) is the obligate sodium-independent antiporter that carries large neutral amino acids across the blood-brain barrier. Its substrates include leucine, isoleucine, valine, phenylalanine, tryptophan, tyrosine, methionine, and histidine — all the large neutral amino acids that need to enter the brain for protein synthesis and neurotransmitter precursor delivery.
Critically, LAT1 is competitive: when plasma concentration of one substrate is high, it occupies more of the transporter and reduces the uptake of the others. The competitive interaction is well-characterized kinetically. The BCAAs (leucine, isoleucine, valine combined) and the aromatic amino acids (tryptophan, tyrosine, phenylalanine) are the two main substrate groups that compete with one another for LAT1 capacity at the BBB.
This is the molecular substrate of the Newsholme hypothesis. By supplementing BCAAs (or maintaining high plasma BCAA through dietary protein), athletes elevate the BCAA share of LAT1 occupancy and reduce tryptophan's share, blunting tryptophan delivery into the brain even when plasma tryptophan itself is elevated. The effect is competitive, not absolute — tryptophan is not completely blocked — but the kinetics shift in a direction that should reduce brain serotonin synthesis.
The LAT1 competition also has implications outside endurance sport. Patients on levodopa for Parkinson's disease must time protein-rich meals carefully because LAT1-mediated uptake of large neutral amino acids competes with levodopa transport into the brain. The same competitive transport biology that BCAAs use to limit tryptophan delivery can also limit therapeutic drug delivery, depending on the timing and balance.
Isoleucine's Specific Role — Glucose Plus Competition
Within the BCAA trio, isoleucine contributes to the endurance picture through two parallel mechanisms.
Direct LAT1 competition. Isoleucine, like its two BCAA partners, competes with tryptophan for LAT1-mediated uptake at the BBB. A BCAA supplement containing isoleucine in the 2:1:1 ratio (along with leucine and valine) contributes proportionally to the competition. In studies that have compared 2:1:1 BCAAs to leucine-only formulations for endurance outcomes, the 2:1:1 formulation has tended to produce slightly stronger effects, partly because the additional isoleucine and valine each contribute to LAT1 occupancy.
Substrate delivery via GLUT4. As discussed in the Glucose Uptake deep-dive, isoleucine acutely promotes GLUT4 translocation in skeletal muscle through an insulin-independent PI3K pathway. During prolonged endurance exercise, when muscle glycogen is progressively depleted and the muscle becomes increasingly dependent on circulating glucose for sustained ATP production, isoleucine's GLUT4 effect can help maintain glucose delivery into the working muscle. This complements the central fatigue mechanism: the central pathway delays the brain's decision to stop, while the peripheral pathway helps maintain the actual energy substrate the muscle needs to continue.
The two mechanisms operating together — central fatigue delay plus peripheral substrate maintenance — are the strongest physiological argument for including isoleucine specifically (rather than just leucine) in endurance-targeted BCAA supplementation. Whether the combined effect translates to meaningful time-to-exhaustion improvements in well-trained athletes is the question that the human trial evidence has tried to answer with mixed results.
Timing and Dose for Endurance Events
If BCAA supplementation is going to support endurance performance, the timing and dose need to align with the physiological windows where the effect can plausibly operate:
Pre-event (60-90 minutes before). Loading 5-10 grams of 2:1:1 BCAAs in water 60-90 minutes before a long event raises plasma BCAA concentration during the early portion of the exercise, when free fatty acids are still relatively low and the competitive balance with tryptophan can be most effectively shifted. This is the timing that has been used in most positive trials.
During the event (intra-exercise). For events exceeding 90-120 minutes, ongoing BCAA intake during the exercise itself helps maintain plasma BCAA levels as muscle oxidation consumes them. Typical dose: 5-7 grams of 2:1:1 BCAAs every 60-90 minutes, often combined in a carbohydrate-electrolyte sports drink. The carbohydrate is important — the BCAAs alone do not provide significant exercise calories, and the carbohydrate addresses the peripheral substrate side of the equation.
Post-event recovery. The post-exercise window is more about muscle protein synthesis than acute performance support. A whole-protein meal (containing the full essential amino acid spectrum, not just BCAAs) is preferable to isolated BCAAs for recovery from a long endurance event. The recovery picture is discussed more fully in the Muscle Protein Synthesis deep-dive.
The dose ranges above are calibrated for adult endurance athletes (60-80 kg body weight) doing competitive-intensity exercise lasting 90+ minutes. Recreational endurance exercisers doing 30-60 minute sessions are unlikely to benefit meaningfully from BCAA supplementation because the central fatigue mechanism is not the rate-limiting factor at that duration. Trained elite athletes may benefit more than recreational athletes because they reach the central-fatigue-limited regime during their high-volume training sessions.
The Meta-Analysis Evidence Base
Several systematic reviews and meta-analyses have attempted to synthesize the trial evidence on BCAAs and endurance performance. The conclusions vary depending on which outcome measures are pooled and which trial populations are included:
Time to exhaustion outcomes. Meta-analyses pooling time-to-exhaustion trials (athletes exercise at a fixed sub-maximal intensity until volitional failure) have generally found a small positive effect of BCAA supplementation, on the order of 2-5% improvement in time to exhaustion. The effect is statistically detectable but small relative to the natural variation in test-retest reliability of endurance time-to-exhaustion tests.
Time-trial outcomes. Trials using time-trial designs (athletes complete a fixed distance as fast as possible) have shown more variable results. Some studies have found significant improvements in finishing time; others have found no effect. The variability likely reflects differences in athlete training status, dietary status, supplementation timing, and the specific cognitive demands of self-paced versus externally-paced exercise.
Subjective fatigue and rating of perceived exertion (RPE). The most consistent finding across BCAA endurance trials is a reduction in subjective fatigue and RPE at a given exercise workload. Athletes feel less tired at the same physiological intensity. This is consistent with a central fatigue mechanism: the supplementation is not making the muscle work better, it is changing the brain's perception of effort. Whether this translates to faster finishing times depends on the athlete's willingness to push harder when they feel they can.
Recovery markers. Most meta-analyses find that BCAA supplementation modestly reduces post-exercise muscle damage markers (creatine kinase, lactate dehydrogenase) and exercise-induced muscle soreness (DOMS). This is consistent with the muscle-protein-synthesis and anti-catabolic effects discussed in the partner deep-dive, rather than the central fatigue mechanism per se.
The honest summary: BCAA supplementation produces a small but real benefit in endurance performance contexts, most reliably in long-duration events where central fatigue is a meaningful limiter, and most clearly seen in subjective fatigue and recovery markers rather than in raw performance times. The effect is not transformative and does not substitute for adequate dietary protein, carbohydrate fueling during the event, or training-driven physiological adaptation.
Which Events Benefit Most
Not all endurance events are equally likely to benefit from BCAA supplementation. The events most likely to show meaningful effects are those that meet several criteria:
- Long duration (90+ minutes). The central fatigue mechanism takes time to develop. Short events end before tryptophan and FFAs have risen enough to shift the central serotonergic balance meaningfully.
- Sub-maximal intensity. All-out short-duration exercise (sprints, weightlifting) is peripheral-substrate-limited rather than central-fatigue-limited. Sub-maximal pace sustained over long distance is where central mechanisms dominate.
- Hot environments. Heat stress amplifies central fatigue through additional serotonergic mechanisms and increased perceived effort. BCAA effects have been more reliably demonstrated in hot-environment trials.
- Self-paced format. Time-trials and self-paced events depend heavily on the athlete's willingness to maintain pace, which is precisely what central fatigue limits. Fixed-pace tests to exhaustion may show different effect profiles.
- Well-trained athletes. Trained endurance athletes reach the central-fatigue regime in training and competition more consistently than recreational athletes, who often stop for peripheral or motivational reasons before central serotonergic limits become dominant.
The classic event profile that maximizes the theoretical benefit: a trained endurance athlete completing a marathon, ultramarathon, century cycling ride, or long triathlon in warm conditions. These are also the events where most positive BCAA endurance trials have been conducted. Conversely, recreational 30-minute jogging in temperate conditions is unlikely to show meaningful benefit because the limiting factors are different.
For broader endurance training context, see our pages on Fatigue and Hydration. Endurance performance is multifactorial; BCAAs are at most a small modifier within a much larger training and nutrition program.
Real-World Practice and Tradeoffs
The cost-benefit analysis for endurance athletes considering BCAA supplementation:
Benefits: Small but real improvement in time to exhaustion in long-duration sub-maximal events. Reduced subjective fatigue at given workload. Modest reduction in post-exercise muscle damage markers and soreness. Anti-catabolic protection during very long efforts that approach negative net energy balance.
Costs: Modest financial cost ($30-60 per month for a regular user). Calories that displace other fueling options (typically negligible since BCAAs are essentially zero-calorie at typical doses). Flavor and GI tolerance issues in some users. The opportunity cost of using BCAAs instead of better-validated interventions like carbohydrate fueling, electrolyte management, caffeine, or simply more training.
What well-fueled athletes actually need first: Adequate sleep, adequate training, adequate dietary protein from food (1.2-1.6 g/kg/day for endurance training, slightly higher for high-volume training), adequate carbohydrate intake (5-7 g/kg/day for moderate-volume endurance training, 8-10+ g/kg/day for very high volume), in-event carbohydrate fueling (30-90 g/hour depending on event duration and intensity), adequate hydration and electrolyte replacement, and event-day caffeine if individually tolerated. After all of these foundations are dialed in, BCAA supplementation is a small marginal addition.
The athletes most likely to benefit are those at the elite competitive level where small improvements matter, those doing very long events where central fatigue is clearly a factor, and those whose dietary protein intake is at the lower end (vegan endurance athletes who do not consume enough plant protein to comfortably meet the 1.6 g/kg/day target). Most recreational endurance athletes will get more benefit from improving the foundations than from adding BCAAs.
Cautions
- Maple syrup urine disease (MSUD) — absolute contraindication; any BCAA supplementation is potentially lethal.
- SSRI and other serotonergic medications — the BCAA central fatigue mechanism reduces brain serotonin synthesis. Theoretically, BCAAs could partially counter the therapeutic effect of SSRIs. Clinical relevance is limited (BCAA effects on brain serotonin are modest and acute), but patients on antidepressants should be aware of the interaction in principle.
- Levodopa for Parkinson's disease — the LAT1 transporter competition reduces levodopa uptake into the brain. Patients on levodopa should not take BCAA supplements within 60-90 minutes of their levodopa doses.
- Insulin resistance and type 2 diabetes — see the BCAA paradox discussion in the Glucose Uptake deep-dive. Chronic high-dose BCAA supplementation may worsen insulin resistance over time. Pre-event acute use is unlikely to be problematic, but chronic daily supplementation in diabetic athletes should be approached cautiously.
- Endurance training adaptation — one underappreciated concern: some endurance training adaptations (notably mitochondrial biogenesis driven by PGC-1alpha activation in response to glycogen depletion) depend on the metabolic stress of incomplete fueling. Supplementing aggressively during every training session may blunt these adaptations. A common practice is "train low, race high" — minimal supplementation in most training sessions to preserve the adaptive stress, with full BCAA and carbohydrate support reserved for race day.
- GI tolerance — high-dose BCAAs in concentrated form (powder mixed in a small volume of water) can cause GI upset, particularly during exercise when blood is diverted away from the digestive system. Diluting in a larger volume of fluid and consuming gradually reduces GI issues.
- Quality control — the supplement industry is poorly regulated. BCAA products have occasionally been found to contain different ratios than labeled, contaminants, or banned substances. Third-party tested products (NSF Certified for Sport, Informed Sport) are preferred for competitive athletes subject to anti-doping rules.
Key Research Papers
- Newsholme EA, Acworth IN, Blomstrand E (1987). Amino acids, brain neurotransmitters and a functional link between muscle and brain that is important in sustained exercise. Advances in Myochemistry, 1:127-133. — PubMed
- Blomstrand E (2001). Amino acids and central fatigue. Amino Acids, 20(1):25-34. — PubMed
- Davis JM, Bailey SP (1997). Possible mechanisms of central nervous system fatigue during exercise. Medicine and Science in Sports and Exercise, 29(1):45-57. — PubMed
- Blomstrand E, Hassmen P, Ekblom B, Newsholme EA (1991). Administration of branched-chain amino acids during sustained exercise — effects on performance and on plasma concentration of some amino acids. European Journal of Applied Physiology, 63(2):83-88. — PubMed
- Mittleman KD, Ricci MR, Bailey SP (1998). Branched-chain amino acids prolong exercise during heat stress in men and women. Medicine and Science in Sports and Exercise, 30(1):83-91. — PubMed
- Watson P, Shirreffs SM, Maughan RJ (2004). The effect of acute branched-chain amino acid supplementation on prolonged exercise capacity in a warm environment. European Journal of Applied Physiology, 93(3):306-314. — PubMed
- Fernstrom JD (2005). Branched-chain amino acids and brain function. Journal of Nutrition, 135(6 Suppl):1539S-1546S. — PubMed
- Meeusen R, Watson P (2007). Amino acids and the brain: do they play a role in "central fatigue"? International Journal of Sport Nutrition and Exercise Metabolism, 17(Suppl):S37-46. — PubMed
- Greer BK, White JP, Arguello EM, Haymes EM (2011). Branched-chain amino acid supplementation lowers perceived exertion but does not affect performance in untrained males. Journal of Strength and Conditioning Research, 25(2):539-544. — PubMed
- Gualano AB et al. (2011). Branched-chain amino acids supplementation enhances exercise capacity and lipid oxidation during endurance exercise after muscle glycogen depletion. Journal of Sports Medicine and Physical Fitness, 51(1):82-88. — PubMed
- AbuMoh'd MF, Matalqah L, Al-Abdulla Z (2020). Effects of oral branched-chain amino acids (BCAAs) intake on muscular and central fatigue during an incremental exercise. Journal of Human Kinetics, 72:69-78. — PubMed
- Rahimi MH, Shab-Bidar S, Mollahosseini M, Djafarian K (2017). Branched-chain amino acid supplementation and exercise-induced muscle damage in exercise recovery: a meta-analysis of randomized clinical trials. Nutrition, 42:30-36. — PubMed
PubMed Topic Searches
- PubMed: BCAA central fatigue tryptophan serotonin
- PubMed: Newsholme central fatigue hypothesis
- PubMed: LAT1 BBB transport competition
- PubMed: BCAA endurance time-to-exhaustion meta-analysis
- PubMed: BCAAs marathon endurance performance
Connections
- Isoleucine Overview
- Isoleucine Benefits Hub
- Isoleucine for Muscle Protein Synthesis
- Isoleucine for Glucose Uptake
- Isoleucine for Hemoglobin & Wound Healing
- Leucine
- Valine
- Tryptophan
- Tyrosine
- Phenylalanine
- Fatigue
- Hydration
- Eggs
- All Amino Acids