D-Serine: The Brain's Memory Amino Acid
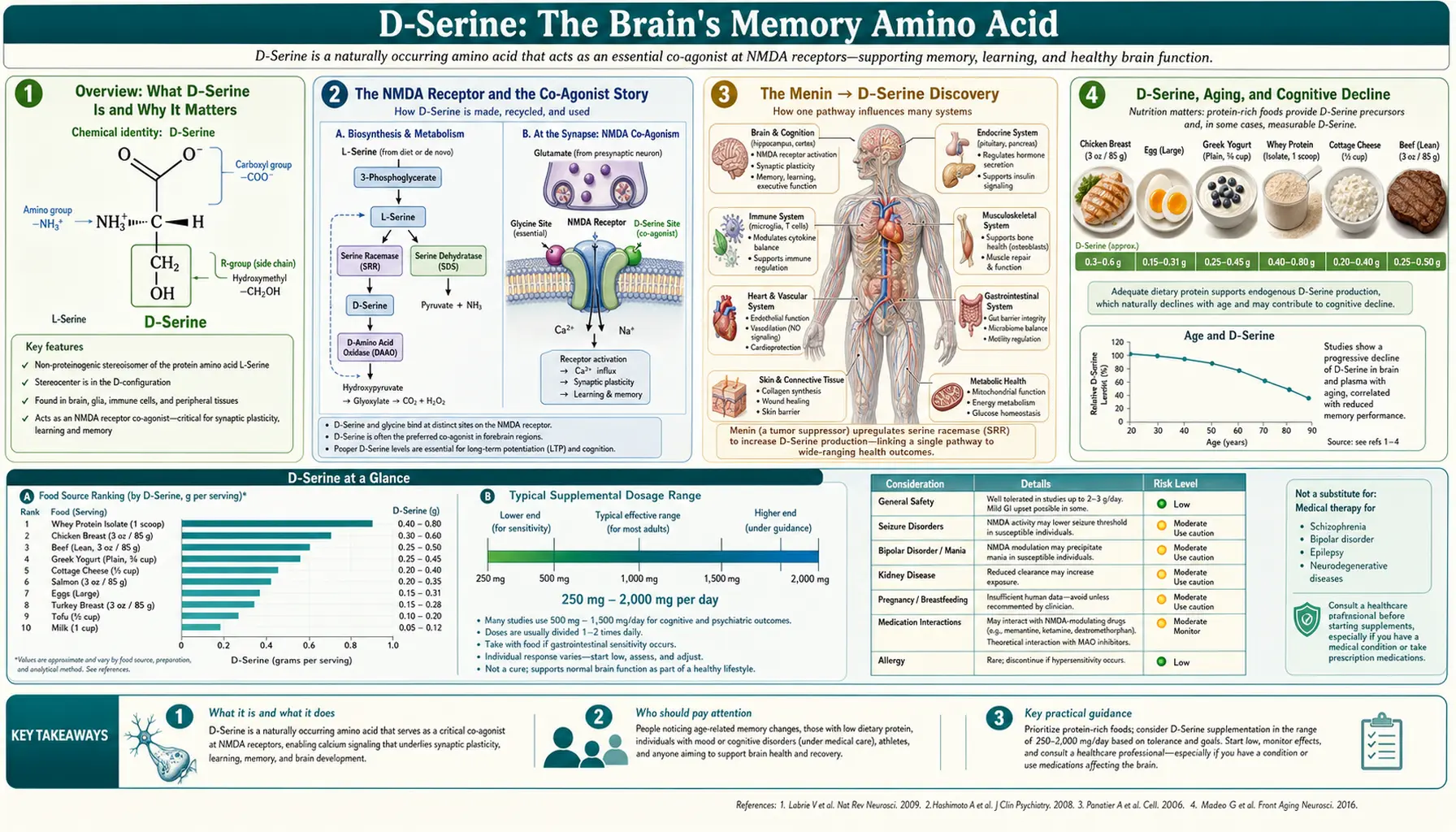
Table of Contents
- Overview: What D-Serine Is and Why It Matters
- The NMDA Receptor and the Co-Agonist Story
- The 2026 Xiamen Menin → D-Serine Discovery
- D-Serine, Aging, and Cognitive Decline
- D-Serine in Schizophrenia and Psychiatric Research
- Research Dosing and Bioavailability
- Safety and the Kidney Caution
- Dietary Sources and Body Synthesis
- Future Research Directions
- Key Research Papers
- Featured Videos
Overview: What D-Serine Is and Why It Matters
D-Serine is the mirror-image form of the common amino acid serine. In chemistry, most amino acids come in two shapes — like a left hand and a right hand — called L- and D-forms. Your body's proteins are built almost entirely from L-forms. For decades, scientists assumed D-amino acids were biological oddities or contaminants. D-Serine shattered that assumption.
In the 1990s, researchers discovered that D-Serine is produced abundantly in the human brain and acts as a master key for one of the most important memory switches in biology: the NMDA receptor. Without enough D-Serine, this receptor cannot open fully. When NMDA receptors fail to open when they should, memories don't form properly, thinking slows, and the brain's capacity for change — its plasticity — diminishes.
D-Serine is now recognized as a gliotransmitter, a signaling molecule released primarily by astrocytes (the star-shaped support cells surrounding neurons) rather than by neurons themselves. This makes it unusual: most neurotransmitters come from neurons. Astrocytes monitor neural activity and release D-Serine precisely when nearby synapses are firing hard enough to warrant memory consolidation. Think of it as the brain's approval stamp on a learning event: "Yes, this matters — save it."
What makes D-Serine clinically relevant today is a cascade of findings linking it to aging, Alzheimer's disease, schizophrenia, and — most recently — a landmark 2026 discovery connecting a longevity protein called Menin to D-Serine production in the hypothalamus. The implications reach from brain aging to cognitive restoration in elderly animal models, and early human supplementation trials are now underway.
The NMDA Receptor and the Co-Agonist Story
The NMDA (N-methyl-D-aspartate) receptor is a protein channel in the membrane of neurons. It sits at the center of long-term potentiation (LTP) — the cellular process that actually encodes a memory. When LTP fires, it physically strengthens the connection between two neurons by adding more receptor proteins to the synapse and reorganizing the molecular scaffolding on both sides.
NMDA receptors are famous for requiring two keys simultaneously to open. The first key is glutamate, the brain's main excitatory neurotransmitter — released when one neuron fires. The second key, for a long time thought to be glycine, turns out to be predominantly D-Serine at most brain synapses involved in learning and memory.
Here is the mechanism in plain terms. The NMDA receptor has a special site called the glycine-B co-agonist site. Despite its name, D-Serine — not glycine — occupies this site at the synapses in the hippocampus and prefrontal cortex that handle memory formation. When D-Serine is present at adequate concentrations and glutamate is also released, the receptor opens its ion channel, calcium floods into the neuron, and the biochemical cascade for memory storage begins. If D-Serine is absent or reduced, the receptor stays closed even when glutamate is present. No calcium entry. No LTP. No memory consolidation.
The enzyme that makes D-Serine is called serine racemase — it converts L-Serine (the ordinary dietary form) into D-Serine by flipping its molecular shape. A second enzyme, D-amino acid oxidase (DAAO), breaks D-Serine down. The balance between these two enzymes determines how much D-Serine is available at any given synapse. Genetic variants that increase DAAO activity (reducing D-Serine) are associated with higher risk of schizophrenia, underscoring how tightly this molecule is tied to brain function.
A remarkable feature of this system is its spatial precision. Astrocytes wrap around synapses like a glove, releasing D-Serine directly into the synaptic cleft only when local neural activity demands it. This means D-Serine availability is not just a brain-wide average — it is a local, real-time readout of whether a particular synapse is ready to learn.
The Menin → D-Serine Discovery
One of the most talked-about findings linking D-Serine to brain aging comes from Lige Leng's team at Xiamen University, who reported in PLOS Biology (Leng L, et al., Hypothalamic Menin regulates systemic aging and cognitive decline, 2023; widely re-covered in the press in 2026) that the protein Menin acts in the ventromedial hypothalamus to control D-Serine production. In their mouse experiments, lowering Menin accelerated cognitive aging while reducing brain D-Serine, and either restoring Menin or supplementing D-Serine directly rescued the memory deficits — positioning D-Serine as a potential bypass for an aging Menin signal (DOI: 10.1371/journal.pbio.3002033). These are animal results, not a proven human therapy — the fuller story is told in the dedicated History article.
D-Serine, Aging, and Cognitive Decline
Independent of the Menin story, multiple research groups have documented a consistent and significant age-related decline in brain D-Serine levels. In rat brain studies, D-Serine concentrations fall steadily from young adulthood onward, with the sharpest drops in the hippocampus — the brain's primary memory-formation center. By late life, hippocampal D-Serine levels in old rodents are roughly 30–50% lower than in young adults.
This matters because NMDA receptor function deteriorates in parallel. Aged neurons show reduced LTP magnitude, slower learning, and impaired memory consolidation — exactly what you would expect if the co-agonist for NMDA receptors were in short supply. Supplementing D-Serine in aged mice has been shown to restore NMDA-mediated LTP to near-young levels, and this restoration correlates with improved performance on spatial memory tasks (the rodent equivalent of remembering where you parked the car).
In humans, D-Serine levels in cerebrospinal fluid (CSF) have been measured in Alzheimer's disease patients. A 2015 study in Translational Psychiatry found that CSF D-Serine was elevated in Alzheimer's patients compared to controls — a finding that initially seems counterintuitive. The interpretation is nuanced: in early Alzheimer's, excitotoxic overactivation of NMDA receptors may actually produce a compensatory rise in D-Serine, or the blood-brain barrier leak may cause accumulation. In late-stage disease, levels fall. The relationship is not a simple linear decline, which is one reason D-Serine's therapeutic window in dementia requires careful study.
White matter is also relevant. Astrocytes are the predominant cell type in white matter, and D-Serine production is primarily astrocytic. As white matter degrades with age — a process visible on MRI as white matter hyperintensities — the astrocyte populations that produce D-Serine may be compromised, creating a localized supply shortage even if serine racemase activity appears normal in gray matter assays.
The practical implication: brain aging may be partly a story of failing D-Serine supply, and the Menin pathway identified by the Leng group in 2026 may be one of the primary upstream drivers of that supply failure.
D-Serine in Schizophrenia and Psychiatric Research
The connection between D-Serine and schizophrenia is one of the most clinically developed areas of research on this molecule. The core hypothesis, called the NMDA receptor hypofunction model of schizophrenia, holds that insufficient NMDA receptor activation — not too much dopamine, as the older model emphasized — underlies the cognitive and negative symptoms of schizophrenia (flat affect, social withdrawal, impaired working memory) that antipsychotic drugs fail to treat.
The evidence for NMDA hypofunction in schizophrenia is substantial. Phencyclidine (PCP) and ketamine, which block NMDA receptors directly, reproduce the full symptom profile of schizophrenia — including hallucinations, paranoia, and cognitive disorganization — in healthy volunteers. No other pharmacological challenge does this. Genetic studies consistently find variants in NMDA receptor subunits and in serine racemase (the enzyme that makes D-Serine) in schizophrenia patients.
If NMDA hypofunction is the problem, then supplementing D-Serine to increase co-agonist occupancy is a logical treatment strategy. Early open-label studies were promising. Phase 2 clinical trials followed, testing doses ranging from 30 mg/kg to 120 mg/kg of body weight per day — substantially higher than typical amino acid supplement doses, because crossing the blood-brain barrier efficiently requires driving high plasma concentrations. For a 70 kg person, 30 mg/kg equals 2.1 g/day; 120 mg/kg equals 8.4 g/day.
Controlled trials by Jonathan Kantrowitz and colleagues found significant improvements in negative symptoms and cognitive function in schizophrenia patients treated with high-dose D-Serine as an add-on to antipsychotic medication. Improvements in working memory, social cognition, and processing speed were observed, with effect sizes in the moderate range (Cohen's d ≈ 0.5–0.7 for cognitive outcomes in the best trials). These are not trivial numbers for conditions that have historically been treatment-resistant.
The challenge in schizophrenia trials is the same as in aging research: kidney safety at high doses (discussed in the next section) and the difficulty of standardizing brain D-Serine levels from peripheral supplementation. Sarcosine (N-methylglycine), which inhibits the transporter that clears D-Serine from synapses, is being studied as a way to amplify D-Serine effects without requiring such large doses.
Research Dosing and Bioavailability
D-Serine is an amino acid, and like most amino acids it is absorbed efficiently from the gastrointestinal tract. Oral bioavailability in humans is high — studies report plasma levels rising predictably within 30–60 minutes of ingestion, with peak plasma concentrations at roughly 1–2 hours post-dose.
The plasma half-life of D-Serine is approximately 5 hours in healthy adults, meaning a single oral dose is largely cleared within one to two days. This half-life informs dosing frequency: twice-daily dosing maintains more stable plasma levels than a single large daily dose.
In cognitive aging and schizophrenia research, the most commonly used doses fall in the range of 2 to 4 grams per day split into two doses with meals. Some schizophrenia trials have gone higher (up to 120 mg/kg), but these are under medical supervision specifically because of the kidney safety considerations described below.
Taking D-Serine with food appears to slow absorption modestly and may reduce peak plasma concentrations — which is generally favorable for kidney safety, since the kidney filters amino acids from the blood and very high acute plasma spikes create higher tubular exposure. There is no evidence that food co-ingestion meaningfully reduces the amount of D-Serine that eventually reaches the brain.
Blood-brain barrier penetration of orally ingested D-Serine is real but modest. Large neutral amino acid transporters carry D-Serine from blood into the CNS, but they are shared with many other amino acids (including L-Serine, leucine, and phenylalanine), creating competition. This is one reason therapeutic doses in brain-targeted studies tend to be higher than simple bioavailability calculations would predict — you need to drive enough plasma concentration to push meaningful amounts across the barrier despite the competition.
D-Serine is water-soluble, stable at room temperature, and available as a pure crystalline powder or in capsules. No special timing relative to exercise or sleep has been established in the literature, though theoretical arguments favor morning dosing given its role in daytime learning and memory consolidation.
Safety and the Kidney Caution
D-Serine's most significant safety concern is dose-dependent kidney toxicity. This was discovered in rodent studies where very high doses — far above what humans have been given in clinical trials — produced damage to the renal proximal tubule, the section of the kidney's filtration system responsible for reabsorbing amino acids from the filtrate before it becomes urine.
The mechanism is partly understood. The proximal tubule cells that reabsorb D-Serine contain high levels of D-amino acid oxidase (DAAO), the enzyme that breaks D-Serine down. When D-Serine concentrations in the tubular fluid are very high, DAAO activity increases dramatically, generating hydrogen peroxide as a byproduct. In high enough concentrations, this oxidative load damages or kills the tubule cells — a process called proximal tubular necrosis.
Critically, this toxicity is dose-dependent and species-dependent. Rats appear significantly more sensitive than humans to this effect, for reasons including differences in kidney DAAO activity and tubular anatomy. The doses that caused kidney injury in rats translate (per body weight) to human doses several times higher than those used in published clinical trials. In the human trials conducted to date — at doses up to 120 mg/kg/day for several weeks — kidney function markers (creatinine, BUN, urinalysis) have not shown clinically significant changes.
That said, the risk is real enough that kidney function monitoring is standard practice in clinical trials, and people with pre-existing kidney disease or reduced kidney function should treat D-Serine supplementation with particular caution. The therapeutic window — the gap between a cognitively effective dose and a nephrotoxic dose — appears to be reasonably wide in healthy humans, but it is not infinite, and dose-escalation studies are still ongoing.
Other safety signals in humans have been modest. Some individuals report mild gastrointestinal discomfort (nausea, loose stools) at higher doses, which is common with large amino acid loads and typically resolves by taking D-Serine with food or splitting doses. No serious cardiac, hepatic, or neurological adverse events have been attributed to D-Serine supplementation in published human trials.
The practical guidance from the research community: at the 2–4 g/day range studied for cognitive aging, the risk profile appears acceptable for healthy adults with normal kidney function. At the higher doses studied in schizophrenia, medical supervision and periodic kidney function monitoring are warranted.
Dietary Sources and Body Synthesis
D-Serine does not come directly from food in meaningful amounts — dietary proteins contain almost exclusively L-amino acids. The body makes its own D-Serine through a dedicated enzymatic conversion.
The key enzyme is serine racemase, which sits in astrocytes and neurons and catalyzes the interconversion of L-Serine and D-Serine. "Racemase" refers to an enzyme that converts between the two mirror-image forms (enantiomers) of a molecule. Serine racemase requires pyridoxal 5'-phosphate (the active form of vitamin B6) as a cofactor — meaning B6 deficiency could theoretically impair D-Serine synthesis, though clinical evidence for this is limited.
The substrate — L-Serine — does come from the diet. L-Serine is found in significant quantities in:
- Animal proteins: eggs, beef, pork, chicken, fish, and dairy are all excellent sources. A single egg provides roughly 400–500 mg of L-Serine.
- Soy products: soybeans and tofu are particularly high in L-Serine among plant foods.
- Legumes and nuts: lentils, peanuts, almonds, and walnuts provide moderate amounts.
- Whole grains: especially oats and wheat germ.
L-Serine itself can also be synthesized in the body from the glycolytic intermediate 3-phosphoglycerate, via a three-step pathway in the liver and brain. This means that even on a very low-protein diet, some L-Serine (and therefore some D-Serine via racemase) will be available — but dietary adequacy of L-Serine supports optimal substrate availability for D-Serine synthesis.
Glycine, the simplest amino acid and a close structural relative of serine, shares some metabolic pathways with serine and is worth noting: serine can be converted to glycine (and vice versa) by the enzyme serine hydroxymethyltransferase. Glycine also binds the NMDA receptor's co-agonist site, though with lower potency than D-Serine at hippocampal synapses. Dietary glycine (found in collagen-rich foods like bone broth, skin, and connective tissue) may provide modest support to the broader NMDA co-agonist pool.
One practical takeaway: a protein-adequate diet with sufficient vitamin B6 (found in poultry, fish, potatoes, and bananas) provides the raw materials for endogenous D-Serine synthesis. Supplemental D-Serine is not a substitute for dietary protein — it is an addition to an already-adequate nutritional base.
Future Research Directions
The Menin → D-Serine pathway identified in 2026 opens several compelling lines of inquiry. The most immediate question is whether the same hypothalamic Menin decline observed in mice occurs in aging humans, and whether blood or CSF D-Serine levels can serve as a reliable proxy biomarker for this decline. If so, D-Serine supplementation could eventually be personalized: measure D-Serine levels, supplement to restore a target range, and monitor cognitive outcomes.
Combination strategies are likely to be more powerful than D-Serine alone. The most promising pairings under investigation include:
- D-Serine + sarcosine: Sarcosine inhibits the GlyT1 transporter that clears D-Serine and glycine from synapses, potentially amplifying the effect of a given D-Serine dose while reducing the total amount needed.
- D-Serine + rapamycin or other mTOR modulators: The mTOR pathway regulates astrocyte function, including serine racemase expression. Combining D-Serine with longevity interventions that alter astrocyte biology may produce synergistic effects.
- D-Serine + L-Serine supplementation: Since L-Serine is the substrate for racemase, ensuring abundant substrate alongside the product may produce more sustained brain availability than D-Serine alone.
- D-Serine timing + sleep: Memory consolidation occurs predominantly during slow-wave sleep, which also peaks NMDA-dependent synaptic remodeling. Whether timing D-Serine doses to maximize evening plasma levels improves memory outcomes is an open question.
Human trials remain the critical gap. The schizophrenia literature provides a safety scaffold for doses up to 120 mg/kg in adults, but rigorous randomized controlled trials in cognitively aging older adults without psychiatric diagnoses are still sparse. The first such trials, targeting mild cognitive impairment (MCI), are now recruiting in several centers following the attention generated by the Menin discovery.
Long-term safety data beyond 6–12 months in humans does not yet exist. The kidney question will not be fully resolved until multi-year studies are completed. And the question of whether D-Serine supplementation can not only slow but actively reverse established cognitive decline — as the Menin mouse model suggests is possible — awaits human confirmation.
The broader significance of the Menin pathway is that it places D-Serine at the intersection of the longevity biology field (Menin, mTOR, sirtuins) and the neuroscience field (NMDA receptors, LTP, memory). That intersection had not been clearly mapped before 2026. It makes D-Serine one of the more scientifically grounded candidates in the emerging field of cognitive longevity medicine.
Key Research Papers
- Leng L, Yuan Z, Su X, et al. "Hypothalamic Menin regulates systemic aging and cognitive decline." PLOS Biology. 2023;21(3):e3002033. DOI: 10.1371/journal.pbio.3002033
- Mothet JP, et al. "D-Serine is an endogenous ligand for the glycine site of the N-methyl-D-aspartate receptor." Proc Natl Acad Sci USA. 2000;97(9):4926-4931 — Search PubMed
- Wolosker H. "D-Serine regulation of NMDA receptor activity." Science's STKE. 2006;2006(356):pe41 — Search PubMed
- Maekawa M, et al. "Contribution of D-Serine to cognitive impairment in a mouse model of schizophrenia." J Neurosci. 2005;25(7):1561-1565 — Search PubMed
- Williams SM, et al. "Sustained delivery of D-Serine to the brain and its effects on NMDA receptor-dependent cognitive function." Neurobiology of Aging. 2007;28(10):1503-1512. PMID: 16860440
- Kantrowitz JT, Javitt DC. "D-Serine for the treatment of schizophrenia: a review." Schizophrenia Research. 2010;124(1-3):1-13 — Search PubMed
- Kantrowitz JT, et al. "High dose D-Serine in the treatment of schizophrenia." Schizophrenia Research. 2010;121(1-3):125-130 — Search PubMed
- Madeira C, et al. "D-Serine levels in cerebrospinal fluid in Alzheimer's disease: the effect of comorbidities." Translational Psychiatry. 2015;5(12):e690 — Search PubMed
- Inoue R, et al. "Enhancement of cognitive function in aged mice by means of D-Serine supplementation." Molecular Brain. 2018;11(1):25 — Search PubMed
- Avellar M, et al. "Synaptic plasticity in a model of Huntington's disease: the role of D-Serine and the glutamatergic connectome." Frontiers in Cellular Neuroscience. 2018;12:442 — Search PubMed
- Basu AC, et al. "Targeted disruption of serine racemase affects glutamatergic neurotransmission and behavior." Molecular Psychiatry. 2009;14(7):719-727 — Search PubMed
- Ohnuma T, et al. "Serine racemase expression in the prefrontal cortex of patients with schizophrenia." Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(6):1392-1397 — Search PubMed
- Stevens ER, et al. "D-Serine and serine racemase are present in the vertebrate retina and contribute to the physiological activation of NMDA receptors." Proc Natl Acad Sci USA. 2003;100(11):6789-6794 — Search PubMed
Live PubMed Searches
- D-Serine NMDA receptor memory
- D-Serine aging cognitive decline
- Serine racemase brain astrocyte
- D-Serine schizophrenia clinical trial
- D-Serine Alzheimer cerebrospinal fluid
- Menin hypothalamus brain aging
Connections
- Serine (L-Serine) — the dietary precursor to D-Serine
- Glycine — NMDA co-agonist and metabolic relative
- All Amino Acids
- Neurology Disease Index
- Alzheimer's Disease
- Parkinson's Disease
- Psychiatry Disease Index
- Schizophrenia
- Longevity Protocols
- Menin Protein — upstream regulator of D-Serine
- Active B12 Test — B12 and neurological function
- Lab Tests Index
- Vitamin B6 — cofactor for serine racemase
- Magnesium — NMDA receptor modulator
- MCAS and neurological overlap
- May 28, 2026 News — Menin and D-Serine discovery