PABA (Para-Aminobenzoic Acid): The Former Vitamin B10
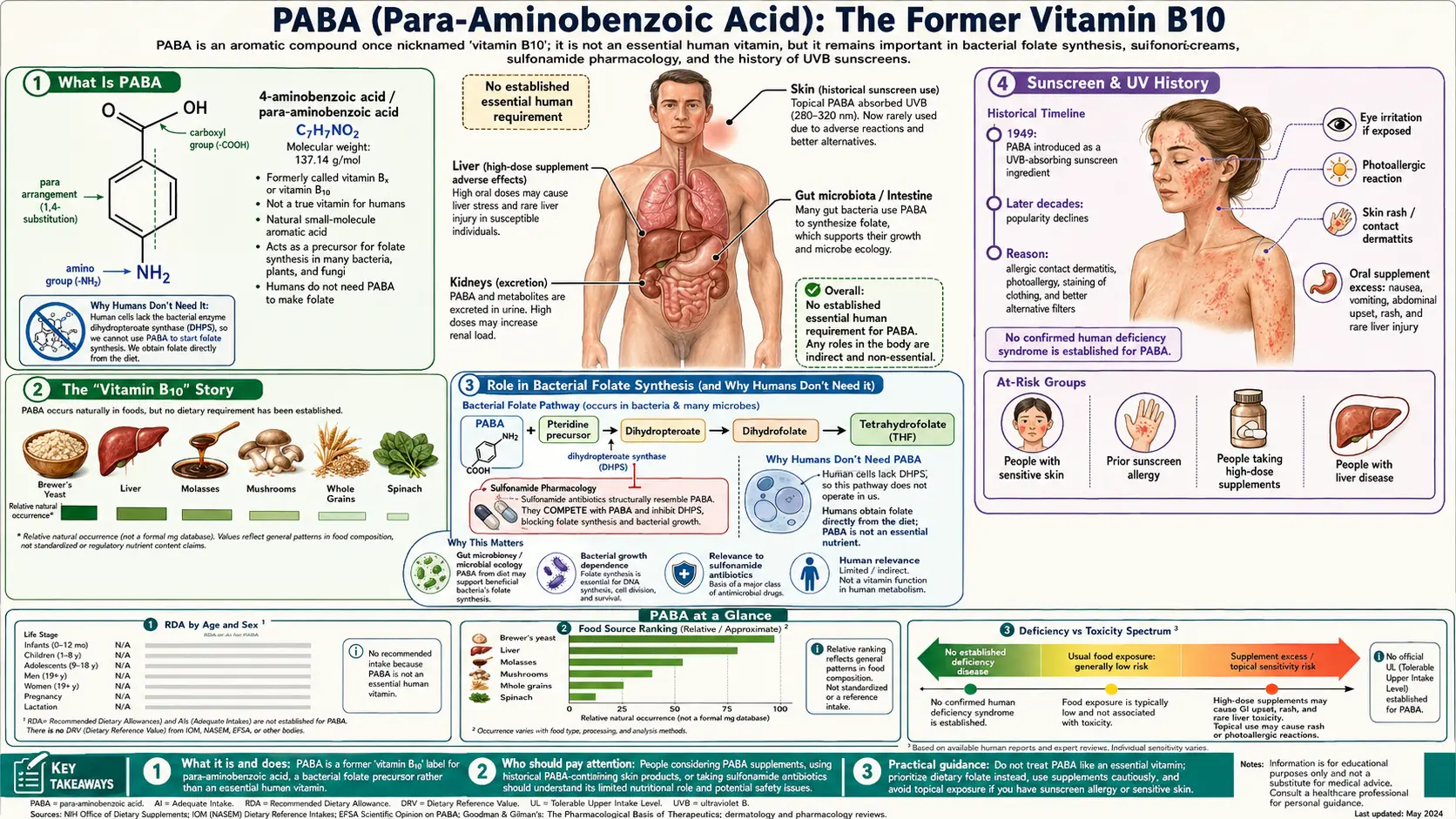
Para-aminobenzoic acid (PABA) is a real organic compound that was once marketed as "vitamin B10" — and also as "vitamin Bx" and "vitamin H1" — but it is not a vitamin for human beings. There is no PABA deficiency disease, no recommended intake, and no Daily Value, because the human body has no requirement for it. PABA earns its place in nutrition history honestly: it is an essential building block that many bacteria use to manufacture their own folate, which is exactly why the sulfa antibiotics — drugs that block that bacterial step — work at all. This page separates the genuine, citable science of PABA (its role in microbial folate synthesis, its history as a UVB sunscreen ingredient, and the prescription drug potassium para-aminobenzoate studied for Peyronie's disease and scleroderma) from the folk claims, such as the idea that it restores gray hair, where the evidence is weak or absent.
Table of Contents
- What Is PABA
- The "Vitamin B10" Story
- Role in Bacterial Folate Synthesis
- Sunscreen & UV History
- Peyronie's Disease (Potaba Evidence)
- Scleroderma & Skin Fibrosis
- Hair, Skin & Pigment Claims
- Food Sources
- Dosage & Forms
- Safety, Sulfa-Drug Interaction & Cautions
- References
- Connections
- Featured Videos
1. What Is PABA
Para-aminobenzoic acid is a small, simple organic molecule with the formula C7H7NO2: a benzene ring carrying an amino group on one side and a carboxylic acid group directly opposite it (the "para" position). The compound is also called 4-aminobenzoic acid, and it is the structural parent of several well-known chemicals — including the local anesthetics procaine (Novocain) and benzocaine, which are esters of PABA. As a pure substance, PABA is a white-to-pale-tan crystalline powder that dissolves modestly in water and more readily in alcohol.
PABA is not synthesized to any meaningful degree by human tissue, and humans have no biochemical pathway that uses it for an essential purpose. The PABA that appears in human urine comes from two outside sources: small amounts in food, and far larger amounts produced by the trillions of bacteria living in the gut, which make and consume PABA as part of their own folate metabolism. Because PABA is rapidly absorbed, partly acetylated in the liver, and quickly excreted by the kidneys, a measured oral dose of PABA is sometimes used clinically as a marker to check whether a urine collection was complete — a use that has nothing to do with nutrition and everything to do with PABA's predictable pharmacokinetics.
Understanding PABA correctly starts with this distinction: it is a genuine, biologically active chemical, but its biology is overwhelmingly microbial. The reason PABA was ever called a vitamin at all is a story about early-twentieth-century animal experiments — and about how easy it is to confuse a nutrient that an animal's gut bacteria need with a nutrient that the animal itself needs.
2. The "Vitamin B10" Story
In the 1930s and 1940s, researchers feeding restricted diets to rats, mice, and chicks observed that certain animals developed poor growth, fur or feather changes, and graying of dark fur — and that adding PABA to the diet sometimes corrected these signs. On the strength of these animal findings, PABA was given vitamin-style names: "vitamin B10" and the closely related "vitamin Bx," and in some older literature "vitamin H1." For a time it was grouped with the B-complex and sold as a nutritional factor that supported skin, hair, and pigment.
The reclassification came once the underlying biochemistry was worked out. The benefit of PABA in those animals was traced not to a human-style vitamin requirement but to PABA's role as a precursor of folate — and, critically, to the fact that the animals' own intestinal bacteria were the parties that needed PABA to make folate. When the experimental diets also contained adequate folate, the apparent "PABA requirement" disappeared. In other words, PABA was acting as a raw material for a folate-synthesizing system that lives in the gut, not as an essential dietary factor for the mammal. Humans obtain folate directly from food (leafy greens, legumes, liver, fortified grains) and do not depend on making it from PABA at all.
Because of this, modern nutrition science does not classify PABA as a vitamin for humans. There is no Recommended Dietary Allowance, no Adequate Intake, no Tolerable Upper Intake Level set by nutrition authorities, and — most tellingly — no recognized human deficiency disease. Its modern status is that of a non-essential organic compound that is sometimes sold as a dietary supplement and is regulated in the United States as a drug in its prescription form (potassium para-aminobenzoate, brand name Potaba). When a label, blog, or older reference calls PABA "vitamin B10," it is using an obsolete name from a research era that has since corrected the record.
3. Role in Bacterial Folate Synthesis (and Why Humans Don't Need It)
PABA's one genuinely important biological job is to serve as a substrate in the folate (vitamin B9) biosynthesis pathway of bacteria, fungi, plants, and some protozoa. In these organisms, an enzyme called dihydropteroate synthase (DHPS) joins PABA to a pteridine intermediate to build dihydropteroate, which is then converted into dihydrofolate and ultimately the active folate coenzymes those cells need to make DNA, RNA, and certain amino acids. Researchers have even used radioactively labeled PABA to directly track folate production in Escherichia coli, confirming that PABA uptake mirrors the rate of folate synthesis in the microbe.
Humans, and animals generally, lack the DHPS enzyme entirely. We cannot build folate from PABA no matter how much PABA we consume. Instead, humans must take in pre-formed folate from the diet, transport it into cells, and recycle it. This single fact — that the bacterial folate factory exists and the human one does not — is the foundation of one of the most important classes of antibiotics ever developed.
The sulfonamide ("sulfa") antibiotics, such as sulfamethoxazole, are structural look-alikes of PABA. They competitively block dihydropteroate synthase: the bacterium's enzyme tries to use the sulfa drug as though it were PABA, the reaction stalls, and the microbe is starved of the folate it needs to grow. Because human cells do not run this pathway, the drug damages the bacterium while sparing us. This is the textbook example of selective toxicity in pharmacology — and it has a direct, practical consequence for anyone taking PABA supplements, discussed in the safety section below: supplemental PABA can flood the bacterial enzyme with its natural substrate and thereby reduce the effectiveness of sulfa antibiotics. The relationship was demonstrated experimentally in 1941, when investigators showed that adding p-aminobenzoic acid prevented the growth-inhibitory action of sulfanilamide on bacteria.
4. Sunscreen & UV History
One of PABA's most visible real-world uses was in sunscreen. PABA absorbs ultraviolet-B (UVB) radiation — the high-energy band of sunlight most responsible for sunburn — and in the mid-twentieth century it became one of the first widely used chemical sunscreen agents. It was, in fact, among the original active ingredients that made modern sunburn-preventing lotions possible, and early studies confirmed that PABA-containing sunscreens not only reduced sunburn but also blunted some of the immune changes that UVB radiation induces in skin.
Despite this effectiveness, PABA was largely phased out of consumer sunscreens, for two practical reasons. First, PABA and its derivatives caused contact allergic reactions and photosensitivity in a meaningful number of people, producing itchy, inflamed skin in those who became sensitized — sometimes cross-reacting with related "para" compounds such as certain hair dyes, anesthetics, and sulfa drugs. Second, PABA had a tendency to stain clothing a yellowish color. As newer UV filters with better cosmetic properties and lower sensitization rates became available, manufacturers moved away from PABA, and "PABA-free" became a common marketing label on sunscreens by the 1980s and 1990s.
It is worth being precise about what this history does and does not mean. PABA genuinely worked as a UVB absorber; it was not removed because it failed to protect skin. It was removed because better-tolerated alternatives existed and because a subset of users developed skin reactions. Modern sunscreens overwhelmingly use other filters, and a person today is far more likely to encounter PABA as an oral supplement or a prescription drug than as a sunscreen ingredient. The sunscreen chapter is best read as a real but closed episode in PABA's story rather than a current recommendation.
5. Peyronie's Disease (Potaba Evidence)
The most legitimate medical use of PABA is in its prescription salt form, potassium para-aminobenzoate (sold as Potaba), which has been studied for fibrotic conditions — disorders in which the body lays down excess scar-like connective tissue. The longest-standing of these is Peyronie's disease, a condition in which a plaque of fibrous tissue forms in the penis, causing curvature, pain, and difficulty with erections. Clinicians first reported treating Peyronie's disease with potassium para-aminobenzoate in the late 1950s, and the drug has remained one of the oral options discussed for the condition ever since.
The evidence is genuine but modest and mixed. A double-blind, placebo-controlled randomized trial of potassium para-aminobenzoate in men with Peyronie's disease, published in BJU International in 2007, reported that the drug significantly reduced penile plaque size and pain and helped stabilize the disease — while not reliably reversing established curvature. More recently, a 2026 retrospective comparison in the Nigerian Journal of Clinical Practice found potassium para-aminobenzoate and colchicine to be broadly comparable in everyday practice. Overall, the most defensible reading is that Potaba may help slow progression and ease pain in early, active Peyronie's disease, but it is not a cure, the curvature improvements are limited, and the long course of treatment (often a year at several grams per day) is expensive and hard to tolerate. Major urology guidelines treat oral therapies for Peyronie's disease cautiously for exactly these reasons. PABA should only be used for this purpose in its prescription form, under a urologist's supervision.
6. Scleroderma & Skin Fibrosis
The same anti-fibrotic rationale led to decades of research on potassium para-aminobenzoate in scleroderma (systemic sclerosis), an autoimmune disease in which the skin and sometimes internal organs become progressively hardened by excess collagen. The proposed mechanism is that PABA may increase the activity of an enzyme (monoamine oxidase) involved in collagen turnover and may interfere with the abnormal cross-linking of collagen fibers, theoretically softening fibrotic tissue. This made it an appealing candidate at a time when few effective treatments for scleroderma existed.
The clearest data come from the long work of Zarafonetis and colleagues. In a large retrospective analysis published in the Journal of Clinical Epidemiology in 1988, scleroderma patients treated with potassium para-aminobenzoate showed better long-term survival than untreated comparison patients, and related analyses suggested benefits for skin softening and preservation of lung function. These are meaningful observations — but they come with an important caveat: they are retrospective, not randomized. Patients were not assigned to treatment by chance, so factors other than the drug (such as which patients were healthy enough to tolerate a long course of therapy) could have influenced the results.
Later, better-controlled research tempered the enthusiasm. A prospective, randomized, double-blind, placebo-controlled trial found that potassium para-aminobenzoate did not significantly improve skin thickening in diffuse scleroderma compared with placebo. The honest summary is that PABA has a real, long-studied history in scleroderma and some suggestive retrospective survival data, but it is not an established, guideline-endorsed treatment, and modern management of systemic sclerosis relies on other agents. As with Peyronie's disease, any use here belongs to the prescription drug, not to over-the-counter supplements.
7. Hair, Skin & Pigment Claims (Weighed Honestly)
The most widely repeated folk claim about PABA is that it can restore color to gray hair or prevent further graying. This idea traces directly back to the 1930s–40s animal experiments described earlier, in which dark-furred rats and mice on deficient diets developed gray fur that sometimes re-darkened when PABA (or related B-factors such as pantothenic acid) was added back. From there the claim migrated into human supplement folklore, often bundled with the now-obsolete "vitamin B10" branding.
The evidence in humans is weak and largely anecdotal. Human graying is overwhelmingly driven by genetics and age — the gradual exhaustion of pigment-producing melanocyte stem cells in the hair follicle — and there is no robust, modern, controlled clinical trial showing that PABA supplements reverse or reliably slow this process. Even in the original animal era, the picture was contested: a 1940 report in Science, for example, found pantothenic acid ineffective against the graying of fur, illustrating how shaky the "anti-graying nutrient" claims were even at their source. Older accounts that PABA darkened gray hair in some people often involved high doses and uncontrolled observation, and any darkening tended to fade when supplementation stopped.
It is fair to say PABA is not an established remedy for gray hair, wrinkles, or skin pigment. Some people take it hoping for these cosmetic effects, but the responsible framing is that the benefit is unproven, the underlying cause of graying is not a PABA deficiency, and high-dose use carries the real risks described in the safety section. If a product promises to reverse gray hair "with vitamin B10," that promise is selling 1940s folklore, not current evidence.
8. Food Sources
Because PABA is not an essential nutrient, there is no target intake to "meet" from food, and no deficiency to avoid. Still, PABA does occur naturally in small amounts in a variety of foods, generally bound up within folate-containing compounds. Notable dietary sources include organ meats (especially liver), whole grains, brewer's yeast and nutritional yeast, eggs, mushrooms, and leafy green vegetables such as spinach. Molasses and bran are also sometimes listed.
By far the largest source of PABA in the human body, however, is not the diet at all but the gut microbiome. The bacteria in the large intestine synthesize PABA as part of their own folate metabolism, and this internally produced PABA dwarfs the trace amounts that come from food. This is another reason nutrition scientists do not treat dietary PABA as important: the body is awash in microbial PABA regardless of what is eaten, and none of it is required for human health.
The practical takeaway is that no one needs to seek out PABA-rich foods. A normal diet supplies trace amounts, gut bacteria supply far more, and the human body has no use for any of it as a vitamin. Eating liver, eggs, leafy greens, and whole grains is worthwhile for their actual nutrients — folate, B12, iron, choline, fiber — not for their PABA content.
9. Dosage & Forms
PABA is sold in two very different guises, and the distinction matters. The first is the over-the-counter dietary supplement, typically PABA powder or capsules in the range of about 100 to 500 mg per day, marketed for hair, skin, and general "B-complex" support. At these modest doses PABA is generally well tolerated by most people, but — as this page has emphasized — there is little credible evidence that supplementation provides a health benefit, because PABA is not an essential nutrient for humans.
The second form is the prescription drug potassium para-aminobenzoate (Potaba), used for Peyronie's disease and historically for scleroderma. Here the doses are far higher: clinical regimens have used roughly 12 grams per day, divided into multiple doses, taken with food and fluids and often continued for many months. These are pharmaceutical doses prescribed and monitored by a physician, not casual supplement amounts. The high pill burden, gastrointestinal upset, and cost are major reasons patients struggle to complete a full course.
If a person chooses to take a low-dose PABA supplement, taking it with food reduces stomach upset and improves tolerance. There is no benefit to "loading" high doses on one's own; the high-dose regimens belong to supervised drug therapy for specific diagnoses. Because PABA can interact with prescription medications — most importantly sulfa antibiotics — anyone considering it should review their full medication list with a pharmacist or physician first.
10. Safety, Sulfa-Drug Interaction & Cautions
At low supplemental doses (a few hundred milligrams per day), PABA is generally well tolerated. The most common complaints are mild and dose-related: nausea, loss of appetite, and other gastrointestinal upset, and occasionally skin rash or itching in people who are sensitive to "para" compounds. These usually resolve when the dose is lowered or stopped.
At the high gram-level doses used pharmaceutically, the risk profile is more serious. The most important concern is liver injury (hepatotoxicity): there are published case reports of acute hepatitis and elevated liver enzymes in patients taking potassium para-aminobenzoate at gram doses, generally reversible after the drug is discontinued. High-dose PABA has also been associated with low blood sugar, low-grade fever, and rash. For this reason, high-dose PABA should only be used under medical supervision, and it should be avoided in people with kidney or liver impairment, who clear the compound poorly.
The single most clinically important interaction is with sulfonamide ("sulfa") antibiotics. Because sulfa drugs kill bacteria by blocking the bacterial enzyme that uses PABA to build folate, taking supplemental PABA can directly antagonize and weaken these antibiotics — supplying the enzyme with the very substrate the drug is trying to withhold. Anyone taking a sulfa antibiotic (for example, sulfamethoxazole–trimethoprim) should not take PABA supplements. PABA can also interfere with certain laboratory and pharmacological measurements and may add to the effects of medications that affect blood sugar. As a general rule: low-dose PABA is mostly harmless but mostly pointless for healthy people; high-dose PABA is a prescription matter; and PABA should be kept well away from sulfa drugs.
References
- Zarafonetis, C.J.D., and Horrax, T.M. "Treatment of Peyronie's Disease with Potassium Para-Aminobenzoate (Potaba)." Journal of Urology, vol. 81, no. 6, 1959, pp. 770-772.
- Zarafonetis, C.J.D., et al. "Retrospective Studies in Scleroderma: Effect of Potassium Para-Aminobenzoate on Survival." Journal of Clinical Epidemiology, vol. 41, no. 2, 1988, pp. 193-205.
- Kervancioglu, E., et al. "Comparison of the Effectiveness of Potassium Para-aminobenzoate and Colchicine in the Treatment of Peyronie Disease: A Retrospective Study." Nigerian Journal of Clinical Practice, vol. 29, no. 4, 2026, pp. 454-458.
- Safarinejad, M.R. "Efficacy and Safety of Potassium Para-Aminobenzoate in the Treatment of Peyronie's Disease: A Randomized, Double-Blind, Placebo-Controlled Study." BJU International, 2007. PubMed search.
- Dimond, A.E. (Diamond), et al. "P-Aminobenzoic Acid Prevents the Growth-Inhibitory Action of Sulfanilamide." Science, vol. 94, no. 2444, 1941, pp. 420-421.
- King, T.E., et al. "Measurement of the Uptake of Radioactive para-Aminobenzoic Acid Monitors Folate Biosynthesis in Escherichia coli K-12." Analytical Biochemistry, vol. 216, no. 2, 1994, pp. 427-430.
- Morison, W.L. "The Effect of a Sunscreen Containing Para-Aminobenzoic Acid on the Systemic Immunologic Alterations Induced in Mice by Exposure to UVB Radiation." Journal of Investigative Dermatology, vol. 83, no. 6, 1984, pp. 405-408.
- Williams, R.J., et al. "Inefficacy of Pantothenic Acid Against the Graying of Fur." Science, vol. 92, no. 2398, 1940, pp. 561-562.
- "Potassium-Aminobenzoate: Hepatotoxicity — Case Report." Reactions Weekly, vol. 1946, 2023, p. 470.
- Gabrielsen, A.A., et al. "Potassium Para-Aminobenzoate (Potaba) in the Treatment of Diffuse Systemic Sclerosis: A Randomized, Double-Blind, Placebo-Controlled Trial." PubMed search.
- National Library of Medicine. "Para-Aminobenzoic Acid (PABA): Folate Biosynthesis, Sulfonamide Mechanism, and Clinical Pharmacology." PubMed topic search.
- Contact Dermatitis Literature. "Para-Aminobenzoic Acid (PABA) Sunscreen Photosensitivity and Allergic Contact Dermatitis." PubMed topic search.
Connections
- Former & Deprecated Vitamins
- Folate (Vitamin B9)
- Inositol (B8)
- Choline
- Vitamin C
- Urology (Peyronie's Disease)
- Rheumatology (Scleroderma)
- Dermatology & Skin Health
- Hair Loss & Hair Health
- Toxins
- Lab Tests
- Back to Vitamins