Sleep Hygiene — Temperature and Mattress
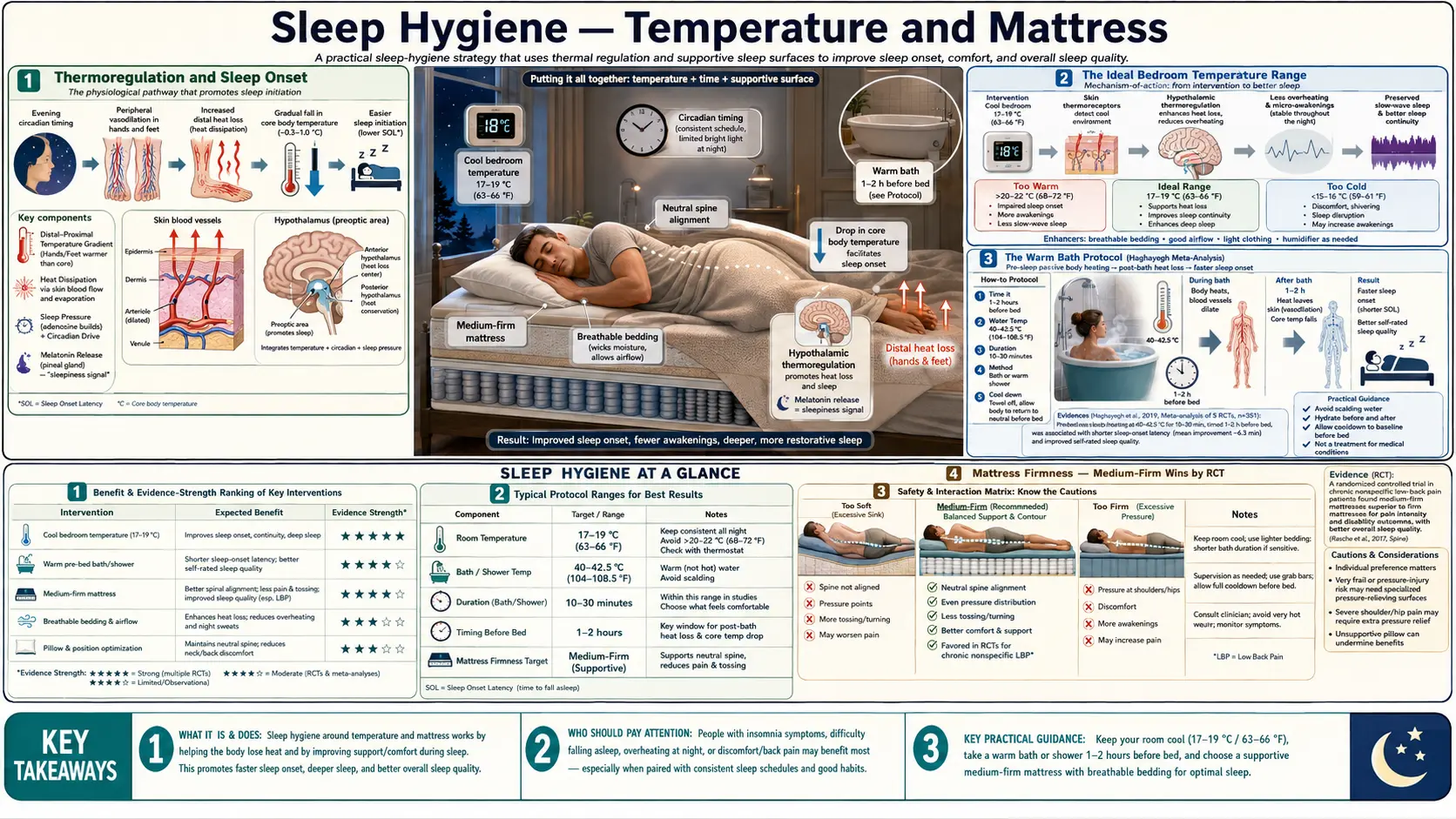
Sleep onset is gated by thermoregulation. The human core body temperature must drop by approximately 0.3°C from its daytime peak to initiate the slow-wave sleep cascade, and this drop is mediated by distal-skin vasodilation that radiates heat away from the body core. A bedroom temperature of 60–67°F (15.5–19.5°C), with a sweet spot around 65°F (18°C), is the range across which most healthy adults achieve this drop most efficiently. Two ancillary interventions help: a warm shower or bath 90 minutes before bed (the Haghayegh meta-analysis showed a 36% reduction in sleep onset latency), and a medium-firm mattress with cervical-aligning pillow. This page covers the physiology in depth, then walks through the practical decisions on thermostats, mattresses, pillows, sheets, and cooling toppers.
Table of Contents
- Thermoregulation and Sleep Onset
- The Ideal Bedroom Temperature Range
- The Warm Bath Protocol (Haghayegh Meta-Analysis)
- Mattress Firmness — Medium-Firm Wins by RCT
- Mattress Types (Innerspring, Memory Foam, Latex, Hybrid)
- Pillow Loft and Cervical Alignment
- Sheets and Bedding (Fiber, Weave, Tog)
- Cooling Toppers and Active Climate Systems
- Night Sweats, Hot Flashes, and Hot Sleepers
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Thermoregulation and Sleep Onset
Core body temperature follows a robust circadian rhythm in healthy adults, peaking at roughly 99°F (37.2°C) in the late afternoon and reaching a nadir of approximately 97.5°F (36.4°C) about 2 hours before habitual wake time. This is not incidental — sleep onset is causally gated by the descending slope of body temperature in the evening. The thermal phase shift comes from the SCN through the suprachiasmatic-paraventricular projections that regulate the sympathetic nervous system.
The mechanism of temperature drop involves distal-skin vasodilation: blood vessels in the hands and feet open, allowing warm blood to radiate heat through the skin into the environment. This is why warm hands and feet are a reliable physiological marker of imminent sleep, and why cold hands and feet at bedtime (often caused by sympathetic activation from stress or low ambient temperature) predict difficulty falling asleep. Krauchi et al. (Nature 1999, PMID 10485703) demonstrated that the ratio of distal-skin temperature to proximal-skin temperature (the "distal-proximal gradient") is the single best physiological predictor of sleep latency — warm feet and cool core predict rapid sleep onset.
Once asleep, body temperature continues to drop through the first half of the night, reaches its nadir in the second half, and begins to climb again roughly 2 hours before natural wake time. Cortisol surges in parallel with the temperature climb, producing the cortisol awakening response (CAR). Disruption of the temperature rhythm — from a too-warm bedroom, an insulating mattress, heavy bedding, or pre-bed alcohol — flattens the temperature curve and fragments sleep, particularly reducing slow-wave (deep) sleep in the first third of the night.
The Ideal Bedroom Temperature Range
Sleep researchers converge on 60–67°F (15.5–19.5°C) as the optimal bedroom temperature for most adults, with the sweet spot around 65°F (18°C). The range exists because individuals vary considerably in basal metabolic rate, body composition (more lean mass = more heat production), thyroid status, and bedding preferences.
Practical findings from Okamoto-Mizuno & Mizuno (J Physiol Anthropol 2012, PMID 22738673) and related sleep-lab studies:
- Below 60°F (15.5°C): Sleep becomes fragmented as the body must work to maintain core temperature; sympathetic activation increases; REM sleep decreases.
- 60–67°F (15.5–19.5°C): Optimal range. Slow-wave sleep is maximized; sleep onset latency is shortest; wake-after-sleep-onset (WASO) is lowest.
- 67–72°F (19.5–22°C): Generally tolerated but slow-wave sleep begins to drop and REM is preserved less well.
- Above 75°F (24°C): Substantial impairment of sleep architecture. Frequent micro-arousals, reduced slow-wave sleep, sweating-mediated dehydration.
Older adults often prefer warmer rooms by 2–5°F because of reduced basal metabolic rate and thinner skin (less efficient thermoregulation). Postmenopausal women experiencing hot flashes may need an even cooler room (60–63°F) with cooling sheets and possibly a bedside fan. Couples with mismatched preferences are well served by dual-zone climate-controlled mattress systems (Eight Sleep Pod, Sleep Number ClimateCool, Chilipad / Ooler).
The Warm Bath Protocol (Haghayegh Meta-Analysis)
The Haghayegh et al. systematic review and meta-analysis (Sleep Medicine Reviews 2019, PMID 31102877) pooled 17 RCTs of pre-bed warm-water bathing or showering. The headline finding: a 10-minute warm shower or bath at 40–42.5°C (104–108.5°F) ending 1–2 hours before bedtime produced a 36% reduction in sleep onset latency on average, and improved subjective sleep quality.
The mechanism is counterintuitive. The warm water does not cool you down directly — it warms you up. But the warm bath causes massive distal-skin vasodilation, and when you step out of the bath and into cooler ambient air, the dilated peripheral vessels radiate heat away from the body core extremely efficiently. The net effect over the next 1–2 hours is a faster and deeper core-body-temperature drop than would occur naturally, accelerating the thermal trigger for sleep onset.
Practical protocol:
- Timing: 60–120 minutes before intended bedtime is optimal. Closer to bedtime fails because the temperature drop is incomplete; further away fails because the effect has dissipated.
- Temperature: 104–108°F (40–42°C). Hot enough to feel pleasantly warm but not scalding.
- Duration: 10–20 minutes. Long enough to warm the body core; short enough to be practical.
- Post-bath: Towel off, change into light cool pajamas, lower bedroom thermostat if possible.
- Footbath alternative: Liao et al. (PubMed: Liao footbath) showed a 20-minute warm footbath at the same temperature produces comparable effects in older adults who cannot easily get in and out of a tub.
Magnesium-rich Epsom salt baths are popular but the magnesium contribution is largely irrelevant (transdermal absorption is minimal); the sleep benefit comes from the thermal effect alone.
Mattress Firmness — Medium-Firm Wins by RCT
The Kovacs et al. trial (Lancet 2003, PMID 14630439) is the landmark RCT on mattress firmness. 313 adults with chronic non-specific low back pain were randomized to a firm mattress (Hf 2.3 on the European scale) or medium-firm (Hf 5.6) for 90 days. The medium-firm group had significantly less daytime pain, less in-bed pain, and less disability. The conclusion: medium-firm mattresses outperform very firm ones for both pain and sleep quality in adults with non-specific back pain.
Jacobson et al. studies of new bedding systems consistently found that replacing an old mattress (9+ years) with any modern medium-firm mattress reduced perceived back pain and improved sleep quality. The take-home: mattress age and condition matter more than brand. The average mattress useful lifespan is 7–10 years; visible sagging, body impressions deeper than 1.5 inches, or springs poking through indicate a worn-out mattress regardless of age.
Mattress firmness intersects with body weight: heavier individuals (over 230 lb / 105 kg) generally need firmer mattresses to prevent excessive sinking; lighter individuals (under 130 lb / 60 kg) often find very firm mattresses uncomfortable because they cannot compress the surface enough to relieve pressure points. Side sleepers benefit from slightly softer surfaces (pressure relief at hip and shoulder); back and stomach sleepers benefit from slightly firmer surfaces (lumbar support).
Mattress Types (Innerspring, Memory Foam, Latex, Hybrid)
The four major mattress categories each have characteristic profiles:
- Innerspring: Traditional coil-based construction. Excellent airflow (sleeps cool), good edge support, moderate pressure relief, moderate durability (5–8 years typical lifespan). Best for: hot sleepers, heavier individuals, those wanting traditional feel and bounce.
- Memory foam: Viscoelastic polyurethane foam. Excellent pressure relief and motion isolation; tends to sleep warm without phase-change materials or gel infusions; 7–10 year lifespan. Best for: side sleepers, couples (motion isolation), those with joint pain. Avoid for: hot sleepers (unless cooling formulation).
- Latex: Natural or synthetic rubber foam. Most durable category (10–15+ years for natural latex); excellent pressure relief with more bounce than memory foam; cooler than memory foam; expensive. Best for: those wanting longevity, allergy sufferers (natural latex is dust-mite resistant), eco-conscious buyers.
- Hybrid: Innerspring coil base + foam or latex comfort layers on top. Combines coil airflow and edge support with foam pressure relief; 7–10 year lifespan. Best for: most buyers seeking a versatile general-purpose mattress.
The choice of mattress type is highly individual — no single material is best for everyone. The most important tactic is buying from a vendor with a generous trial period (90–365 nights). The body takes 2–4 weeks to adapt to a new sleep surface; impressions in the first few nights are unreliable.
Pillow Loft and Cervical Alignment
The pillow's job is to keep the cervical spine in neutral alignment with the thoracic spine during sleep. Pillow height (loft) requirements differ dramatically by sleep position:
- Back sleepers: Low to medium loft (3–5 inches). The pillow should fill the space between the head and the mattress without tilting the head forward. A contoured cervical pillow with a depression for the head and a roll under the neck is often ideal.
- Side sleepers: Medium to high loft (5–7 inches). The pillow must fill the wider gap between the head and the mattress created by the shoulder. Broader-shouldered sleepers need taller pillows. The head should be level with the spine, not tilted up or down.
- Stomach sleepers: Very low loft or no pillow. Most pillows force the cervical spine into hyperextension when stomach sleeping. Stomach sleeping is best avoided due to chronic cervical strain; transitioning to side sleeping is often a high-leverage hygiene change.
- Combination sleepers: Adjustable-loft pillows (shredded memory foam or buckwheat hulls) that can be added to or removed from a zippered shell are most flexible.
Pillow lifespan is 1–3 years for polyester, 3–5 years for memory foam, 5–10 years for latex or buckwheat. A flattened pillow that no longer springs back when folded is past its useful life. A leg pillow (small wedge between the knees for side sleepers; pillow under the knees for back sleepers) is a low-cost addition that often substantially reduces morning back pain.
Sheets and Bedding (Fiber, Weave, Tog)
Sheets and bedding contribute meaningfully to bed-surface temperature. Key variables:
- Fiber: Cotton (especially long-staple Egyptian or Pima) and linen are the most breathable. Linen actively wicks moisture and feels cool to the touch year-round. Bamboo lyocell is breathable and antimicrobial. Synthetic microfiber (polyester) traps heat and moisture — avoid for hot sleepers.
- Weave: Percale (one-over-one-under) is crisp and cool; sateen (four-over-one-under) is silkier but warmer. For hot sleepers, percale beats sateen for the same fiber.
- Thread count: Quality matters more than thread count. Above 400–500 thread count, additional threads come from low-quality multi-ply yarns. Reputable 200–400 thread count single-ply long-staple cotton outperforms 1000-thread-count multi-ply.
- Comforter / duvet tog rating: Tog is a unit of thermal insulation. Light summer comforter: 4.5 tog or lower. All-season: 10.5 tog. Winter / cold-climate: 13.5 tog or higher. Mismatched tog is a frequent cause of sleep-disrupting overheating.
The Scandinavian "two-duvet" system — each partner under their own duvet rather than sharing — resolves mismatched-tog disputes and reduces sleep disruption from a partner's movements.
Cooling Toppers and Active Climate Systems
For chronic hot sleepers, passive cooling toppers (phase-change material, gel-infused memory foam, gel beads in pillows) provide modest cooling for the first 30–60 minutes after lying down, then equilibrate with body temperature. Helpful but limited.
Active climate-controlled mattress pads (Chilipad, Ooler, Eight Sleep Pod) circulate water at user-set temperatures (55–110°F / 13–43°C) through tubes embedded in a topper. These can independently cool each side of the bed, programmable to drop temperature in the first half of the night and rise gently before wake. Cost: $1,500–$3,500. Reports from users with menopausal hot flashes, postmenopausal night sweats, or who simply run hot are consistently positive in this category.
A simpler, cheaper alternative is a bedside fan or ceiling fan on low, providing air circulation that aids evaporative cooling without dropping room temperature uncomfortably.
Night Sweats, Hot Flashes, and Hot Sleepers
Persistent night sweats severe enough to soak through pajamas or sheets warrant clinical evaluation. Common causes include perimenopause/menopause, hyperthyroidism, lymphoma (especially Hodgkin), tuberculosis, HIV, GERD, anxiety disorders, and medications (SSRIs, opioid withdrawal, certain antihypertensives). New-onset night sweats in an adult without an obvious cause merit a primary-care visit including basic labs and lymph-node exam.
For perimenopausal/postmenopausal hot flashes, in addition to bedroom cooling: layered breathable nightwear that can be quickly removed; avoidance of alcohol, spicy foods, and large meals in the evening (all triggers); cognitive behavioral therapy for menopause (CBT-Meno); SSRI/SNRI pharmacotherapy if indicated; and discussion of menopause hormone therapy where appropriate.
Cautions
- Persistent back pain after mattress change: If a new mattress has not improved or has worsened pain after 4–6 weeks, the mattress is wrong for you. Use the trial period to return or exchange.
- Pregnancy and side sleeping: After 20 weeks of gestation, left-side sleeping is recommended to optimize uterine blood flow. A pregnancy wedge pillow under the abdomen and between the knees adds comfort.
- Recent surgery, fractures, or severe arthritis: Mattress decisions should be made in consultation with physical therapy or orthopedics. Adjustable beds may be indicated.
- Severe hot flashes or night sweats: See above; not a sleep-hygiene problem alone, may indicate an underlying medical condition.
- Sleep apnea: Sleeping prone or supine can worsen positional OSA; side sleeping may improve it. If snoring or witnessed apneas are noted, formal evaluation should not be delayed by mattress shopping.
Key Research Papers
- Haghayegh S et al., Before-bedtime passive body heating by warm shower or bath to improve sleep: A systematic review and meta-analysis (Sleep Med Rev 2019) — PMID 31102877
- Krauchi K et al., Warm feet promote the rapid onset of sleep (Nature 1999) — PMID 10485703
- Okamoto-Mizuno K, Mizuno K, Effects of thermal environment on sleep and circadian rhythm (J Physiol Anthropol 2012) — PMID 22738673
- Kovacs FM et al., Effect of firmness of mattress on chronic non-specific low-back pain: randomised, double-blind, controlled, multicentre trial (Lancet 2003) — PMID 14630439
- Raymann RJ et al., Skin deep: enhanced sleep depth by cutaneous temperature manipulation (Brain 2008) — PMID 18192289
- Lack LC et al., The relationship between insomnia and body temperatures (Sleep Med Rev 2008) — PMID 18603220
- Liao WC et al., A warm footbath before bedtime and sleep in older Taiwanese with sleep disturbance — PubMed: Liao footbath
- Jacobson BH et al., Effect of prescribed sleep surfaces on back pain and sleep quality — PubMed: Jacobson sleep surface
- Onen SH et al., Prevention and treatment of sleep disorders through regulation of sleeping habits — PubMed: Onen sleep regulation
- Van Someren EJ, More than a marker: interaction between the circadian regulation of temperature and sleep, age-related changes, and treatment possibilities — PubMed: Van Someren temperature
- Murphy PJ, Campbell SS, Nighttime drop in body temperature: a physiological trigger for sleep onset? (Sleep 1997) — PMID 9415943
- Buman MP et al., Sitting and television viewing: novel risk factors for sleep disturbance and anxiety (Mental Health and Physical Activity) — PubMed: Buman sitting and sleep
Connections
- Sleep Hygiene Benefits Hub
- Sleep Hygiene (Main)
- Circadian Light Exposure
- Caffeine Cutoff Timing
- Sleep Tracking Tech
- Insomnia
- Sleep Apnea
- Meditation
- Breathing Exercises
- Magnesium Glycinate
- Valerian
- Chamomile
- Ashwagandha
- L-Theanine
- Glycine
- All Remedies