Cold and Flu Natural Treatments: History and Origins
Unlike a remedy with a single inventor, the treatment of colds and flu has no founder. It is one of the oldest projects in the whole history of medicine — the running effort of dozens of cultures, across thousands of years, to ease a runny nose, a sore throat, a cough, and a fever. This article tells that story honestly: the ancient roots of honey, willow, garlic, and elderflower; the slow scientific separation of "the cold" from "the flu" and the 1933 isolation of the influenza virus; the named people behind the modern naturopathic staples (George Eby and zinc lozenges, Linus Pauling and high-dose vitamin C, the elderberry trials of Zichria Zakay-Rones, the revival of echinacea); and the arrival of real antiviral drugs. Throughout, it states plainly what the evidence does and does not support — because the single most important historical fact about the common cold is that, after all this time, there is still no cure for it.
Table of Contents
- A Remedy With No Founder
- Ancient Roots: Honey, Willow, Garlic, and Elderflower
- Naming the Enemy: "Influenza" and the Cold
- Elderberry: From Hippocrates to the Zakay-Rones Trials
- Echinacea: A Plains Medicine Goes Global
- Linus Pauling and the Vitamin C Era
- George Eby and the Zinc Lozenge
- The Arrival of Real Antivirals
- Evidence and Reception: What Actually Holds Up
- Research Papers and References
- Connections
- Featured Videos
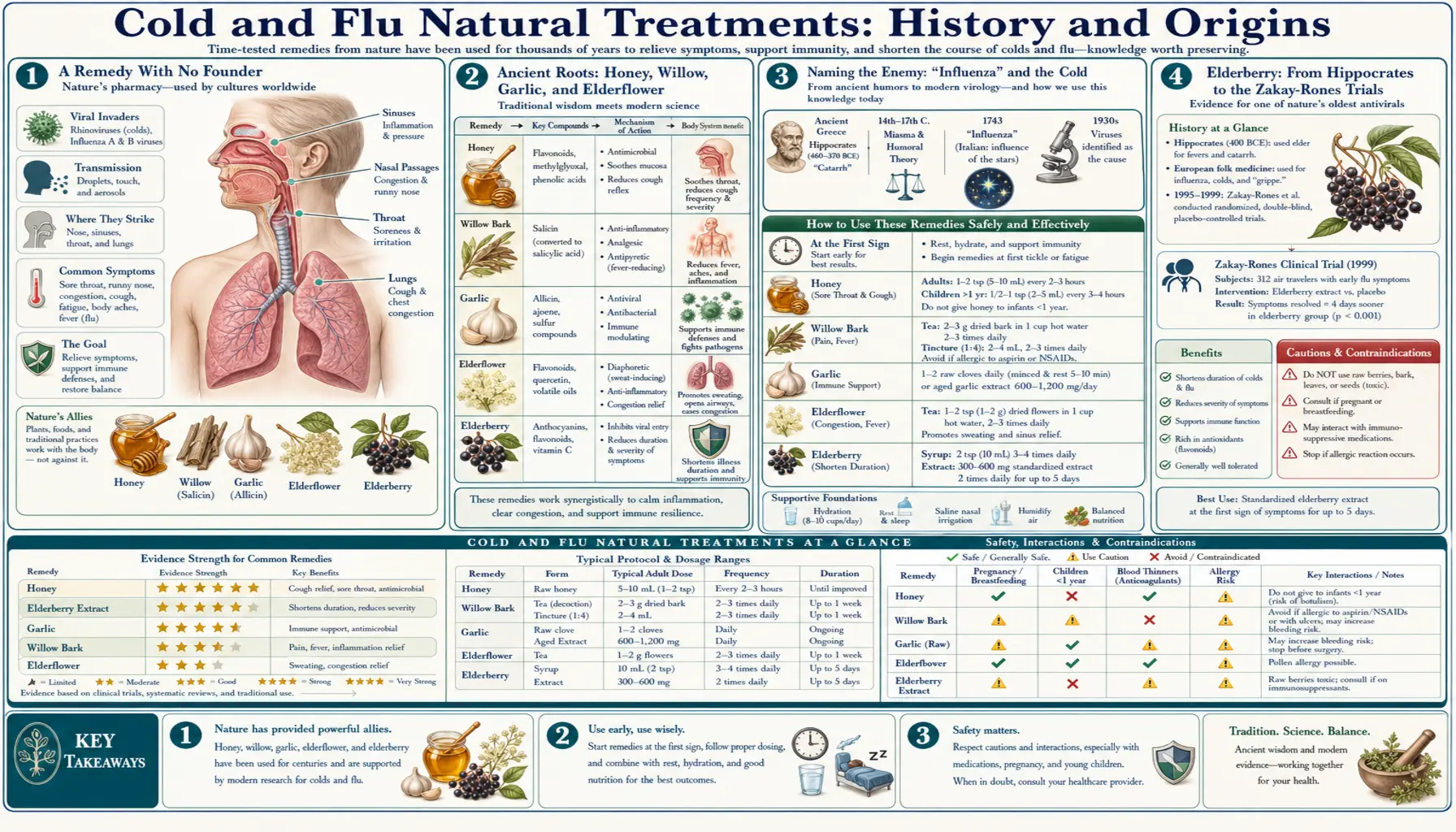
A Remedy With No Founder
Many of the remedies on this site can be traced to a single person — a physician who built a protocol, a chemist who isolated a molecule, a practitioner who put their name on a method. The natural treatment of colds and flu is not like that. There is no founder, no inventor, and no origin date. The reason is simple: respiratory infections are among the most universal experiences in human life, and every culture that ever kept records left behind its own folk remedies for them. The honest history is therefore not a biography but a layering — ancient kitchen and garden remedies at the bottom, centuries of trial-and-error tradition in the middle, and a thin top layer of modern science that has tested a handful of those old ideas and added a few genuinely new tools.
It is worth saying at the outset what that modern science has and has not delivered. Researchers have learned to tell colds and influenza apart, to identify and grow the viruses that cause them, to make vaccines against influenza, and to develop antiviral drugs that modestly shorten the flu. But despite a century of intensive effort and enormous commercial incentive, there is still no cure for the common cold, and the natural remedies in this story range from "modestly supported" to "popular but unproven." This article names the real people and real milestones where they exist, and is equally careful to flag where a remedy's reputation outruns its evidence.
Ancient Roots: Honey, Willow, Garlic, and Elderflower
The oldest layer of cold-and-flu treatment is the one we still reach for: warmth, sweetness, soothing drinks, and a small set of plants. Honey appears in the medical record of ancient Egypt and runs through Greek medicine as well; the writings attributed to Hippocrates (c. 460–370 BCE) describe honey, often combined with vinegar or herbs, for coughs and sore throats. That a spoonful of honey still tops many modern lists of cough remedies is a striking piece of continuity — and one of the better-supported ones, as the evidence section notes.
Willow bark is an even older thread, and an important one, because it connects this folk history to a famous modern drug. The bark and leaves of the willow (Salix) were used for pain and fever by the ancient Sumerians and Egyptians more than three thousand years ago, and their fever-reducing use was recorded by Hippocrates and later by the Greek physician Dioscorides in the first century CE. The active principle, a compound called salicin, was isolated from willow bark in 1828 (the French pharmacist Henri Leroux and the German pharmacist Johann Buchner are both credited with early purifications), and in 1838 the Italian chemist Raffaele Piria converted it into salicylic acid. That chain — willow → salicin → salicylic acid — eventually led to aspirin, still one of the most common things people take for the aches and fever of a cold or flu; the fuller drug story is told on the dedicated Aspirin page.
Garlic (Allium sativum) is named in Egyptian, Greek, and many other ancient traditions as a remedy for infection and chest complaints, and elderflower and elderberry (Sambucus nigra) carry their own deep folk pedigree for feverish colds — a story important enough to get its own section below. The honest framing for all of these is the same: long, continuous, cross-cultural use tells us these remedies were trusted and available, not that they were ever proven by the standards we now expect. Tradition raises the question; it does not answer it.
Naming the Enemy: "Influenza" and the Cold
For most of history, a "cold" and "the flu" were not clearly separated, and neither was understood to be caused by a virus — a category that did not yet exist. The word influenza itself records an older theory of disease: it is Italian for "influence," and reflects the medieval and Renaissance belief that epidemics came from the influence of the stars or of the cold (influenza di freddo). The term spread into English in the eighteenth century. The first widely cited epidemic that clearly matches influenza dates to 1580, and devastating pandemics recurred over the following centuries — most catastrophically the 1918–1919 pandemic, which killed tens of millions of people worldwide.
The decisive scientific step came in the twentieth century. In 1933, at Britain's National Institute for Medical Research, the researchers Wilson Smith, Christopher Andrewes, and Patrick Laidlaw isolated the influenza A virus by transmitting it to ferrets — the first time the cause of the flu had been captured and grown in the laboratory. Influenza B was identified a few years later, in 1936, by Thomas Francis Jr. Identifying the virus is what eventually made influenza vaccines and, much later, antiviral drugs possible, and it is what finally put the long-blurred distinction between "a bad cold" and "the flu" on a firm biological footing. (The common cold, it turned out, is caused not by one virus but by many — rhinoviruses above all — which is a large part of why it has never yielded to a single cure or vaccine.)
Elderberry: From Hippocrates to the Zakay-Rones Trials
Among the herbal cold remedies, elderberry has one of the longest and best-documented arcs. The elder plant was valued in ancient Egypt and Greek medicine; Hippocrates is traditionally said to have called it his "medicine chest," and elderflower's use as a diaphoretic — a remedy that promotes sweating to help break a fever — runs through European folk medicine for centuries. Indigenous peoples of North America likewise used native elder species for coughs and colds. For most of that history, elderberry was tradition, not tested medicine.
The modern chapter is tied to a specific researcher: the Israeli virologist Zichria Zakay-Rones. In 1995, Zakay-Rones and colleagues published a study reporting that an elderberry extract inhibited several strains of influenza virus in the laboratory and appeared to shorten symptoms during an outbreak of influenza B in Panama. In 2004, a second, more rigorous randomized, double-blind, placebo-controlled trial of 60 flu patients in Norway reported that those taking elderberry syrup recovered, on average, about four days sooner than those on placebo. These trials are the foundation of elderberry's modern reputation as a flu remedy and of the commercial extracts sold today.
Honesty requires two cautions. First, these were small studies, several connected to a particular branded product, and larger independent trials have been called for; elderberry is best described as promising but not definitively proven. Second, raw or unripe elder berries, leaves, and bark contain cyanogenic compounds and can cause nausea and vomiting if eaten uncooked — properly prepared syrups and cooked products are what the traditional and clinical use refers to. The deeper mechanism and dosing detail live in the companion Elderberry and Antiviral article.
Echinacea: A Plains Medicine Goes Global
Echinacea's history is a clear example of a Native American medicine entering, and then dividing, Western practice. The coneflowers (Echinacea species) are native to North America, and Indigenous peoples of the Great Plains used the roots, leaves, and flowers for a wide range of complaints, including coughs, sore throats, and infections. The plant crossed into settler medicine in the late nineteenth century largely through H. C. F. Meyer, a German lay practitioner in Nebraska who, around 1870, learned of its use and began selling a patent medicine he called "Meyer's Blood Purifier," promoting echinacea extravagantly as a near-cure-all.
In 1887 Meyer brought echinacea to the attention of two prominent figures in American Eclectic medicine in Cincinnati — the pharmacist John Uri Lloyd and the physician John King — and through the Lloyd Brothers pharmaceutical house it became one of the most popular medicines in the United States in the early twentieth century. As mainstream medicine turned toward antibiotics, echinacea faded in America but was taken up in Germany, where in the 1930s Gerhard Madaus introduced a commercial preparation marketed as Echinacin and conducted some of the first laboratory and clinical work on the genus. Most modern echinacea research has European roots in that lineage.
The cautionary note here is about evidence rather than safety. Echinacea is one of the most-studied cold herbs, yet its trial results are famously inconsistent — in large part because studies have used different species (E. purpurea, E. angustifolia, E. pallida), different plant parts, and very different preparations, so they are not really testing the same thing. That heterogeneity, more than any single negative result, is why echinacea's standing remains genuinely unsettled.
Linus Pauling and the Vitamin C Era
No single person did more to popularize a cold remedy than the chemist Linus Pauling (1901–1994), one of the most celebrated scientists of the twentieth century and a winner of two Nobel Prizes (Chemistry in 1954, Peace in 1962). Late in his career, Pauling became convinced that very large daily doses of vitamin C (ascorbic acid) could prevent and treat the common cold, and in 1970 he laid out the case in a best-selling book, Vitamin C and the Common Cold, published by W. H. Freeman. The book launched the modern vitamin-C-for-colds movement and helped make high-dose supplementation a household habit.
The honest assessment of this episode is mixed, and it matters. Pauling's book was written for the general public and rested heavily on his own reasoning and personal experience rather than on strong clinical trials; mainstream medicine criticized him at the time for promoting an unproven megadose therapy to a mass audience ahead of the evidence. A related figure, the physician Robert Cathcart, popularized the idea of taking vitamin C up to "bowel tolerance" — very large divided doses — during illness, an approach that remains a naturopathic staple but has never been validated in controlled trials. As the evidence section below explains, decades of subsequent research found that Pauling was partly right and substantially over-optimistic: routine vitamin C does not stop people from catching colds, though it may modestly shorten them.
George Eby and the Zinc Lozenge
The zinc lozenge has one of the most precisely datable origin stories in this whole field, and it begins not in a laboratory but with a sick child. In 1979, an American researcher named George Eby gave his three-year-old daughter — who was being treated for leukemia and had a bad cold — a zinc tablet to dissolve in her mouth because she could not swallow it whole. Her cold symptoms, by his account, cleared within hours. That chance observation, repeated informally many times, led Eby to design a formal trial.
In 1984, Eby and colleagues (D. R. Davis and W. W. Halcomb) published a double-blind, placebo-controlled study in the journal Antimicrobial Agents and Chemotherapy reporting that zinc gluconate lozenges shortened the duration of colds dramatically — in their data, by around seven days. The result electrified the field and launched the entire category of zinc cold lozenges. But it also kicked off decades of difficulty: over the following years, roughly a dozen further trials gave conflicting results, with about half showing benefit and half showing none. Later analysis traced much of this to chemistry — whether the lozenge actually releases free zinc ions in the mouth depends heavily on the zinc salt used and on additives such as citric acid that bind the zinc and neutralize it. The mechanism and the formulation details are covered in the companion Zinc Acetate Lozenges article.
The Arrival of Real Antivirals
The natural and folk remedies above all aim to ease symptoms or support the body; the twentieth century also produced drugs that attack the influenza virus directly. The first was amantadine, introduced in the mid-to-late 1960s as the earliest antiviral active against influenza A. It worked but had real limitations, and widespread resistance eventually made it largely obsolete for flu.
The bigger breakthrough came from understanding the virus's structure. Once the three-dimensional shape of the influenza enzyme neuraminidase was worked out, chemists could design molecules to block it. This produced the neuraminidase inhibitors: zanamivir (Relenza), registered in 1999, followed by oseltamivir (Tamiflu) in 2000. These drugs can shorten influenza when started early, and they are genuinely modern, rationally designed medicines — though their real-world benefit, especially in otherwise healthy people, has itself been the subject of major scientific debate. Importantly, none of these antivirals work against the common cold, which is not caused by influenza viruses at all. This is the dividing line in the whole history: against the flu, medicine eventually built specific weapons; against the cold, it is still, for the most part, managing symptoms and waiting for the immune system to win.
Evidence and Reception: What Actually Holds Up
Because this site values truth over promotion, the most useful thing a history can do is state plainly where the evidence has landed after all this time. The fairest summary, drawing on Cochrane systematic reviews and other high-quality analyses, is that the popular natural cold-and-flu remedies are modestly helpful at best, and several are unproven.
- Vitamin C. The 2013 Cochrane review (Hemilä and Chalker) of trials in more than 11,000 people found that taking vitamin C regularly does not reduce how often most people catch colds, but it does modestly shorten them — by roughly 8% in adults and 14% in children. Taking vitamin C only after a cold has already started has not been shown to help. So Pauling was partly vindicated and largely overstated.
- Zinc. Some trials show zinc lozenges shorten colds when started very early and formulated correctly; others show nothing. A 2024 Cochrane review concluded that the overall evidence remains insufficient to firmly recommend zinc for preventing or treating colds — an honest reflection of forty years of conflicting results.
- Elderberry. Supported mainly by small trials (notably Zakay-Rones 1995 and 2004) suggesting faster flu recovery; promising but not definitively established, and in need of larger independent confirmation.
- Echinacea. Heavily studied but inconsistent, largely because trials used different species and preparations. Some prevention regimens look beneficial; the picture overall is unsettled.
- Honey. One of the better-supported traditional remedies: reasonable evidence that honey eases cough, particularly nighttime cough in children (with the firm caveat that honey must never be given to infants under one year, because of the risk of infant botulism).
- Homeopathic flu products such as Oscillococcinum are widely sold but are not supported by good scientific evidence, and their proposed mechanism is not accepted by mainstream science.
Two themes run through the whole record. First, timing dominates: the remedies with any signal of benefit (zinc, echinacea, the first-day protocols) generally show it only when started at the very first symptoms. Second, and most important, none of this is a cure. After thousands of years of honey and willow and elderflower, and a century of vaccines, antivirals, and vitamins, the common cold remains stubbornly undefeated — which is why the sober goal of natural treatment is comfort, support, and modest shortening of illness, not conquest. Anyone with a high-risk condition, a very high or prolonged fever, breathing difficulty, or symptoms that worsen after improving should seek medical care rather than rely on self-treatment.
Research Papers and References
The list below combines key peer-reviewed sources on the history and evidence of cold-and-flu remedies with curated PubMed topic-search links. Historical figures and primary sources (Hippocrates, Dioscorides, and the early chemists of willow and salicin) are named in the article as historical sources rather than as modern citations. Author names, titles, and journals are given as plain text; only the stable DOI, PMID, or archive link is hyperlinked, and each opens in a new tab.
- Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews. 2013;(1):CD000980. — doi:10.1002/14651858.CD000980.pub4 · PMID: 23440782
- Eby GA, Davis DR, Halcomb WW. Reduction in duration of common colds by zinc gluconate lozenges in a double-blind study. Antimicrobial Agents and Chemotherapy. 1984;25(1):20-24. — PMID: 6367635
- Zakay-Rones Z, Varsano N, Zlotnik M, et al. Inhibition of several strains of influenza virus in vitro and reduction of symptoms by an elderberry extract (Sambucus nigra L.) during an outbreak of influenza B Panama. Journal of Alternative and Complementary Medicine. 1995;1(4):361-369. — PMID: 9395631
- Zakay-Rones Z, Thom E, Wollan T, Wadstein J. Randomized study of the efficacy and safety of oral elderberry extract in the treatment of influenza A and B virus infections. Journal of International Medical Research. 2004;32(2):132-140. — doi:10.1177/147323000403200205 · PMID: 15080016
- Eby GA. Zinc lozenges as cure for the common cold — a review and hypothesis. Medical Hypotheses. 2010;74(3):482-492. — PMID: 19906491
- Pauling L. Vitamin C and the Common Cold. San Francisco: W. H. Freeman; 1970. — Internet Archive
- History of cold and influenza remedies — PubMed: common cold history and treatment
- Influenza history and antiviral development — PubMed: influenza history and antivirals
External Authoritative Resources
- NCCIH — Cold and Flu: Complementary Approaches
- CDC — Influenza (Flu)
- Cochrane Library — Vitamin C for the common cold
Connections
- All Remedies
- Cold and Flu Natural Treatments
- Cold and Flu Treatments Benefits
- Immune Boosting
- Aspirin
- Elderberry
- Echinacea
- Vitamin C
- Zinc
- Influenza