Chiropractic Care
Chiropractic is a licensed health profession that focuses on the muscles, joints, and bones of the body — especially the spine. Its signature treatment is spinal manipulation, also called an adjustment: a quick, controlled push applied to a joint, often producing an audible pop. Many people find real relief from ordinary back and neck pain through chiropractic care, and for those complaints the research is genuinely supportive. But chiropractic also carries a century of controversy, because the idea it was founded on — that misaligned vertebrae cause disease throughout the body — has not held up to scientific testing. This page tries to be scrupulously fair: it separates what chiropractic does well from what it has overpromised, explains what an adjustment actually is and feels like, and is honest about safety, including the rare but serious risk tied to forceful neck manipulation. The goal is to help you decide when a chiropractor is a reasonable choice and when you should see a medical doctor first.
Table of Contents
- What Chiropractic Care Is
- A Brief, Honest History
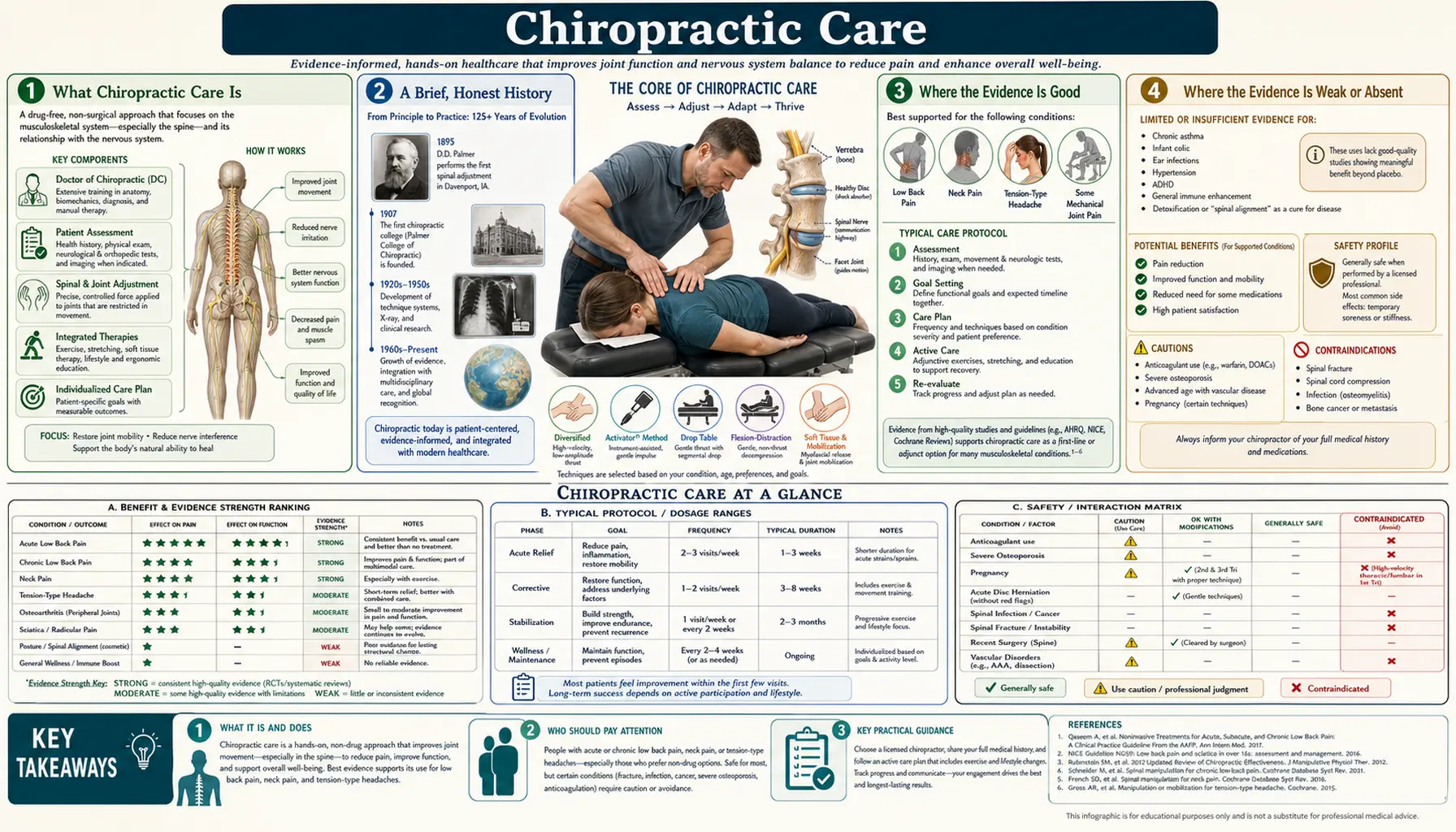
- Where the Evidence Is Good
- Where the Evidence Is Weak or Absent
- What an Adjustment Is & What to Expect
- Safety: Common, Rare, and Serious Risks
- Neck Manipulation and Stroke
- Who Benefits & When to See a Doctor First
- How It Fits With Evidence-Based Care
- Choosing a Chiropractor Wisely
- The Honest Bottom Line
- Research Papers
- Connections
- Featured Videos
What Chiropractic Care Is
Chiropractic is a regulated healthcare profession centered on the musculoskeletal system — the network of muscles, ligaments, joints, and bones that lets you move — with a particular emphasis on the spine. In most countries a chiropractor must complete a multi-year doctoral program, pass board examinations, and hold a license to practice. The title "Doctor of Chiropractic" (DC) reflects that training, though it is not the same as a medical degree (MD or DO).
The core tool of the profession is spinal manipulative therapy (SMT). In an adjustment, the practitioner uses their hands or a small instrument to move a joint quickly through a short distance, usually to the end of its normal range. Chiropractors also use related techniques — slower joint mobilization, soft-tissue and muscle work, stretching, exercise instruction, and advice on posture and activity. In practice, good chiropractic care for back or neck pain looks a lot like other forms of conservative, hands-on physical care.
It helps to hold two ideas at once. As a set of manual techniques for mechanical back and neck problems, chiropractic is a mainstream, evidence-supported option. As a theory of disease — the historical claim that the spine is the gateway to overall health — it is not supported by evidence. Much of the confusion around chiropractic comes from mixing those two things together.
A Brief, Honest History
Chiropractic began in Davenport, Iowa, in 1895, when a magnetic healer named Daniel David (D.D.) Palmer reported restoring a janitor's hearing by adjusting his spine. From that single anecdote Palmer built an entire system. He proposed that a life force he called "Innate Intelligence" flowed through the nerves, that misaligned vertebrae — which he named vertebral subluxations — pinched those nerves and blocked the flow, and that correcting the subluxations by hand could cure disease throughout the body. His son B.J. Palmer turned the idea into a movement and a thriving school.
It is important to be clear-eyed about this origin. The subluxation theory was not derived from anatomy, physiology, or experiment; it was a metaphysical idea from the era before modern medicine. As the science of the nervous system and the spine advanced, the theory did not gain support — the "subluxations" Palmer described cannot be reliably found on imaging and do not correspond to a demonstrated cause of illness.
The profession has spent more than a century in tension over this legacy. Many modern chiropractors are essentially evidence-based spine and musculoskeletal clinicians who have largely set the old theory aside and practice much like physical therapists. A smaller group still centers care on detecting and correcting subluxations and promotes broad, whole-body health claims. When you evaluate a chiropractor, it is worth knowing which tradition they draw from — it strongly shapes what they will offer you and what they will claim.
Where the Evidence Is Good
Here is the genuinely good news, and it deserves to be stated plainly: for ordinary low-back pain and neck pain, spinal manipulation is a reasonable, evidence-supported treatment.
For acute (recent) low-back pain, a 2017 systematic review and meta-analysis in JAMA pooled 26 randomized trials and found that spinal manipulation produced modest improvements in pain and function, on par with other recommended first-line treatments, without serious adverse events in the trials reviewed (Paige 2017). For chronic low-back pain, a large 2019 meta-analysis in The BMJ concluded that SMT gives short-term improvements in pain and function roughly comparable to other recommended therapies such as exercise (Rubinstein 2019). Cochrane reviews — the gold standard of careful evidence synthesis — reach similar, measured conclusions: manipulation is about as helpful as other common conservative options, not a miracle and not useless (Rubinstein 2012).
For neck pain, a Cochrane review found that manipulation and mobilization can reduce pain and improve function in the short term, and that combining manual therapy with exercise tends to work better than either alone (Gross 2015).
Crucially, this evidence has made its way into mainstream clinical guidelines. The American College of Physicians recommends starting with non-drug options for low-back pain — and lists spinal manipulation among the reasonable choices alongside exercise, heat, massage, and acupuncture (Qaseem 2017). A pragmatic trial in active-duty military members found that adding chiropractic care to usual medical care improved pain and disability more than usual care alone (Goertz 2018). In other words, for the right complaint, chiropractic is not fringe — it sits squarely within accepted conservative care.
Two honest caveats keep this in perspective. First, the benefits are typically modest and short-term, similar to other good conservative treatments rather than dramatically better than them. Second, mechanical back and neck pain often improves on its own within weeks, so some of what people credit to an adjustment is natural recovery. That does not make the treatment worthless — feeling better sooner and moving more comfortably is a real benefit — but it argues for realistic expectations.
Where the Evidence Is Weak or Absent
Now the other half of an honest account. Several long-standing chiropractic claims are not supported by evidence, and it is important to name them.
The subluxation theory itself. The founding idea — that tiny spinal misalignments block nerve flow and cause disease — has never been validated. The "subluxations" described by traditional chiropractic cannot be reliably identified, and there is no demonstrated mechanism by which correcting them would cure illness elsewhere in the body.
Treating non-musculoskeletal disease. The claim that spinal adjustments can treat conditions unrelated to the muscles and joints — such as asthma, ear infections, infant colic, allergies, high blood pressure, digestive disorders, bed-wetting, or immune problems — is not supported by good clinical trials. Where these conditions have been studied, manipulation has generally shown no meaningful benefit beyond placebo. Parents in particular should be cautious of clinics that offer chiropractic as a treatment for a child's asthma, colic, or recurrent infections.
"Maintenance" and lifelong adjustment schedules. There is little good evidence that frequent adjustments in people without symptoms prevent future problems or keep you healthy. A recommendation for open-ended, indefinite visits — especially bundled into a large prepaid package — is a reason for healthy skepticism rather than a sign of thorough care.
Routine full-spine X-rays. Repeated X-rays to hunt for subluxations expose you to radiation without changing the treatment for ordinary back or neck pain. Imaging has a real place — ruling out fracture, tumor, or infection when red-flag symptoms are present — but not as a routine screen on every visit.
None of this means a good chiropractor is a bad clinician. It means the specific promises matter. Care aimed at your aching back or stiff neck rests on solid ground; care sold as a cure for asthma or a lifetime health-maintenance program does not.
What an Adjustment Is & What to Expect
A spinal adjustment — clinicians call it a high-velocity, low-amplitude thrust — is a fast, small, targeted push applied to a joint, usually taking it just past its normal range of motion. The technique is quick and precise rather than forceful over a long distance.
The familiar popping sound is not a bone being "cracked" or a vertebra snapping back into place. It is cavitation: a small gas bubble forms and collapses in the fluid inside the joint as the pressure changes, much like the pop of a knuckle. The sound is harmless and, importantly, is not a measure of whether the treatment worked.
A typical first visit includes a history and physical examination, questions about how the pain started and what makes it better or worse, and screening for warning signs that call for medical work-up. A reasonable treatment course for a mechanical complaint is usually a defined number of visits over a few weeks, with a clear plan to reassess: if you are meaningfully better, care winds down; if you are not improving after a short trial, that is a signal to change course rather than to keep going indefinitely. Alongside adjustments, expect soft-tissue work, stretches, exercise advice, and guidance on posture and daily activity — the parts of care that help you stay better between visits.
Safety: Common, Rare, and Serious Risks
For most people receiving care for the low back, chiropractic is generally safe. A systematic review of chiropractic safety found that serious adverse events are rare and that the most common effects are mild and temporary (Gouveia 2009).
Common and minor. The most frequent side effect is short-lived soreness, stiffness, or a headache in the day or two after an adjustment — reported by a substantial share of patients but usually mild and self-resolving, much like the ache after a new workout (Paanalahti 2014). This is expected and not a cause for alarm.
Uncommon but real. Forceful manipulation can occasionally aggravate an existing problem. In people with a herniated disc, severe osteoporosis, spinal instability, inflammatory arthritis affecting the spine, or bones weakened by cancer, aggressive manipulation can do harm and is generally not appropriate. A careful chiropractor screens for these before treating.
Rare and serious. The most serious concern is tied specifically to manipulation of the neck, and it deserves its own honest discussion below.
Reviews of adverse events emphasize two themes: serious harms are uncommon, but they are also under-reported, so the true rate is not known with precision (Ernst 2007). That uncertainty is a reason for careful screening and informed consent — not a reason to either dismiss the risk or to exaggerate it.
Neck Manipulation and Stroke
This is the part of chiropractic that requires the most care to describe accurately, because it is easy to either frighten people or to wave the concern away. Neither is fair. Here is what the evidence actually shows.
The concern is a rare event called cervical artery dissection — a small tear in the inner wall of one of the arteries that run up through the neck to the brain (most often the vertebral artery). A tear can lead to a clot and, in the worst case, a stroke. Warning signs can include a sudden, unusual, severe headache or neck pain, dizziness, double vision, slurred speech, or trouble with balance and coordination.
What is genuinely debated is cause versus coincidence. A large population-based study compared people who had this type of stroke with people who did not, and found that those who saw a chiropractor were more likely to have also seen a primary-care doctor in the days beforehand — suggesting that in many cases the artery may have already been tearing, producing the neck pain and headache that sent the person to seek care in the first place (Cassidy 2008). In that reading, the manipulation did not cause the dissection; the early dissection caused the symptom that led to the visit. Other analyses reach similar conclusions and note that the association with chiropractic visits is similar to the association with primary-care visits (Whedon 2015).
At the same time, the risk cannot be dismissed. Case reviews document dissections and strokes that followed neck manipulation, and biologically it is plausible that a forceful rotational thrust could injure a vulnerable artery (Kranenburg 2017). The honest synthesis is this: a stroke caused by neck manipulation is very rare — estimates are on the order of roughly one per hundreds of thousands to millions of manipulations — its causal role is uncertain and debated, but it is real enough to warrant caution.
Practical takeaways that respect both the rarity and the seriousness: a good practitioner discusses this risk and obtains informed consent before manipulating the neck; gentler mobilization and non-thrust techniques are reasonable alternatives to a high-velocity neck thrust; anyone who develops a sudden severe headache, neck pain, dizziness, or neurological symptoms after a neck adjustment should seek emergency care immediately; and if you arrive for care already having an unusual new headache or neck pain, that symptom itself deserves a medical evaluation rather than a manipulation.
Who Benefits & When to See a Doctor First
Reasonable candidates. Chiropractic is a sensible option for uncomplicated mechanical low-back or neck pain — the everyday aches, stiffness, and strains that make up most spine complaints — particularly if you prefer a hands-on, drug-free approach and want to stay active. It fits naturally into a plan built around movement and exercise.
See a medical doctor first if any of these "red flags" are present. These can signal a problem that needs urgent evaluation, and manipulation is not the answer:
- New loss of bladder or bowel control, or numbness in the groin/saddle area (a possible medical emergency).
- Progressive weakness, numbness, or tingling in an arm or leg.
- Back or neck pain following a significant injury, fall, or car accident.
- Fever, unexplained weight loss, or a history of cancer along with new back pain.
- A sudden, severe, "worst-ever" headache or neck pain, or pain with dizziness, slurred speech, or vision changes.
- Known severe osteoporosis, spinal instability, or bones weakened by disease.
For children, and for any non-musculoskeletal illness — asthma, infections, colic, allergies, digestive complaints — the right first stop is a pediatrician or physician, not a chiropractor. Chiropractic care is not a substitute for evaluating and treating disease.
How It Fits With Evidence-Based Care
The most useful way to think about chiropractic is as one tool within conservative musculoskeletal care — not a rival to medicine and not a complete health system on its own. For back and neck pain, the treatments with the best evidence overlap heavily: staying active, guided exercise, physical therapy, manual therapy (including manipulation and massage), heat, and time. Guidelines increasingly favor this whole toolkit over rushing to imaging, opioids, or surgery for ordinary spine pain (Qaseem 2017).
In that light, chiropractic and physical therapy are more complementary than competing. Both use hands-on techniques and exercise; the biggest predictor of a good outcome is often not which profession you choose but whether the clinician screens carefully, sets realistic goals, and gets you moving rather than keeping you dependent on passive treatment. A chiropractor who coordinates with your physician, welcomes exercise, and refers you onward when needed is practicing exactly the kind of integrated care the evidence supports.
The framing to be wary of is the opposite one: a practice that positions adjustments as an alternative to mainstream medicine, discourages standard care, or treats the spine as the master switch for all health. That is the part of chiropractic's history that the science left behind.
Choosing a Chiropractor Wisely
If you decide to try chiropractic, a few practical habits protect you and improve your odds of benefit:
- Match the claim to the evidence. Care aimed at back or neck pain is well-founded. Be skeptical of promises to treat asthma, allergies, infections, or "boost immunity" through adjustments.
- Expect a real exam and a time-limited plan. A good first visit includes history-taking and screening for red flags, and a course of care with a point to reassess — not an open-ended commitment.
- Be cautious of large prepaid packages. Dozens of prepaid "maintenance" visits for someone without symptoms are a business model, not a treatment supported by evidence.
- Question routine repeat X-rays. Imaging should answer a specific question (like ruling out fracture when red flags exist), not screen for "subluxations" on every visit.
- Ask about the neck. If neck manipulation is proposed, expect a discussion of risks and alternatives, and feel free to request gentler mobilization instead of a forceful thrust.
- Watch for improvement. If a short trial of care is not helping, that is a reason to change the plan or seek a medical opinion — not to keep going indefinitely.
The Honest Bottom Line
Chiropractic care earns a genuinely mixed but fair verdict. For mechanical low-back and neck pain, spinal manipulation is a reasonable, evidence-supported part of conservative care — roughly as helpful as other good non-drug options, endorsed in mainstream guidelines, and generally safe. Many people are helped, and there is no need to be dismissive of that.
At the same time, the founding subluxation theory is not supported by evidence, and claims that adjustments treat asthma, infections, colic, allergies, or disease throughout the body should be treated with skepticism. The rare but serious risk associated with forceful neck manipulation is real enough to warrant caution and informed consent, even though its causal role is debated. And red-flag symptoms belong to a doctor, not an adjustment table.
Used for what it does well — and kept away from what it has overpromised — chiropractic is a legitimate, useful option for common back and neck pain. Judge it by the specific problem you bring and the specific claims you are offered, and it can be a sound choice within a broader, evidence-based plan.
Research Papers
- Paige NM, Miake-Lye IM, Booth MS, et al. Association of spinal manipulative therapy with clinical benefit and harm for acute low back pain: systematic review and meta-analysis. JAMA. 2017;317(14):1451–1460. doi:10.1001/jama.2017.3086 — pooled 26 trials; SMT gave modest pain/function benefit for acute low-back pain, comparable to other first-line options.
- Rubinstein SM, de Zoete A, van Middelkoop M, et al. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of randomised controlled trials. BMJ. 2019;364:l689. doi:10.1136/bmj.l689 — for chronic low-back pain, SMT produced short-term improvement similar to other recommended treatments such as exercise.
- Rubinstein SM, Terwee CB, Assendelft WJJ, et al. Spinal manipulative therapy for acute low-back pain. Cochrane Database Syst Rev. 2012;(9):CD008880. doi:10.1002/14651858.CD008880.pub2 — Cochrane review found SMT no more or less effective than other common conservative therapies for acute low-back pain.
- Gross A, Langevin P, Burnie SJ, et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst Rev. 2015;(9):CD004249. doi:10.1002/14651858.CD004249.pub4 — manipulation/mobilization can reduce neck pain short-term; combining manual therapy with exercise works best.
- Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367 — mainstream guideline listing spinal manipulation among reasonable non-drug options for low-back pain.
- Goertz CM, Long CR, Vining RD, et al. Effect of usual medical care plus chiropractic care vs usual medical care alone on pain and disability among US service members with low back pain: a comparative effectiveness clinical trial. JAMA Netw Open. 2018;1(1):e180105. doi:10.1001/jamanetworkopen.2018.0105 — adding chiropractic care to usual care improved pain and disability more than usual care alone.
- Bronfort G, Haas M, Evans R, et al. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopat. 2010;18:3. doi:10.1186/1746-1340-18-3 — broad review: manipulation helps spine-related pain but evidence is lacking for most non-musculoskeletal conditions.
- Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34(11):E405–E413. doi:10.1097/BRS.0b013e3181a16d63 — serious adverse events are rare; most effects are mild and transient, but reporting is incomplete.
- Ernst E. Adverse effects of spinal manipulation: a systematic review. J R Soc Med. 2007;100(7):330–338. doi:10.1177/014107680710000716 — catalogs reported serious harms and stresses that under-reporting makes true risk hard to quantify.
- Cassidy JD, Boyle E, Côté P, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine (Phila Pa 1976). 2008;33(4 Suppl):S176–S183. doi:10.1097/BRS.0b013e3181644600 — stroke risk after chiropractic visits mirrored risk after primary-care visits, suggesting early dissection prompts the visit rather than manipulation causing the stroke.
- Whedon JM, Song Y, Mackenzie TA, et al. Risk of stroke after chiropractic spinal manipulation in Medicare B beneficiaries aged 66 to 99 years with neck pain. J Manipulative Physiol Ther. 2015;38(2):93–101. doi:10.1016/j.jmpt.2014.12.001 — found no excess stroke risk attributable to manipulation compared with primary-care visits in older adults.
- Kranenburg HA, Schmitt MA, Puentedura EJ, et al. Adverse events associated with the use of cervical spine manipulation or mobilization and patient characteristics: a systematic review. Musculoskelet Sci Pract. 2017;28:32–38. doi:10.1016/j.msksp.2017.01.008 — reviews reported cervical-manipulation adverse events, including artery dissection, and the difficulty of predicting who is at risk.
Connections
- Acupuncture
- Massage Therapy
- Exercise
- Low Back Pain
- Sciatica
- Herniated Disc
- Osteoarthritis
- Stroke
- Migraine
- Orthopedics
- Neurology
- All Remedies