Zinc Toxicity (Excess Zinc): Weakened Immunity
Zinc has a reputation as the “immune mineral,” so it surprises people to learn that taking too much of it, for too long, can quietly do the opposite — leaving you catching more infections, healing more slowly, and feeling generally run-down. The twist is that excess zinc rarely harms immunity directly. Instead, a steady overdose drives down copper, a metal your bone marrow needs to build white blood cells, and it is the resulting copper shortage that hollows out your defenses. This is almost always self-inflicted — large daily supplements, zinc lozenges used for months, or zinc-laden denture creams — not something you can get from food. This page explains how a chronic zinc excess weakens immunity, why the symptom is so easy to misread, the warning signs, and how the problem is confirmed and reversed.
Table of Contents
- What Zinc-Driven Immune Weakness Feels Like
- The Mechanism: How Excess Zinc Starves Your Immune Cells
- Honesty: Frequent Infections Have Many Causes
- Clues That Point Toward Excess Zinc
- Where the Excess Zinc Comes From
- Getting Checked
- How Zinc Excess and Its Immune Effects Are Reversed
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Zinc-Driven Immune Weakness Feels Like
This is not a sudden illness. Immune weakness from chronic zinc excess creeps in over weeks to months, and it tends to feel less like “getting sick” and more like your body's defenses have lost a step. Because the cause is slow, most people do not connect it to the supplement bottle on the shelf — especially when that supplement was started for the very purpose of helping immunity.
The pattern people describe usually includes some mix of:
- Catching everything that goes around. More frequent colds, sore throats, sinus infections, and skin or urinary infections than is normal for you — and infections that drag on longer or bounce back after seeming to clear.
- Slow, stubborn healing. Cuts, scrapes, and mouth ulcers that take longer to close, sometimes with repeated minor skin infections, because the same white cells that fight germs also do the cleanup work of healing.
- A vague, sapped feeling. Unusual fatigue, pallor, or feeling washed-out — often because the copper shortage behind the immune problem is also causing anemia, so the white-cell and red-cell problems arrive together.
- Blood-test surprises. Frequently the first real clue is not a feeling at all but a routine blood count showing a low white-cell count (especially low neutrophils, the front-line bacteria-fighters) and often a low red-cell count alongside it.
Notice what is missing from that list: there is no pain, no fever that points to the cause, no single dramatic symptom that says “zinc.” The experience is one of gradual, unexplained vulnerability. That vagueness is exactly why this problem is so often missed for months — and why the next section, on honesty about other causes, matters so much.
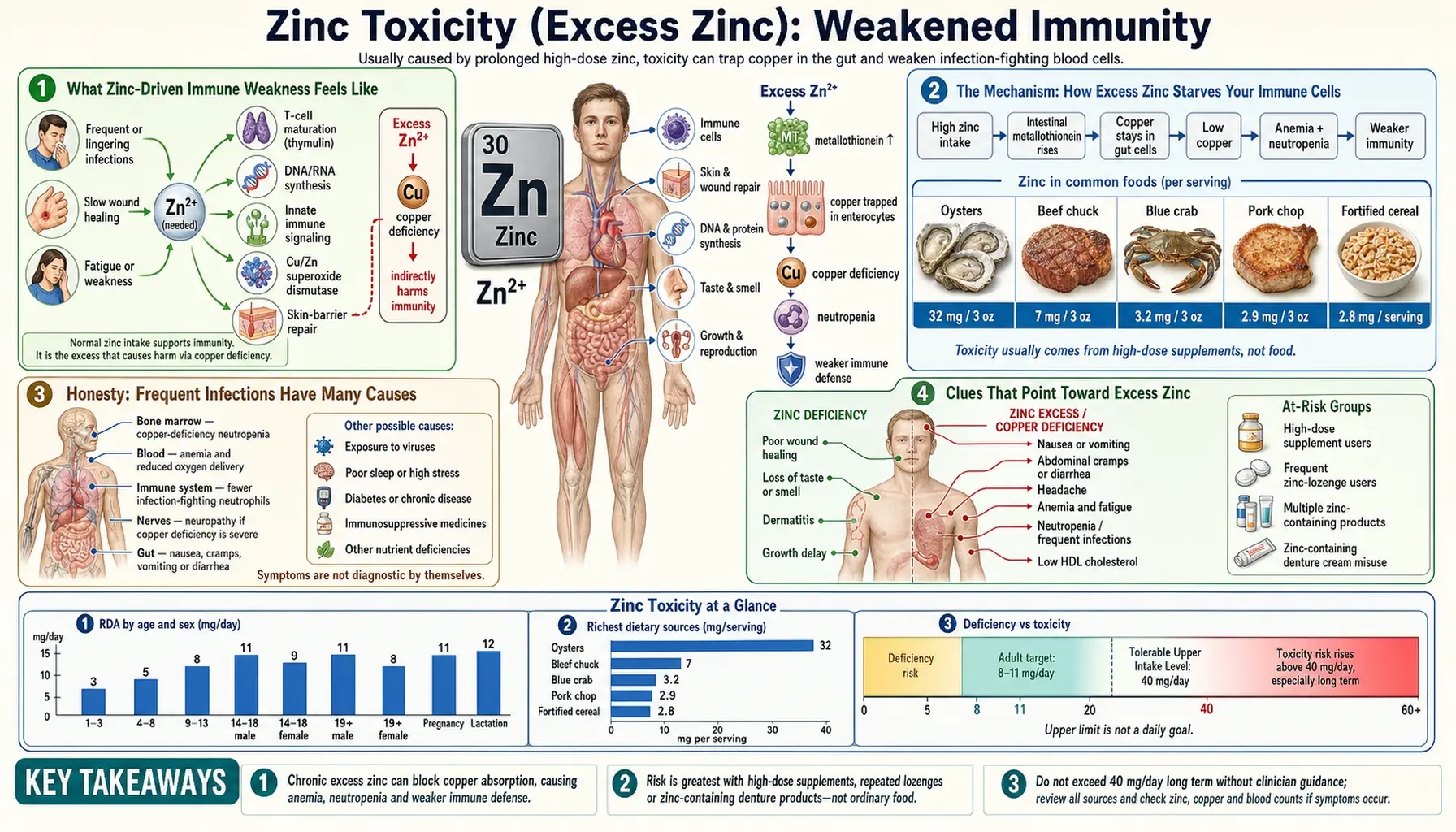
The Mechanism: How Excess Zinc Starves Your Immune Cells
To understand why too much of the immune mineral can weaken immunity, it helps to hold two facts together. First, zinc genuinely is essential for immune function — it is a structural cofactor in hundreds of enzymes and in the immune system's signaling, and a true zinc deficiency badly impairs the body's defenses. Second, the body's need for zinc follows a narrow curve: too little is harmful, the right amount is essential, and too much is also harmful. The harm at the high end works almost entirely through a different metal — copper.
The copper connection. Zinc and copper are absorbed in the same stretch of small intestine and partly compete for the same uptake. When zinc intake is chronically high, the lining cells of the gut respond by producing a binding protein called metallothionein, which has a stronger grip on copper than on zinc. The metallothionein latches onto dietary copper and holds it inside the intestinal cells, which are then shed back into the gut and lost in the stool. In effect, a steady excess of zinc sets a copper trap: more zinc → more metallothionein → more copper captured and discarded → falling body copper. This is the well-described mechanism of zinc-induced copper deficiency, and it is covered in its own right on the companion page, Zinc Toxicity and Copper Deficiency.
Why a copper shortage hits immunity. Copper is not a bystander — your bone marrow needs it to manufacture blood cells. When copper runs low, the production line for neutrophils (the white cells that swallow and kill bacteria) falters, and the blood count drops — a state called neutropenia. Fewer neutrophils means fewer front-line soldiers, so ordinary bacteria that your body would normally brush aside are more likely to take hold and cause infection. The same copper-starved marrow typically also under-produces red cells, which is why anemia and a low white count so often appear together in this condition.
An analogy. Picture your immune system as a fire department, with neutrophils as the firefighters. Copper is the training academy that turns out new recruits, and zinc, in the right amount, is the fuel that keeps the trucks running. A modest amount of fuel is essential. But pour in far too much fuel for too long and it floods the academy next door — copper — shutting down recruitment. The trucks may be gassed up, but the station slowly empties of firefighters. When the next fire (an infection) breaks out, there simply aren't enough people to answer the call. Cut the fuel back to a sane level and reopen the academy — restore copper — and the station refills over the following weeks.
There is a second, smaller piece to the story. At very high concentrations, zinc can also directly disturb the function and signaling of immune cells, because the metal that normally fine-tunes their enzymes and receptors becomes a blunt instrument when present in excess. But in real-world human cases, the dominant, repeatedly documented pathway to weakened immunity is the copper one — the marrow being starved of the metal it needs to build white cells.
Honesty: Frequent Infections Have Many Causes
It would be misleading to suggest that catching a lot of infections means you have zinc poisoning. The opposite is true: among all the reasons a person gets sick more often, excess zinc is an uncommon one. Frequent infections, slow healing, and a low white-cell count are non-specific — they are the final common pathway of dozens of conditions, most of which are far more likely than zinc overload. Being honest about that is the whole point of this section, because chasing the wrong cause wastes time, and missing a serious one can be dangerous.
Far more common explanations for recurrent infections and a low white-cell count include:
- Common viral infections, which can transiently lower white-cell counts and leave you feeling run-down for weeks afterward.
- Medications, a huge category — chemotherapy, many immune-suppressing drugs, some antibiotics, certain thyroid and seizure medicines, and others can lower neutrophils directly.
- Autoimmune disease, such as lupus, in which the body destroys its own white cells.
- Bone-marrow and blood disorders, including the conditions doctors most need to exclude — aplastic anemia, myelodysplastic syndromes, and leukemia — which is precisely why an unexplained low blood count is taken seriously.
- Poorly controlled diabetes, which blunts the function of immune cells and raises infection risk.
- Other nutritional deficiencies, notably vitamin B12 or folate deficiency, which impair white- and red-cell production in their own right.
- True zinc deficiency, the more familiar nutritional cause of impaired immunity — the mirror image of this page — covered on the zinc deficiency hub.
So the honest framing is this: if your immunity seems weakened, the first job is a proper medical work-up to rule out the common and the serious causes — not to assume a supplement is to blame. Excess zinc earns a place on the list only when the specific clues in the next section are present. It is a real, reversible cause worth catching, but it is the exception, not the rule.
Clues That Point Toward Excess Zinc
Because frequent infections are so non-specific, excess zinc moves up the list of suspects only when the surrounding picture fits. The single most important clue is also the most obvious one, and yet it is routinely overlooked: a history of taking a lot of zinc. The features that, taken together, should raise the possibility include:
- A clear high-zinc exposure. Daily zinc supplements well above the recommended limit, often 50–150 mg or more per day; zinc lozenges or nasal products used for weeks or months rather than a few days; high-dose “immune,” prostate, or eye-health formulas; or heavy long-term use of a zinc-containing denture adhesive cream — a classic and frequently missed source.
- Low white and red counts together. The combination of neutropenia (low neutrophils) and anemia on the same blood count is a recognizable signature of copper deficiency, and far more suggestive than a low white count alone.
- A documented low copper level. When testing shows low serum copper and a low ceruloplasmin (the main copper-carrying protein), with a normal-to-high zinc level, the chain from zinc to copper to immune cells becomes hard to dispute.
- Neurological symptoms creeping in. Severe, prolonged copper deficiency can also damage the spinal cord, producing numbness, tingling, and unsteady walking (a “copper myelopathy”). When that neurological picture accompanies a low blood count in someone taking a lot of zinc, it is a strong pointer — and a reason not to delay.
One clue that does not help is how you feel day to day, since the symptoms overlap with everything else. This is a diagnosis made by connecting the exposure to the blood counts and the copper studies — not by symptoms in isolation. If those threads line up, the closely related copper-deficiency story on the companion page fills in the rest, and a digestive history of nausea and stomach upset from the same high-dose zinc can be another supporting detail.
Where the Excess Zinc Comes From
A reassuring fact sits underneath this whole topic: you essentially cannot reach harmful zinc levels by eating food. Even zinc-rich foods like oysters, beef, and pumpkin seeds do not deliver enough to overwhelm copper. Chronic zinc excess is, with rare exceptions, a product of concentrated supplements and products. For context, the recommended dietary allowance for adults is roughly 8–11 mg per day, and the tolerable upper limit — the most an average adult should get from all supplemental sources combined — is 40 mg per day. The common sources of trouble are:
- High-dose zinc supplements. Single tablets of 50 mg are sold over the counter, and some people take more than one, or stack a standalone zinc on top of a multivitamin and a separate “immune” formula — quietly pushing total intake far past 40 mg a day for months on end.
- Zinc lozenges and cold remedies used too long. Lozenges may be reasonable for a few days at the start of a cold, but taken continuously through a long winter they can add up to a large cumulative dose. (Zinc-containing intranasal cold products carry a separate, well-documented risk of permanent loss of smell and are best avoided entirely.)
- Denture adhesive creams. Some adhesive creams contain zinc, and people who use large amounts daily — reapplying throughout the day, often because of ill-fitting dentures — can absorb a surprisingly large zinc load over years. This is one of the best-documented real-world causes of zinc-induced copper deficiency and neurological injury, and it is easy to miss unless someone specifically asks about denture products.
- Specialty and combination products. Some prostate-health, eye-health (high-dose AREDS-style), and athletic formulas carry substantial zinc, which is easy to overlook when tallying total daily intake across several products.
The practical lesson is to add up zinc from every source — multivitamin, standalone supplement, lozenges, specialty formula, and denture cream — not just the bottle labeled “zinc.” For most adults, routine supplemental zinc has no proven benefit and is best kept at or below the 40 mg upper limit unless a clinician has identified a specific reason and is monitoring for it.
Getting Checked
Confirming that excess zinc is behind weakened immunity is a step-by-step process that links your history to a few inexpensive blood tests. No single result proves it; it is the pattern that makes the case.
The work-up usually unfolds like this:
- A complete blood count (CBC) with differential. This is the cornerstone. It measures neutrophils and the other white cells along with red cells and platelets, and the telltale finding is neutropenia with anemia — low white and low red counts together. This pattern is what should prompt a clinician to think about copper, and from there about zinc.
- Copper and ceruloplasmin levels. If the blood count fits, the next step is to measure serum copper and ceruloplasmin. Both being low supports copper deficiency as the cause of the blood changes.
- A serum zinc level. A zinc level that is normal or high, sitting alongside the low copper, closes the loop — pointing to zinc as the reason copper is being driven down.
- A careful exposure history. Arguably the most decisive “test” is simply a thorough review of supplements, lozenges, specialty formulas, and — crucially — denture-cream use. The diagnosis often hinges on someone asking the right question.
- Excluding the serious mimics first. Because an unexplained low blood count can signal a primary bone-marrow disorder, clinicians make sure those are considered. A Comprehensive Metabolic Panel and other routine labs help build the broader picture, and in some cases a bone-marrow examination is needed before excess zinc is accepted as the explanation.
The reassuring part is that, once the exposure and the copper studies are recognized together, this is a satisfying diagnosis to make — because it is so directly reversible. The diagnostic logic overlaps heavily with the copper-deficiency page, which goes deeper into the copper studies themselves.
How Zinc Excess and Its Immune Effects Are Reversed
The treatment is refreshingly logical: remove the cause and replace what was lost. Because the immune weakness is driven by copper depletion, and because the blood-forming machinery recovers once copper is restored, most people see their counts climb back toward normal over weeks to a few months. The steps, done under medical guidance, are:
- Stop the excess zinc. This is the single most important move — discontinue high-dose zinc supplements, stop overusing lozenges, and switch away from a zinc-containing denture cream to a zinc-free adhesive. Removing the source ends the copper trap so the body can hold onto copper again.
- Replace copper. Copper supplementation — oral in most cases, intravenous in severe or malabsorptive ones — refills the depleted stores and lets the bone marrow resume normal production of white and red cells. Clinicians choose the dose and route based on how low the copper is and how the person responds.
- Monitor the recovery. Follow-up blood counts and repeat copper and ceruloplasmin levels track the response. The neutrophil count and anemia typically improve first and fairly reliably; once recovered, copper supplements are usually tapered while the diet and any remaining zinc intake are kept sensible.
- Address any lasting nerve damage. The blood abnormalities are highly reversible. The neurological injury of long-standing copper deficiency, however, may only partly recover — which is the strongest argument for catching and treating the problem early, before nerve damage has had time to set in.
Going forward, prevention is mostly a matter of restraint: keep total supplemental zinc at or below the 40 mg daily upper limit unless a clinician advises otherwise, treat zinc lozenges as a short-term tool rather than a daily habit, and — if you wear dentures — choose a zinc-free adhesive. For nearly everyone, a varied diet supplies all the zinc the immune system needs, and more is not better.
When to Seek Care / Red Flags
Frequent infections are usually a nuisance rather than an emergency, but certain features mean you should not wait — both because a serious cause must be excluded and because copper deficiency is most reversible when caught early. Seek medical care promptly if you notice:
- A high or persistent fever with signs of a real infection — shaking chills, a spreading area of red, hot, painful skin, severe sore throat, burning with urination, or feeling severely unwell — especially if you know your white-cell count is low. Significant neutropenia with fever is a medical emergency, because infection can escalate quickly when neutrophils are scarce.
- Infections that are unusually frequent, severe, or slow to clear for you — a clear change from your normal pattern — which warrants a blood count to look for an underlying problem.
- An unexplained low white-cell count on a routine test, particularly when paired with anemia. This combination should never be brushed off; it deserves a work-up that includes copper studies and a review of your zinc intake.
- New numbness, tingling, weakness, or unsteady walking, especially alongside a low blood count and a history of heavy zinc or denture-cream use. This can signal copper-deficiency damage to the spinal cord and should be evaluated without delay, since this kind of nerve injury may not fully reverse.
And the simplest, most empowering action of all: if you take a lot of zinc — from any source — tell the clinician evaluating your infections or your blood count. That one sentence can turn a baffling, drawn-out work-up into a quick fix. When in doubt, an honest inventory of every supplement and product you use is the fastest route to the answer.
Key Research Papers
- Fosmire GJ (1990). Zinc toxicity. The American Journal of Clinical Nutrition;51(2):225-227. — DOI: 10.1093/ajcn/51.2.225
- Wessels I, Maywald M, Rink L (2017). Zinc as a Gatekeeper of Immune Function. Nutrients;9(12):1286. — DOI: 10.3390/nu9121286
- Shankar AH, Prasad AS (1998). Zinc and immune function: the biological basis of altered resistance to infection. The American Journal of Clinical Nutrition;68(2):447S-463S. — DOI: 10.1093/ajcn/68.2.447S
- Prasad AS, Beck FWJ, Bao B, et al. (2007). Zinc supplementation decreases incidence of infections in the elderly: effect of zinc on generation of cytokines and oxidative stress. The American Journal of Clinical Nutrition;85(3):837-844. — DOI: 10.1093/ajcn/85.3.837
- Fraker PJ, King LE (2004). Reprogramming of the Immune System During Zinc Deficiency. Annual Review of Nutrition;24:277-298. — DOI: 10.1146/annurev.nutr.24.012003.132454
- Skrajnowska D, Bobrowska-Korczak B (2019). Role of Zinc in Immune System and Anti-Cancer Defense Mechanisms. Nutrients;11(10):2273. — DOI: 10.3390/nu11102273
- McCall KA, Huang CC, Fierke CA (2000). Function and Mechanism of Zinc Metalloenzymes. The Journal of Nutrition;130(5):1437S-1446S. — DOI: 10.1093/jn/130.5.1437S
- Kumar N (2006). Copper Deficiency Myelopathy (Human Swayback). Mayo Clinic Proceedings;81(10):1371-1384. — DOI: 10.4065/81.10.1371
- Willis MS, Monaghan SA, Miller ML, et al. (2005). Zinc-Induced Copper Deficiency: A Report of Three Cases Initially Recognized on Bone Marrow Examination. American Journal of Clinical Pathology;123(1):125-131. — PubMed
- Wapnir RA (1998). Copper absorption and bioavailability. The American Journal of Clinical Nutrition;67(5 Suppl):1054S-1060S. — PubMed
- National Institutes of Health, Office of Dietary Supplements. Zinc — Health Professional Fact Sheet (toxicity, tolerable upper intake level, and copper interaction). — NIH Office of Dietary Supplements
PubMed Topic Searches
- PubMed — Zinc-induced copper deficiency and neutropenia
- PubMed — Excess zinc and immune suppression
- PubMed — Denture-cream zinc, copper deficiency, and myeloneuropathy
- PubMed — Zinc, copper, and intestinal metallothionein
- PubMed — Zinc supplementation, upper intake level, and toxicity
Connections
- Zinc Toxicity Symptom Hub
- Zinc Toxicity and Copper Deficiency
- Zinc Toxicity and Nausea & Stomach Upset
- Zinc Deficiency Symptom Hub
- Zinc Overview
- Zinc and Immune Function
- Copper
- Anemia
- Vitamin B12
- Comprehensive Metabolic Panel