Uranium and Depleted Uranium Toxicity: Chemical Nephrotoxicity and Radiological Risk
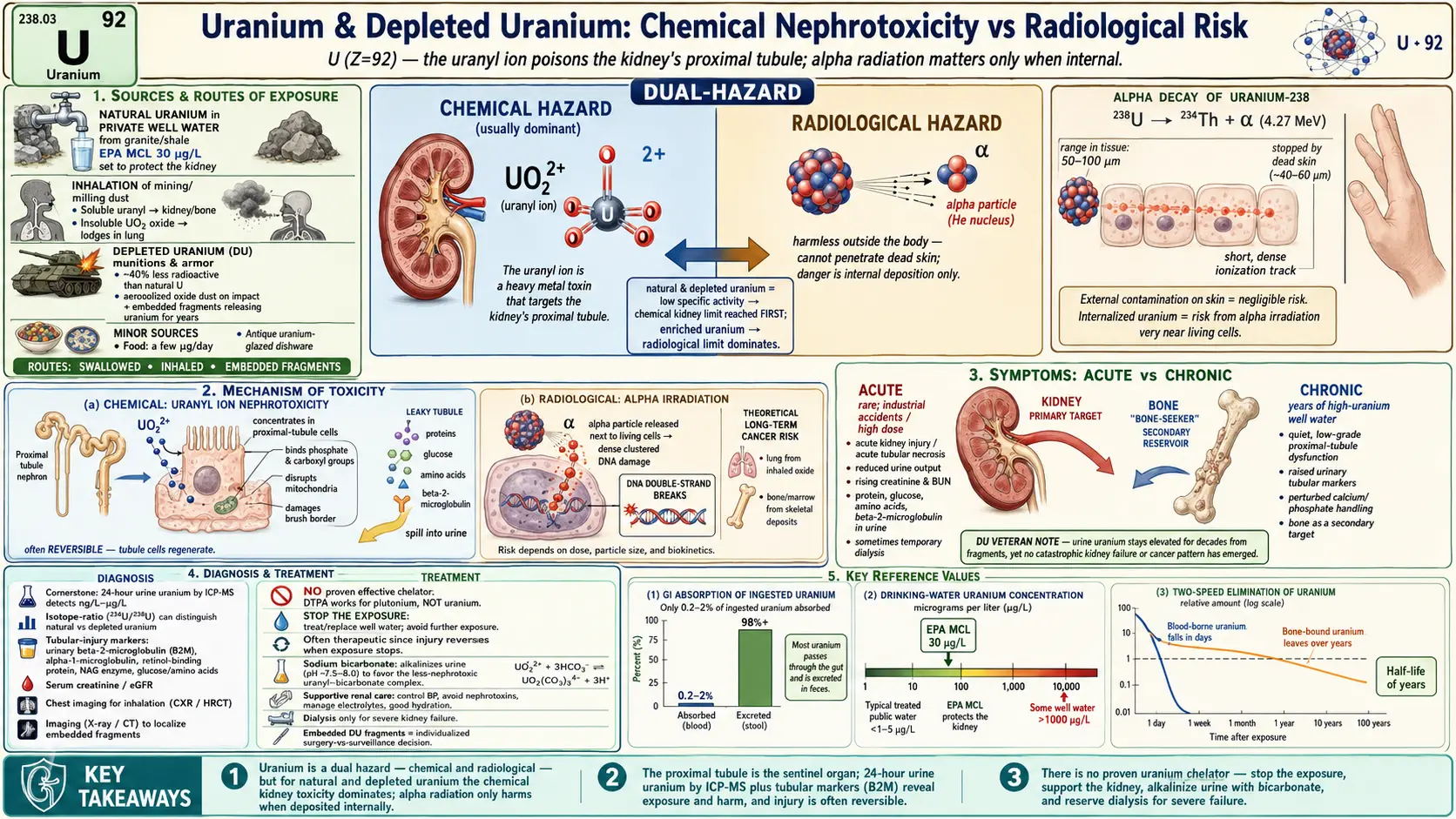
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Uranium is a naturally occurring heavy metal, the heaviest element found in any appreciable quantity in nature (atomic number 92). It carries a property almost no other environmental toxin shares: it is dangerous in two completely different ways at once. Like lead, cadmium, and mercury, uranium is a toxic metal whose ions can poison living tissue through ordinary chemistry. But uranium is also radioactive, slowly decaying and emitting radiation that damages cells through an entirely separate physical mechanism. Understanding uranium toxicity means keeping both hazards in view at once, and knowing which one matters most in a given situation.
The dual-hazard principle
This is the single most important idea on this page. Uranium poses a chemical hazard (it is a toxic metal) and a radiological hazard (it is radioactive), and which one dominates depends entirely on the type of uranium and how a person is exposed. For natural uranium and depleted uranium (DU) — the forms ordinary people are most likely to encounter — the chemical toxicity is by far the greater concern. These forms have very low specific activity, meaning they decay so slowly that the radiation dose they deliver is modest, while the heavy-metal chemistry of the uranyl ion readily injures the kidney. For enriched uranium (used in reactors and weapons) and for internal contamination with the more radioactive isotopes, the radiological risk rises and can become the leading concern. Brugge and colleagues, in a widely cited review, laid out exactly these two exposure-and-effect pathways and concluded that for natural uranium the chemical kidney toxicity is the limiting factor for most realistic exposures.
Uranium versus other toxic metals
If you have read the companion pages on lead or cadmium, the chemical side of uranium will feel familiar. Like cadmium, uranium concentrates in and damages the proximal tubule of the kidney, the segment that reabsorbs nutrients and proteins from filtered fluid. The classic signature of injury — small proteins spilling into the urine, amino acids leaking out, and a measurable dip in filtering ability — is the same family of "tubular" damage seen with other heavy metals. What sets uranium apart is the radiation, which adds questions about cancer risk that simply do not arise with lead or cadmium. A recurring theme below is honesty: uranium is a genuine toxin that deserves respect, but as the depleted-uranium veteran evidence shows, the most alarming predictions have so far not been borne out, and the science is presented here without either dismissing real risk or overstating it.
2. Sources & Routes of Exposure
Uranium is everywhere in trace amounts — in soil, rock, seawater, and even in the food we eat — so everyone carries a tiny, harmless background body burden. Toxicity becomes a concern only when exposure is concentrated by geology, industry, or warfare. The route of exposure (drinking, breathing, or a wound) strongly shapes which organ is hit and which hazard, chemical or radiological, predominates.
Natural uranium in drinking water
For the general public, the most common meaningful exposure is uranium dissolved in groundwater. Where bedrock is rich in uranium-bearing minerals — granites and certain shales — private wells can draw strikingly high concentrations. Studies of well-water users in Finland, where granite is widespread, found water uranium ranging from undetectable to well over a thousand micrograms per liter (µg/L) in extreme cases. The U.S. EPA sets a Maximum Contaminant Level (MCL) for uranium in public drinking water at 30 µg/L, a limit set specifically to protect the kidney from chemical injury rather than for radiation reasons. Private wells are unregulated, so households on well water in uranium-rich regions can unknowingly consume far more than the public-system limit allows.
Mining, milling, and occupational exposure
Workers in uranium mining, ore milling, fuel fabrication, and certain defense facilities can encounter much higher and more varied exposures than the public. The chief occupational route is inhalation of uranium-bearing dusts and aerosols, and chemical form matters enormously: soluble compounds (uranyl salts) are absorbed into the blood and travel to kidney and bone, while insoluble oxides (uranium dioxide) lodge in the lung and clear very slowly, shifting concern toward long-term radiological dose to lung tissue. Miners also face a separate hazard from radon, a radioactive decay-product gas — but radon lung-cancer risk is a distinct topic from uranium-metal toxicity itself.
Depleted uranium in munitions and armor
Depleted uranium (DU) is what is left over after natural uranium has had most of its more radioactive isotope removed during enrichment for reactor or weapons fuel. The leftover metal is roughly 40 percent less radioactive than natural uranium, yet it is extraordinarily dense and hard, which made it attractive for armor plating and armor-piercing munitions. When a DU round strikes a hard target it can ignite and aerosolize, scattering fine uranium-oxide dust. The exposures of concern from DU are therefore (1) inhalation of that aerosol by soldiers or bystanders near impacts, and (2) embedded fragments — shrapnel retained in the body of wounded personnel, which slowly dissolves and releases uranium into the bloodstream for years.
Other and minor sources
Food contributes a small daily intake of uranium, generally a few micrograms, mostly from root vegetables and grains grown in uranium-bearing soil; phosphate fertilizers add natural uranium to some produce and runoff. Historic uses — uranium-colored "Vaseline glass," orange-red ceramic glazes such as old Fiestaware, and antique dental porcelains — are now mostly curiosities and are best not used for food. None of these everyday sources approaches the exposures from high-uranium well water, occupational dust, or embedded DU fragments, which are the situations that actually drive clinical toxicity.
3. Toxicokinetics
Toxicokinetics is the story of what the body does to a toxin: how much gets in, where it goes, where it lingers, and how it leaves. Uranium's behavior is shaped by its chemistry — in body fluids it exists largely as the uranyl ion (UO22+), a charged species that binds avidly to bicarbonate, citrate, and proteins, and these complexes determine its fate.
Absorption depends on the route
Swallowed uranium is poorly absorbed. The gut takes up only a small fraction of ingested uranium — typically 0.2 to 2 percent, with soluble compounds at the higher end and insoluble oxides at the lower end — while the remaining 98-plus percent is excreted in stool without ever entering the body. This low absorption is why drinking-water uranium, even when elevated, tends to produce subclinical kidney effects rather than dramatic acute poisoning. Inhaled uranium is different: soluble aerosols enter the blood within days, whereas insoluble oxide particles can be retained in the lungs and lymph nodes for months to years, releasing uranium gradually. Intact skin is a poor route, but uranium enters directly through wounds and embedded fragments.
Distribution: kidney and bone
Once uranium reaches the blood it distributes to two principal sites. Most is cleared by the kidneys over the following days, but a meaningful share is deposited in the kidney itself, concentrating in the proximal tubule cells — the source of its chemical toxicity. The rest is taken up by bone, where the uranyl ion substitutes for calcium in the mineral matrix. Uranium is therefore, like lead, a "bone-seeker": skeletal uranium can persist for years as a slow internal reservoir. Kurttio and colleagues found that natural uranium in drinking water can affect bone as well as kidney, reinforcing that the skeleton is a genuine target organ, not merely a passive store.
Elimination and half-life
Uranium that enters the blood is excreted chiefly in the urine — which is precisely why a urine sample is the cornerstone of testing. Clearance is not a single number: blood-borne uranium falls quickly over days, while the fraction locked into bone leaves with a half-life of years. This two-speed elimination explains a key observation: in veterans carrying embedded DU fragments, uranium stays detectable in urine for decades after injury, because the fragments continuously top up the body burden faster than the skeleton and kidneys clear it. After a one-time soluble exposure with no retained source, by contrast, urine uranium falls back toward baseline within weeks.
4. Mechanism of Toxicity
Uranium's two hazards arise from two unrelated mechanisms. The chemical mechanism is a matter of metal-ion chemistry attacking cell machinery; the radiological mechanism is a matter of energetic particles breaking molecular bonds. Both can, in principle, occur in the same tissue, but they operate on different timescales and through different biology.
Chemical mechanism: the proximal tubule under attack
The chemical target is the kidney's proximal tubule, the segment that reabsorbs glucose, amino acids, and small proteins after blood is filtered in the glomerulus. The uranyl ion is delivered to and concentrated by exactly these cells. There, like other heavy metals, it binds phosphate and carboxyl groups on proteins and membranes, disrupts the energy-producing mitochondria, impairs the pumps and transporters that drive reabsorption, and damages the brush-border surface. Classic experimental work by McDonald-Taylor and colleagues, dosing rabbits with uranyl nitrate, documented and quantified precisely these proximal-tubule lesions. The result is a leaky tubule: proteins and amino acids that should have been reclaimed spill into the urine, and overall filtering performance can dip. Crucially, because tubule cells regenerate, this injury is often reversible if exposure stops before damage becomes severe.
Radiological mechanism: alpha particles
Uranium decays by emitting alpha particles — heavy, slow, doubly charged particles with a paradoxical safety profile. Outside the body alpha radiation is almost harmless: it cannot penetrate even the dead outer layer of skin, so external uranium does not irradiate living tissue. The entire radiological concern is internal deposition. If uranium is inhaled and lodges in the lung, or settles into bone, the alpha particles are then released right next to living cells, depositing their energy in a tiny volume and causing dense, clustered DNA damage. Over the long term this underlies a theoretical increase in cancer risk (lung from inhaled insoluble oxides; bone and adjacent marrow from skeletal deposits). For natural and depleted uranium the slow decay rate keeps this dose low, which is why chemistry, not radiation, usually wins the race to cause harm.
Which mechanism dominates, and why it matters
O'Connell and colleagues directly compared chemical and radiological toxicity limits across different uranium enrichments and showed how the balance tips: at low enrichment (natural and depleted uranium) the chemical kidney limit is reached first, so kidney protection sets the safety threshold; as enrichment and specific activity climb, the radiological limit becomes the constraint. Kathren's review of acute chemical toxicity similarly emphasizes that in a sudden high-dose human exposure it is the kidney, poisoned chemically, that fails first — not any acute radiation effect. This is not an academic distinction: it tells clinicians to watch the kidney, and it tells regulators that for the uranium most people meet, a chemical heavy-metal framework is the right one.
5. Symptoms & Health Effects
Uranium's symptoms follow directly from its mechanisms, and they differ sharply depending on whether exposure is a sudden large dose (acute) or a low dose sustained over years (chronic). In both, the kidney is the sentinel organ, and many of the early effects are silent — visible only in laboratory tests, not in how a person feels.
Acute toxicity
Acute uranium poisoning is rare and essentially confined to industrial accidents, laboratory mishaps, or deliberate high-dose exposures. When a large amount of soluble uranium enters the body quickly, the dominant effect is acute kidney injury from chemical poisoning of the proximal tubule. Features can include:
- Reduced or changed urine output and a rise in blood markers of kidney function (creatinine, blood urea nitrogen).
- Protein, glucose, and amino acids appearing in the urine as the damaged tubule fails to reabsorb them.
- Tubular markers spilling into urine — small proteins such as beta-2-microglobulin that healthy tubules normally reclaim.
- In severe cases, the picture of acute tubular necrosis, which may require temporary dialysis support.
Kathren's analysis of human acute exposures underscores that it is this chemical renal failure — not radiation sickness — that defines and limits acute uranium toxicity. Encouragingly, even acute tubular injury frequently recovers once exposure ends and supportive care is provided.
Chronic toxicity
Chronic exposure — typically years of drinking high-uranium well water, or long occupational contact — produces a quieter, subclinical pattern. The hallmark is low-grade proximal-tubule dysfunction detectable on laboratory testing before any symptoms appear. Kurttio and colleagues, studying Finnish well-water users, found that higher uranium intake was associated with measurable signs of tubular effect — increased urinary excretion of certain markers and subtle changes in calcium and phosphate handling — even though the participants felt well and their overall filtration was largely preserved. Key points about chronic effects:
- Effects are usually mild and subclinical at typical environmental exposures: biochemical changes rather than overt kidney disease.
- The pattern is tubular (reabsorption failures: small proteins, glucose, amino acids in urine) rather than glomerular.
- Bone is a secondary target; uranium's calcium-mimicry may perturb bone mineral handling, as Kurttio's bone study suggested.
- Whether chronic environmental uranium causes progressive, clinically significant kidney disease in humans remains uncertain, with most studies showing reversible, low-level effects rather than relentless decline.
Radiological and cancer concerns
Because natural and depleted uranium are weak radiation sources, no clear cancer signal has been convincingly demonstrated in human populations exposed at typical levels. The theoretical risk — lung cancer from inhaled insoluble oxides, bone or marrow effects from skeletal deposits — is real in principle and rises with enrichment and internal dose, but for environmental and DU exposures it is small and hard to separate from background. The honest summary is that the chemical kidney effects are far better documented than any radiological disease outcome at these exposure levels.
The depleted-uranium veteran experience
Concern about DU surged after the 1991 Gulf War and later Balkans conflicts, with fears of widespread cancers, birth defects, and "Gulf War syndrome." The long-running U.S. Department of Veterans Affairs follow-up of DU-exposed veterans — many carrying embedded fragments — provides the best human data. Reporting at 25 years, McDiarmid and colleagues found that, despite urine uranium remaining elevated for decades in fragment-carriers, the cohort has generally not shown the dramatic kidney failure, cancers, or other catastrophic effects that were feared; subtle findings in some renal and other measures have been reported and are watched, but no clear pattern of serious disease has emerged. The responsible interpretation is balanced: this is reassuring evidence against the worst-case scenarios, it does not prove zero risk, uncertainty remains for inhalation exposures and longer timeframes, and continued surveillance is warranted. Avoiding both alarmism and dismissal is essential here.
6. Diagnosis & Laboratory Testing
Diagnosing uranium exposure rests on directly measuring uranium in the body and looking for the kidney's characteristic fingerprint of injury. Because uranium is excreted in urine, a urine sample is the central specimen, and modern instruments can detect it at exquisitely low levels.
The cornerstone: 24-hour urine uranium by ICP-MS
The reference test for uranium body burden is a 24-hour urine uranium measured by inductively coupled plasma mass spectrometry (ICP-MS). ICP-MS is sensitive enough to detect uranium in the nanograms-per-liter to micrograms-per-liter range, far below levels of concern, and it can be paired with isotope-ratio analysis to distinguish natural uranium from depleted uranium — forensically valuable, since the isotopic signature reveals whether a person's uranium came from munitions rather than the environment. A full 24-hour collection is preferred over a spot sample because it averages out the day's swings in urine concentration; when a complete collection is impractical, a spot urine uranium can be normalized to urinary creatinine, and McDiarmid and colleagues studied the utility of spot collections for monitoring DU-exposed veterans for exactly this reason. Results are typically expressed as micrograms per gram of creatinine (µg/g creatinine) for spot samples or micrograms per 24 hours (µg/24 h) for timed collections.
Tubular-injury markers
Measuring uranium tells you about exposure; measuring tubular markers tells you about harm. Because uranium injures the proximal tubule, the most informative tests look for small molecules that a healthy tubule reabsorbs but a damaged one lets slip into the urine:
- Urinary beta-2-microglobulin (B2M) — a small protein freely filtered by the glomerulus and normally almost entirely reabsorbed by the proximal tubule. Its appearance in urine is a sensitive sign of tubular dysfunction. (B2M is acid-labile, so samples should be collected with attention to urine pH.)
- Other low-molecular-weight proteins such as alpha-1-microglobulin and retinol-binding protein, used similarly as tubular markers.
- Urinary N-acetyl-beta-D-glucosaminidase (NAG), an enzyme released from injured tubule cells.
- Glucose and amino acids in the urine in the absence of high blood glucose, indicating failed proximal reabsorption.
Together these markers define the "tubular proteinuria" pattern that is the chemical signature of uranium and other heavy-metal nephrotoxicity. Standard tests of overall kidney function — serum creatinine, estimated glomerular filtration rate (eGFR), and routine urinalysis — round out the assessment and detect any reduction in filtering capacity.
Radiological assessment
When internal contamination with a significant radiological component is suspected (for example, after inhaling enriched-uranium aerosol), specialized radiobioassay and whole-body or organ counting can estimate the radiation dose. In vitro bioassay measures uranium and its decay products in urine and feces; in vivo counting uses external detectors (such as lung counters) to estimate the amount of uranium deposited in the body. These methods convert measured uranium into an estimated radiation dose, complementing the chemical-toxicity picture from urine uranium and tubular markers.
Imaging and history
A careful exposure history is indispensable: well-water source and region, occupation, and any history of combat injury or retained shrapnel. In suspected inhalation exposure, chest imaging (radiograph or CT) is used to evaluate the lungs. In wounded individuals, imaging can localize embedded metal fragments, which are radiographically dense; identifying and tracking these fragments is central to managing DU-injured patients, since the fragments are the ongoing internal source revealed by persistently elevated urine uranium.
7. Treatment & Management
Treatment of uranium exposure is, frankly, more limited than patients often expect. There is no quick antidote that pulls uranium cleanly out of the body. Management centers on stopping further exposure, supporting the kidney, and applying a few specific measures of modest and debated benefit.
Stop the exposure
The first and most effective step is to remove the source. For high-uranium well water, this means switching to an alternative supply or installing effective treatment (see Prevention). For occupational dust, it means correcting the workplace hazard and removing the worker from exposure. Because uranium's tubular injury is frequently reversible, simply ending intake often allows the kidney to recover on its own — making source removal not just preventive but genuinely therapeutic.
The chelation problem
For lead and some other heavy metals, chelating drugs that grab the metal and escort it out in urine are a mainstay. Uranium has no clearly proven, effective chelator, which is a key practical difference and a common point of confusion. In particular:
- DTPA (diethylenetriaminepentaacetic acid), the standard chelator for transuranic elements such as plutonium, is not very effective for uranium and is not a reliable treatment for it. Patients and even clinicians sometimes assume "radioactive metal, therefore DTPA," but uranium does not respond well to it.
- Sodium bicarbonate has been used historically not as a chelator but to alkalinize the urine. Raising urine pH favors formation of the relatively soluble, less nephrotoxic uranyl-bicarbonate complex, which may help the kidney handle and excrete uranium with less tubular damage. This is a supportive, mechanism-based measure rather than a proven cure, and it is used with care given the systemic effects of bicarbonate loading.
Supportive renal care
The backbone of treatment is good supportive care of the kidney: maintaining adequate hydration and urine flow, correcting fluid and electrolyte disturbances, avoiding additional nephrotoxic drugs, and monitoring kidney function and tubular markers over time. In severe acute poisoning with kidney failure, dialysis may be needed temporarily to support the patient while the tubule regenerates; dialysis treats the consequence (kidney failure) rather than efficiently removing uranium itself. Because recovery of tubular function is common once exposure stops, the prognosis for the kidney is often favorable with attentive supportive management.
Embedded fragments: a genuine dilemma
For veterans and others with embedded DU shrapnel, management is contested. Each retained fragment is a slow, continuous internal source, which is why urine uranium stays elevated for years. In principle surgical removal would cut off that source — but extracting fragments carries its own risks (damage to nerves, vessels, and tissue), and the demonstrated harm from the fragments has so far been limited. The result is an individualized risk-benefit judgment: easily accessible fragments may be removed, while deeply embedded ones are frequently left in place under long-term surveillance. The VA cohort program, described by Squibb and McDiarmid and colleagues, embodies this — systematic monitoring of urine uranium, kidney function, and other measures rather than reflexive surgery.
What patients should take away
There is no magic uranium antidote; the most powerful interventions are stopping exposure and protecting the kidney, and chelation is not the answer it is for lead. Anyone with a specific concern — a high-uranium well, an occupational history, or retained fragments — should be evaluated by a clinician experienced in toxicology or occupational medicine, with urine uranium and tubular-marker testing to guide decisions. Information here is educational and not a substitute for individual medical advice.
8. Prevention & Risk Reduction
Because uranium absorption is low and its early effects are reversible, prevention is highly effective — and for the most common exposure, drinking water, it is largely within an individual household's control.
Test and treat your water
If you draw water from a private well, especially in a region known for granite or uranium-bearing rock, test it for uranium. Public water systems must meet the EPA's 30 µg/L MCL, but private wells are unregulated and are the most likely place to find dangerous levels. If testing reveals elevated uranium, several treatment technologies reduce it effectively:
- Reverse osmosis (RO) point-of-use systems, which remove the large majority of dissolved uranium and are a common household choice for drinking and cooking water.
- Ion exchange (anion-exchange resins), effective for whole-house uranium removal.
- Activated alumina and certain other adsorptive media.
Switching to bottled or an alternative tested supply for drinking and cooking is a simple interim measure while treatment is arranged. Because the gut absorbs so little uranium, reducing the concentration in drinking water translates fairly directly into a lower body burden over time.
Occupational protection
In mining, milling, fuel fabrication, and defense work, prevention follows standard industrial-hygiene principles aimed primarily at preventing inhalation of uranium dust and aerosols: engineering controls and ventilation to suppress airborne dust, respiratory protection where needed, contamination control and good housekeeping, and biological monitoring (periodic urine uranium and kidney-function testing) to catch exposure early. Special attention goes to the chemical form, since soluble compounds threaten the kidney while insoluble oxides threaten the lung. Radon control is a related but separate program in underground mines.
Battlefield and post-conflict settings
Reducing DU exposure focuses on limiting contact with struck vehicles and impact sites, where uranium-oxide dust and fragments concentrate, and on prompt medical evaluation and urine uranium testing for personnel with possible inhalation or embedded-fragment exposure. The World Health Organization and International Atomic Energy Agency have issued guidance on assessing DU contamination in former conflict zones, including environmental sampling and public-health communication. Clear, honest risk communication — neither minimizing nor exaggerating — is itself a preventive tool, since unfounded panic carries its own harms.
Everyday common-sense measures
For the general public outside these special situations, no elaborate precautions are warranted. Do not use uranium-glazed antique dishware for serving food or drink, and rely on a varied diet and a tested, safe water supply, which keep dietary uranium at the harmless background level everyone carries. The reassuring bottom line: for nearly everyone uranium is a non-issue, and where it is an issue — chiefly high-uranium well water — straightforward testing and treatment resolve it.
9. Related Topics
- Toxic Minerals (overview hub) — the full set of toxic metals and metalloids covered on this site.
- Heavy Metals — shared chemistry and the common proximal-tubule injury pattern across toxic metals.
- Cadmium — another metal whose hallmark is reversible-to-chronic proximal-tubule damage and tubular proteinuria.
- Lead — a fellow "bone-seeker" with long skeletal retention, useful contrast to uranium's bone handling.
- Mercury — heavy-metal nephrotoxin with its own tubular-injury signature.
- Arsenic — drinking-water contaminant of geological origin, a parallel to uranium in wells.
- Phosphorus — uranyl ions bind phosphate groups; phosphate handling is perturbed in uranium tubular injury.
- Calcium — uranium substitutes for calcium in bone, the basis of its "bone-seeker" behavior.
- Kidney Disease — the organ system at the center of uranium's chemical toxicity.
- Lab Tests — background on the urine and blood testing used to detect exposure and kidney injury.
- All Minerals — the broader minerals library, including essential minerals and their toxic counterparts.
10. Key Research Papers
- Brugge D, Buchner V. Exposure pathways and health effects associated with chemical and radiological toxicity of natural uranium: a review. Reviews on Environmental Health. 2005;20(3):177-193.
- Kathren RL, Burklin RK. Acute chemical toxicity of uranium. Health Physics. 2008;94(2):170-179.
- O'Connell M, Strom DJ, Schwartz DR. Evaluation of radiological versus chemical toxicity limits for varying enrichments of uranium for Department of Energy facilities. Health Physics. 2010;98(2 Suppl):S17-S21.
- Kurttio P, Auvinen A, Salonen L, et al. Renal effects of uranium in drinking water. Environmental Health Perspectives. 2002;110(4):337-342.
- Kurttio P, Harmoinen A, Saha H, et al. Kidney toxicity of ingested uranium from drinking water. American Journal of Kidney Diseases. 2006;47(6):972-982.
- Kurttio P, Komulainen H, Leino A, et al. Bone as a possible target of chemical toxicity of natural uranium in drinking water. Environmental Health Perspectives. 2005;113(1):68-72.
- McDonald-Taylor CK, Singh A, Gilman A. Uranyl nitrate-induced proximal tubule alterations in rabbits: a quantitative analysis. Toxicologic Pathology. 1997;25(4):381-389.
- McDiarmid MA, Gaitens JM, Hines S, et al. The U.S. Department of Veterans' Affairs depleted uranium exposed cohort at 25 years: longitudinal surveillance results. Environmental Research. 2017;152:175-184.
- Squibb KS, Gaitens JM, Engelhardt S, et al. Surveillance for long-term health effects associated with depleted uranium exposure and retained embedded fragments in U.S. veterans. Journal of Occupational & Environmental Medicine. 2012;54(6):724-732.
- Gwiazda RH, Squibb K, McDiarmid M, Smith D. Detection of depleted uranium in urine of veterans from the 1991 Gulf War. Health Physics. 2004;86(1):12-18.
- McDiarmid MA. Depleted uranium and public health. BMJ. 2001;322(7279):123-124.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Uranium. U.S. Department of Health and Human Services. Available at: ATSDR ToxProfiles — Uranium.
- World Health Organization. Uranium in Drinking-water: Background Document for Development of WHO Guidelines for Drinking-water Quality. Available at: WHO — Uranium in drinking-water.
- U.S. Environmental Protection Agency. Radionuclides in Drinking Water and the Uranium Maximum Contaminant Level (30 µg/L). Available at: US EPA — Radionuclides Rule.
Connections
- All Toxic Minerals
- Heavy Metals
- Cadmium
- Lead
- Mercury
- Arsenic
- Phosphorus
- Calcium
- Kidney Disease
- Lab Tests
- All Minerals