Gadolinium Toxicity: MRI Contrast Retention, NSF, and Deposition Disease
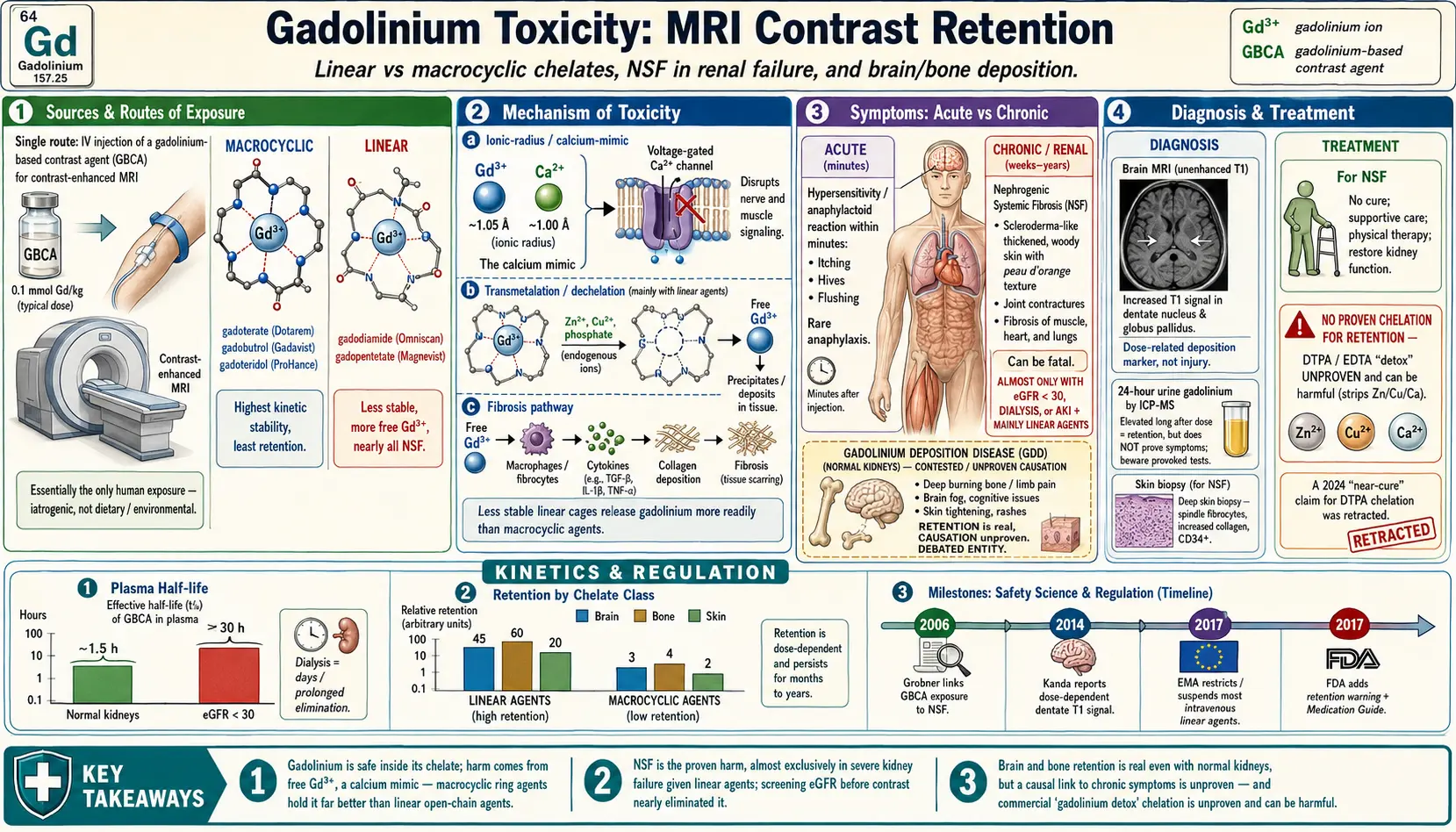
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Gadolinium is a soft, silvery rare-earth metal (a lanthanide, element 64) that almost nobody would ever encounter were it not for one extraordinarily useful property: the free gadolinium ion, written Gd3+, has seven unpaired electrons, which makes it intensely paramagnetic. In a magnetic-resonance-imaging (MRI) scanner, that paramagnetism shortens the relaxation time of nearby water protons and lights up tissues on the image. This is why gadolinium-based contrast agents (GBCAs) are injected into a vein before a "contrast-enhanced" MRI — to make tumors, inflamed tissue, blood vessels, and disrupted areas of the brain stand out. Tens of millions of these injections are given worldwide every year, and for the overwhelming majority of patients an MRI with contrast is a safe, painless test that answers a question no other scan could.
The catch is that the free Gd3+ ion itself is toxic. Its ionic radius is almost identical to that of calcium (Ca2+), so the body's calcium-handling machinery — including voltage-gated calcium channels in nerve and muscle — cannot tell the two apart. Free gadolinium blocks those channels and interferes with any calcium-dependent process it reaches. Nature never intended a +3 lanthanide to circulate in blood, and the body has no transport protein, no storage organ, and no biological use for it. For that reason gadolinium is never given as a bare ion. It is wrapped inside an organic cage called a chelate (from the Greek for "claw"), which grips the metal so tightly that the complex behaves like an inert, water-soluble molecule that the kidneys can flush out within hours.
Almost the entire safety story of gadolinium comes down to a single question: how reliably does the chelate keep its grip? Two things can let gadolinium escape its cage. First, the cage can simply not be very strong — the older "linear" agents have an open-chain structure that releases more free metal than the newer "macrocyclic" agents, whose ring locks the ion in like a closed fist. Second, if the chelate stays in the body far longer than designed — as happens when the kidneys are failing — even a slow leak has time to add up. These two factors define the two distinct gadolinium harms this page covers: nephrogenic systemic fibrosis (NSF), a rare but devastating disease seen almost only in people with severe kidney failure, and gadolinium retention (sometimes described by patients and some clinicians as gadolinium deposition disease, GDD), in which traces of the metal linger in the brain, bone, and skin even in people whose kidneys work normally.
What this page is and is not saying
This is not a page telling people to refuse MRI contrast. Contrast-enhanced MRI saves lives — it finds strokes, cancers, and infections that change treatment. The goal here is to lay out honestly what is well established (NSF is real and gadolinium causes it; gadolinium is measurably retained in the body), what is uncertain (whether that retained gadolinium causes chronic symptoms in people with healthy kidneys), and what is simply unproven or potentially harmful (commercial "gadolinium detox" chelation). Patient-reported symptoms after gadolinium are taken seriously here, not dismissed; at the same time, the science is presented as it actually stands, without overstating a causal link that the published evidence has not yet confirmed.
2. Sources & Routes of Exposure
For practical purposes, there is essentially one route of human exposure to gadolinium: an intravenous injection of a contrast agent for an imaging study. Gadolinium is not a dietary mineral, it is not in food or water at any meaningful level, it is not absorbed through intact skin, and it is not an occupational or environmental poison the way lead or mercury are. People are exposed because a radiologist gave them a deliberate, measured dose. That makes gadolinium toxicity almost entirely iatrogenic (caused by medical care) and therefore, in principle, controllable by how that care is delivered.
The contrast agents themselves
GBCAs are usually injected as a weight-based dose — a common standard for many agents is 0.1 millimole of gadolinium per kilogram of body weight, which for an average adult is on the order of a few grams of the chelated compound. They are given for contrast-enhanced MRI of the brain, spine, breast, heart, liver, and blood vessels (MR angiography), among many others. A closely related use, MR arthrography, injects a very dilute gadolinium solution directly into a joint to outline cartilage; another related route is intrathecal (into the spinal fluid) use, which is generally off-label and used cautiously.
The single most important distinction: linear vs. macrocyclic
Every GBCA falls into one of two structural classes, and this distinction predicts how much free gadolinium it sheds and therefore how much risk it carries.
- Macrocyclic agents — gadoterate (Dotarem/Clariscan), gadobutrol (Gadavist/Gadovist), and gadoteridol (ProHance). The chelate is a pre-formed rigid ring that surrounds the metal on all sides. These have the highest kinetic stability: they release very little free gadolinium and are associated with the least tissue retention.
- Linear agents — gadodiamide (Omniscan), gadopentetate dimeglumine (Magnevist), gadoversetamide (OptiMARK), and others. The chelate is an open chain wrapped around the ion. These are less stable, release more free gadolinium through a process called transmetalation (where the body's own ions, such as zinc, displace gadolinium from the cage), and are linked to more retention and to nearly all cases of NSF.
Because of this, regulators acted on the class, not just on individual products. In 2017 the European Medicines Agency suspended or restricted several of the highest-risk linear agents for general body imaging, keeping a few linear agents only for specific niche uses (such as liver imaging) where they offer a unique benefit. The U.S. Food and Drug Administration did not pull linear agents from the market but added warnings about retention and required a patient-facing Medication Guide. The simplest way to read this: when a GBCA is needed and there is a choice, a macrocyclic agent is the lower-retention option.
3. Toxicokinetics
Toxicokinetics is the study of what the body does to a substance — how it is distributed, where it goes, and how it is removed. For gadolinium chelates the answer is normally simple and reassuring, and it explains exactly why kidney function is the master switch for risk.
Distribution and clearance in healthy kidneys
After injection, a standard GBCA stays almost entirely in the extracellular fluid — the watery space inside blood vessels and between cells. It does not enter cells in any large amount and does not cross an intact blood–brain barrier well, which is precisely why it highlights places where that barrier is broken (tumors, inflammation). The intact chelate is then filtered by the kidneys and excreted essentially unchanged in the urine. In a person with normal renal function the plasma half-life is roughly 1.5 hours, and the great majority of the injected dose is gone in the urine within about a day. In a healthy person, the chelate behaves like a transient dye that comes and goes.
What changes in kidney failure
Now remove the kidneys from the equation. In a patient with an estimated glomerular filtration rate (eGFR) below 30 milliliters per minute, and especially in someone on dialysis, the clearance pathway is crippled. The half-life no longer measures in hours but can stretch to 30 hours or more, and in dialysis-dependent patients the chelate can circulate for days. That prolonged residence time is the problem: the longer a less-stable chelate sits in the body, the more opportunities it has to slowly release free Gd3+ through transmetalation. The released free gadolinium then leaves the bloodstream and binds to tissues — this is the chain of events that produces NSF. Kidney function does not change the toxicity of free gadolinium; it changes how much chelate hangs around long enough to leak.
Retention even with normal kidneys
For decades the assumption was that if the kidneys clear the agent within a day, the gadolinium is simply gone. That assumption turned out to be incomplete. Sensitive measurements — autopsy tissue analysis and signal changes on later MRI scans — show that a small fraction of administered gadolinium is retained for months to years in specific tissues even in people with entirely normal kidneys, particularly the brain (notably the dentate nucleus and globus pallidus), bone (which behaves as a long-term gadolinium reservoir), and skin. The amounts are tiny compared with the injected dose, and retention is greater with linear agents than with macrocyclic ones. Crucially, "retained" does not automatically mean "free toxic ion": some of the retained gadolinium is still chelated, and some is dechelated and bound to tissue macromolecules. Sorting out which form predominates — and whether the dechelated form causes any harm in people with healthy kidneys — is exactly where the open scientific questions lie.
4. Mechanism of Toxicity
To understand why a metal that is so useful inside a cage can be dangerous outside it, it helps to look at the chemistry of the free Gd3+ ion and at the single trick the entire technology relies on.
The calcium mimic
The ionic radius of Gd3+ (about 1.05 angstroms in a typical coordination) is strikingly close to that of Ca2+ (about 1.00 angstroms). Calcium is one of the body's most important signaling ions: it triggers muscle contraction, nerve firing, blood clotting, and countless enzyme reactions, and cells spend enormous energy keeping calcium concentrations precisely controlled. Because gadolinium is almost the same size and also carries positive charge, it can slip into calcium's seat. In the laboratory, free Gd3+ is a potent blocker of voltage-gated calcium channels and can interfere with calcium-dependent enzymes and with the function of large calcium-binding proteins. If meaningful amounts of free gadolinium ever circulated, the result would be disruption of nerve and muscle signaling. This is the fundamental reason gadolinium must never be administered as a free ion — and the reason the chelate is not a luxury but the entire safety basis of the drug.
Thermodynamic vs. kinetic stability — and transmetalation
Chelate strength is described two ways, and the difference matters. Thermodynamic stability asks how tightly the cage holds gadolinium at equilibrium; kinetic stability asks how fast the gadolinium can actually escape under real biological conditions. The second is what counts in a living body, because blood is full of competing ions — zinc, copper, calcium — and competing molecules such as phosphate that want to grab gadolinium. When an endogenous ion displaces gadolinium from its chelate, that swap is called transmetalation. The freed Gd3+ then tends to precipitate with phosphate or bind to tissue, while the displacing metal walks off with the now-empty cage. Macrocyclic ring chelates resist this swap far better than open-chain linear ones — the ring has to break in several places at once before the metal can leave — which is the molecular reason macrocyclic agents shed less free gadolinium and are the safer class.
From free ion to fibrosis
In NSF, the proposed sequence runs: a less-stable chelate persists for days because failing kidneys cannot clear it, transmetalation slowly liberates free Gd3+, the freed gadolinium deposits in skin and other tissues, and its presence appears to recruit and activate circulating fibrocytes — bone-marrow-derived cells that lay down collagen. The result is widespread fibrosis: skin and connective tissue thicken and harden as if scar tissue were forming everywhere at once. For brain retention in people with normal kidneys, the mechanistic picture is much less certain; gadolinium clearly accumulates in specific deep-brain nuclei, but whether it does so as harmful free ion or as inert residue, and whether it injures those neurons at all, has not been established. The honest mechanistic statement is that the path from free gadolinium to fibrosis in kidney failure is well supported, whereas the path from low-level brain retention to chronic symptoms in healthy kidneys is hypothesized but not proven.
5. Symptoms & Health Effects
Gadolinium-associated health effects fall into three quite different categories, and conflating them causes a great deal of confusion. They are: immediate allergic-type reactions to the injection, the rare fibrosing disease NSF, and the contested cluster of chronic symptoms attributed to gadolinium retention. Each has a different cause, a different population at risk, and a very different level of scientific certainty.
Acute hypersensitivity reactions
Like any injected drug, a GBCA can trigger an allergic-type (anaphylactoid) reaction that has nothing to do with retention. These are uncommon, usually mild — itching, hives, nausea — and occasionally severe with breathing difficulty or a drop in blood pressure that requires emergency treatment. They begin within minutes of the injection and are managed exactly like other contrast reactions. Importantly, this category is acute and immediate; it is unrelated to the long-term deposition questions and should not be confused with them.
Nephrogenic systemic fibrosis (NSF) — the best-established harm
NSF is the one gadolinium harm that is unambiguously proven, and it is serious. It is a scleroderma-like fibrosing disorder that develops over days to weeks after gadolinium exposure in a vulnerable patient. The hallmark is the skin: it becomes thickened, hardened, tight, and woody, often with a peau-d'orange (orange-peel) texture and brawny darkening, typically beginning on the lower legs and forearms and spreading. As the fibrosis progresses, the skin can bind down across joints, producing painful joint contractures that immobilize the limbs and can leave patients wheelchair-bound. The process is not limited to skin — fibrosis can involve muscle, the diaphragm, the heart, lungs, and other internal organs, and in its most aggressive form NSF has been fatal.
What makes NSF tractable is that its risk factors are clear. It has occurred almost exclusively in patients with severe renal impairment — advanced chronic kidney disease (eGFR below 30), patients on dialysis, and those with acute kidney injury — and overwhelmingly after exposure to the less-stable linear agents, with gadodiamide implicated most often. People with normal kidney function essentially do not get NSF. Because the cause and the at-risk group are both well defined, the disease has become very rare since hospitals began screening kidney function before contrast MRI and avoiding high-risk linear agents in renal failure.
Gadolinium retention and "gadolinium deposition disease" (GDD)
This is the category that generates the most patient concern and the most scientific debate, and it deserves to be described carefully and respectfully. A number of patients with normal kidney function have reported the onset of a chronic symptom cluster in the hours to weeks after a gadolinium-enhanced MRI. The reported features, as described in the case literature, commonly include:
- persistent pain — often deep, burning, or "boring" pain in the arms, legs, joints, and bones, sometimes described as among the most distressing features;
- cognitive symptoms — "brain fog," difficulty concentrating, and mental cloudiness;
- skin and subcutaneous changes — thickening, tightening, discoloration, or a tethered/"hardened" feeling of the skin (distinct from full NSF and occurring with normal kidneys);
- headache, and a sensation of "skin burning" or other peripheral discomfort;
- a reported tendency for symptoms to begin or flare soon after the contrast injection.
Two facts must be held together honestly here. First, brain retention is radiologically and pathologically real: later MRI scans can show increased T1 signal in the dentate nucleus and globus pallidus, and autopsy studies have measured gadolinium in brain tissue from people who had normal kidneys and several prior contrast scans. Second, a causal link between that retained gadolinium and the chronic symptoms has not been established. Whether GDD is a distinct gadolinium-caused illness, or whether the measured retention is an incidental marker while the symptoms have another explanation, remains genuinely unresolved and is the subject of active research and regulatory attention. Regulators (the FDA and EMA) acknowledge that retention occurs while stating that no harmful effect has been proven in patients with normal kidney function — and the FDA nonetheless requires a patient Medication Guide so that people can make an informed choice. Taking patient-reported symptoms seriously and acknowledging the limits of current causal evidence are not contradictory; both are part of an honest account.
6. Diagnosis & Laboratory Testing
There is no single blood test that "diagnoses gadolinium toxicity," and anyone selling one as a definitive answer is overstating what the science supports. Instead, evaluation combines the clinical picture, the imaging history, and a few specific tests — each interpreted with an understanding of what it can and cannot prove.
24-hour urine gadolinium
The most commonly discussed test is a 24-hour urine collection measured for gadolinium, reported in micrograms of gadolinium per 24 hours or normalized to creatinine (micrograms per gram of creatinine), usually by a technique called inductively coupled plasma mass spectrometry (ICP-MS), which can detect the metal at trace levels. The logic is straightforward: immediately after an MRI, everyone's urine gadolinium is high because the kidneys are excreting the dose, so a test in the first day or two means nothing. But if urine gadolinium remains elevated weeks, months, or years after the last injection — long after a healthy body should have cleared it — that points to ongoing release from a tissue reservoir such as bone, i.e. retention. The important caveat is interpretive: an elevated long-after-dose urine gadolinium confirms that gadolinium is still in the body, but it does not, by itself, prove that the gadolinium is causing a patient's symptoms. Reference ranges and "provoked" testing (giving a chelator first to mobilize metal and inflate the result) are not standardized, and provoked testing in particular can be misleading.
Skin biopsy for NSF
When NSF is suspected — that is, in a patient with kidney disease who develops thickening, hardening skin after gadolinium — the diagnostic test is a deep skin (and sometimes muscle) biopsy. Under the microscope, NSF shows a characteristic proliferation of spindle-shaped fibrocytes and thickened collagen bundles extending into the deep dermis and subcutaneous tissue, often with increased CD34-positive cells, and specialized elemental analysis can sometimes detect gadolinium within the affected tissue. The biopsy, read together with the clinical history of renal failure and prior gadolinium exposure, is what distinguishes NSF from scleroderma and other fibrosing skin diseases that can look similar.
MRI signal as evidence of brain retention
Retention in the brain can be inferred non-invasively from the MRI images themselves. On unenhanced T1-weighted scans, patients who have received multiple doses — especially of linear agents — can show increased (brighter) signal in the dentate nucleus of the cerebellum and the globus pallidus. This finding is a marker that gadolinium has accumulated in those deep nuclei; it is well documented and dose-related. As with the urine test, however, the signal change is evidence of deposition, not of injury or symptoms — many people with visible dentate/pallidal signal have no neurological complaints.
Putting the tests in context
The practical takeaway is that these tests answer the question "is gadolinium still present?" far better than they answer "is gadolinium making this person sick?" A careful evaluation also looks for and treats other explanations for the patient's symptoms, because attributing everything to gadolinium without ruling out alternatives can leave a treatable condition undiagnosed. Honest testing means honest interpretation: confirming retention is achievable; proving causation in an individual is not yet possible with current tools.
7. Treatment & Management
Treatment differs completely between the two main gadolinium conditions, and one widely promoted "treatment" deserves a direct warning.
Managing NSF
There is no reliably effective drug treatment that reverses NSF. Once the fibrosis is established, care is largely supportive: physical therapy to fight joint contractures and preserve mobility, pain control, and skin care. Various agents and procedures — including extracorporeal photopheresis, sodium thiosulfate, and others — have been tried with inconsistent results, and none is a dependable cure. The one intervention that genuinely matters is restoring kidney function: in patients whose acute kidney injury recovers, or who receive a successful kidney transplant, NSF has sometimes stabilized or partially improved, presumably because functioning kidneys finally clear the residual gadolinium and stop new deposition. This underscores that for NSF, prevention is overwhelmingly more powerful than any treatment.
"Detox" chelation for retention — unproven and potentially harmful
For gadolinium retention in people with normal kidneys, there is no proven therapy that removes deposited gadolinium and improves symptoms. This is the point at which patients are most vulnerable to harm from the marketplace. Commercial "gadolinium detox" programs promote chelation — most often with the agent DTPA, sometimes EDTA — given by IV over repeated, expensive sessions, frequently paired with "provoked" urine tests designed to produce alarming-looking numbers that justify more sessions. Several cautions are warranted, and they should be stated plainly:
- It is unproven. No high-quality controlled trial has shown that chelation meaningfully reduces tissue gadolinium and relieves the symptom cluster. (A 2024 paper claiming near-cure with chelation in GDD was subsequently retracted, which is exactly why this page does not rely on it.)
- It can be harmful. Chelators are not selective — they also strip out essential metals such as zinc, copper, and calcium, and aggressive chelation has caused dangerous mineral depletion, kidney injury, and, in the broader chelation-therapy literature, deaths from severe hypocalcemia. The chelator can also itself transiently liberate gadolinium and redistribute it.
- The testing is gamed. Provoked urine tests after a chelator dose predictably yield higher numbers than baseline in almost anyone, so a "high" provoked result is not evidence of disease and is not a valid trigger for treatment.
The honest position is that, at present, management of suspected gadolinium retention is supportive: treat pain and other symptoms, screen for and treat alternative diagnoses, avoid further unnecessary gadolinium exposure, and be skeptical of any program promising to "flush" the metal out. Anyone considering chelation should weigh that its benefit is unproven and its harms are real.
8. Prevention & Risk Reduction
Because gadolinium exposure is almost always a deliberate medical decision, prevention is unusually effective — risk is largely controlled by how, whether, and with which agent the contrast is given. The principles below reflect mainstream radiology guidance and are the reason NSF has nearly disappeared.
Screen kidney function before contrast
The single most important safeguard against NSF is knowing the patient's kidney function before injecting a GBCA. An eGFR below 30, dialysis dependence, or acute kidney injury marks a high-risk patient. In those patients, GBCAs are avoided unless the information is truly essential and cannot be obtained another way; if contrast is unavoidable, a stable macrocyclic agent at the lowest effective dose is used, and for dialysis patients, prompt dialysis after the scan is often arranged to speed clearance (though dialysis is not a guaranteed prevention of NSF). Screening turned NSF from a recognized hazard into a rarity.
Prefer macrocyclic agents and the lowest effective dose
When a contrast agent is chosen, the lower-retention macrocyclic agents (gadoterate, gadobutrol, gadoteridol) are preferred, and the dose is kept to the minimum needed for a diagnostic image. Using the smallest amount that answers the clinical question reduces the total gadolinium burden on every measure that matters.
Avoid unnecessary and unnecessarily repeated scans
Retention is cumulative and dose-related, so the most reliable way to limit it is to give fewer doses. That means asking, before every contrast MRI, whether contrast is genuinely needed for this question or whether an unenhanced MRI, ultrasound, or another test would suffice — and avoiding reflexive repeat contrast scans for conditions that can be followed without them. For people who will need many MRIs over a lifetime (for example, in long-term tumor or multiple-sclerosis surveillance), this thoughtful, contrast-only-when-it-changes-management approach is the practical heart of prevention.
Special situations and informed choice
GBCAs are used in pregnancy only when clearly necessary, since gadolinium crosses the placenta. The FDA's required Medication Guide exists so that patients can be informed that gadolinium is retained and can take part in the decision. None of this should frighten anyone away from a contrast MRI that their doctor judges necessary — the benefit of a correct diagnosis is usually decisive — but it does mean the decision should be a deliberate one: the right agent, the right dose, only when it adds real information.
9. Related Topics
- Heavy Metals — the broader family of toxic metals and how chelation, retention, and tissue burden are measured and (sometimes) treated.
- Lead — another metal where bone acts as a long-term reservoir and where unproven "detox" claims abound; a useful contrast to gadolinium's retention story.
- Kidney Disease — reduced kidney function is the master risk factor for NSF; this explains why eGFR gates gadolinium safety.
- Calcium — the essential mineral that free gadolinium mimics because their ionic radii are nearly identical, the basis of gadolinium's ionic toxicity.
- Zinc — an endogenous metal that can displace gadolinium from a chelate (transmetalation) and that aggressive chelation can deplete.
- Lab Tests — where the 24-hour urine gadolinium and related metal assays fit among diagnostic laboratory tests.
- All Minerals — the full mineral library, including the essential minerals gadolinium interacts with.
10. Key Research Papers
- Grobner T. Gadolinium – a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrology Dialysis Transplantation. 2006;21(4):1104–1108. The first report linking gadolinium contrast exposure in dialysis patients to NSF.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. Journal of the American Society of Nephrology. 2006;17(9):2359–2362. Epidemiologic confirmation implicating the linear agent gadodiamide.
- Kanda T, Ishii K, Kawaguchi H, Kitajima K, Takenaka D. High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose of a gadolinium-based contrast material. Radiology. 2014;270(3):834–841. The landmark paper showing dose-dependent brain signal change from gadolinium.
- McDonald RJ, McDonald JS, Kallmes DF, et al. Intracranial gadolinium deposition after contrast-enhanced MR imaging. Radiology. 2015;275(3):772–782. Demonstrated gadolinium deposition in brain tissue of patients with normal renal function.
- McDonald RJ, McDonald JS, Kallmes DF, et al. Gadolinium deposition in human brain tissues after contrast-enhanced MR imaging in adult patients without intracranial abnormalities. Radiology. 2017;285(2):546–554. Autopsy quantification of retained gadolinium in neurologically normal patients.
- Semelka RC, Ramalho J, Vakharia A, et al. Gadolinium deposition disease: initial description of a disease that has been around for a while. Magnetic Resonance Imaging. 2016;34(10):1383–1390. Proposes diagnostic criteria for the patient-reported GDD symptom cluster.
- Semelka RC, Commander CW, Jay M, Burke LMB, Ramalho M. Presumed gadolinium toxicity in subjects with normal renal function: a report of 4 cases. Investigative Radiology. 2016;51(10):661–665. Detailed case descriptions of chronic symptoms after gadolinium in normal-kidney patients.
- Gulani V, Calamante F, Shellock FG, Kanal E, Reeder SB; International Society for Magnetic Resonance in Medicine. Gadolinium deposition in the brain: summary of evidence and recommendations. The Lancet Neurology. 2017;16(7):564–570. Expert society review weighing retention evidence and clinical recommendations.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29(3):365–376. Review of chelate stability, transmetalation, and proposed toxicity mechanisms.
- U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA warns that gadolinium-based contrast agents (GBCAs) are retained in the body; requires new class warnings (2017–2018), and the FDA-required patient Medication Guide for GBCAs. fda.gov — GBCA retention safety communication.
- European Medicines Agency. Gadolinium-containing contrast agents: EMA's final opinion confirming restrictions on the use of linear agents (PRAC/CHMP referral, 2017). ema.europa.eu — gadolinium-containing contrast agents referral.
- American College of Radiology, Committee on Drugs and Contrast Media. ACR Manual on Contrast Media — chapters on Nephrogenic Systemic Fibrosis and on Gadolinium-Based Contrast Agents. acr.org — ACR Manual on Contrast Media.