Hyperchloremia (High Chloride): What the Evidence Shows
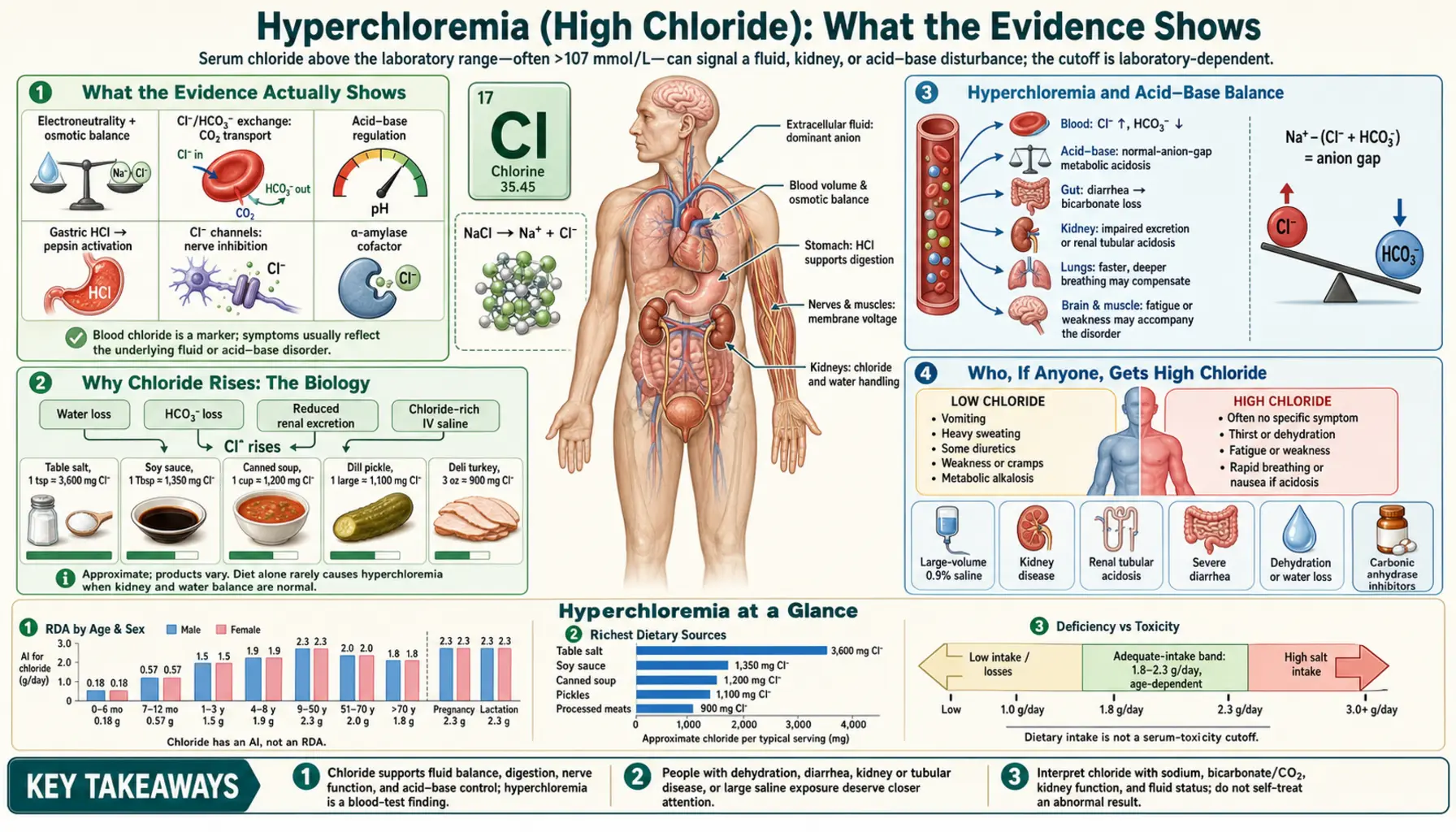
Here is the honest bottom line first: there is no recognized "chloride toxicity" syndrome that ordinary people get from food or supplements. Hyperchloremia simply means the chloride level in the blood is above the normal range (roughly 96–106 mmol/L), and it is almost never a disease in its own right — it is a marker that points to something else, usually a problem with body fluids, the kidneys, or acid–base balance. By far the most common way a person ends up with a high chloride level is being given large volumes of ordinary intravenous "normal saline" in a hospital, which is rich in chloride. High chloride itself usually causes no symptoms; whatever symptoms exist belong to the underlying cause — dehydration, diarrhea, kidney trouble, or a type of acid buildup. You cannot give yourself hyperchloremia by salting your food, and there is no useful home test or treatment for it. This page lays out what the evidence actually shows, the biology behind why chloride rises, the few situations where it matters, and the calm, practical takeaways — without inventing symptoms that do not exist. A high chloride value on a lab report is a clue for your doctor to interpret, not a poisoning to fear.
Table of Contents
- What the Evidence Actually Shows
- Why Chloride Rises: The Biology
- Hyperchloremia and Acid–Base Balance
- Who, If Anyone, Gets High Chloride
- How It Is Found and Interpreted
- What to Do About It
- When to Seek Care / Red Flags
- Related Minerals and Balance
- Key Research Papers
- Connections
- Featured Videos
What the Evidence Actually Shows
It is worth saying plainly, because the internet is full of vague warnings about "too much" of every mineral: chloride does not have a toxicity syndrome the way some substances do. You will not find a recognized clinical condition called "chloride poisoning" caused by eating salty food or taking a supplement. What clinicians do recognize is hyperchloremia — the lab finding that the concentration of chloride in the blood is higher than normal — and they treat it almost entirely as a signpost to an underlying disturbance rather than as a problem to be attacked directly.
Chloride is the most abundant negatively-charged electrolyte in the fluid outside your cells. The body keeps the blood level inside a fairly narrow window, usually reported as about 96 to 106 mmol/L (laboratories vary slightly). A value above that range is hyperchloremia. The single most important thing to understand is this: the number itself rarely tells you a person is sick, and high chloride on its own does not produce a distinctive set of symptoms. When something feels wrong, it is the cause — loss of body water, kidney dysfunction, or an acid–base shift — that is generating the symptoms, not the chloride ion behaving like a toxin.
Three honest points frame everything that follows:
- Diet and supplements essentially never cause it in healthy people. If your kidneys work normally, the body excretes extra chloride easily, just as it does extra sodium. A high-salt meal does not push a healthy person into hyperchloremia. This is the opposite of the popular worry that you can "overdose" on a common dietary mineral.
- The most common real-world cause is medical, not dietary. Large-volume infusion of 0.9% sodium chloride — ordinary "normal saline," a chloride-rich fluid — is the classic way hospitalized and critically ill patients develop a high chloride level. This is recognized well enough that it has driven major clinical trials comparing saline with lower-chloride "balanced" fluids.
- Hyperchloremia is usually a marker, and is best understood through acid–base balance. A rise in chloride very often travels with a particular kind of acid buildup in the blood (a normal–anion–gap, or "hyperchloremic," metabolic acidosis). Understanding that link explains nearly everything else on this page.
So this page is deliberately measured. It will not list a parade of frightening "symptoms of chloride toxicity," because that would be inventing a clinical picture that does not exist. Instead it explains the biology, the genuine situations where a high chloride level matters, and what a sensible person should actually do — which, for almost everyone, is very little.
Why Chloride Rises: The Biology
To understand hyperchloremia you only need one idea: chloride is the body's main partner anion, and it follows water, sodium, and acid–base accounting. Picture the bloodstream as a ledger that must always balance its electrical charges. Sodium is the dominant positive charge; chloride and bicarbonate are the two big negative charges that balance it. When one of those negatives goes down, the other tends to go up to keep the books balanced. That single accounting rule explains most of why chloride climbs.
There are three broad routes to a high chloride level:
- Concentration — losing water faster than chloride. If the body loses relatively more water than salt — through inadequate water intake, certain kinds of dehydration, or excessive free-water loss — the chloride that remains becomes more concentrated, and the measured level rises. Here, high chloride usually travels with a high or high-normal sodium, and the real issue is a water deficit, not a chloride excess. The fix is water, not "lowering chloride."
- Addition — giving chloride directly. The clearest example is intravenous 0.9% sodium chloride ("normal" saline), which actually contains more chloride than blood does (about 154 mmol/L versus the body's ~100). Pour enough of that into the circulation and the chloride level rises. Less commonly, large amounts of certain chloride-containing medications or, in someone with kidney trouble, salt substitutes and supplements can contribute.
- Acid–base shift — chloride rising as bicarbonate falls. This is the most important and most overlooked route. When the body loses bicarbonate — for example through severe diarrhea, which is rich in bicarbonate, or through certain kidney disorders — chloride rises to take its place on the ledger. The result is a hyperchloremic (normal–anion–gap) metabolic acidosis. Crucially, the chloride did not cause the problem; it rose because bicarbonate was lost.
An everyday analogy helps. Imagine a seesaw with bicarbonate on one side and chloride on the other, and the body insisting the seesaw stay level. If bicarbonate drops (lost in diarrhea, or diluted by large-volume saline), the only way to keep the seesaw level is for chloride to rise. The high chloride is the shadow of the bicarbonate problem — informative, but not the villain. This is also why simply trying to "get chloride down" misses the point: you treat the water deficit, stop or switch the offending fluid, or address the bicarbonate loss, and chloride follows on its own.
One more honest note about saline. The reason hospitals have studied this so carefully is that 0.9% saline was, for a century, the default resuscitation fluid — and it turns out its high chloride content can nudge patients toward hyperchloremic acidosis and, in some studies, kidney stress. That does not make saline "toxic"; it remains a workhorse fluid used safely countless times every day. It simply means that, in large volumes and in the sickest patients, the chloride load is not perfectly inert — which is exactly why the acid–base section below matters.
Hyperchloremia and Acid–Base Balance
If you remember only one section of this page, make it this one, because the link between chloride and acid–base balance is where a high chloride value earns its clinical meaning. The phrase clinicians use is hyperchloremic metabolic acidosis, also called normal–anion–gap acidosis. It sounds technical, but the plain-language version is simple: the blood has become slightly too acidic, and the reason is that bicarbonate (the body's main buffer, which neutralizes acid) has been lost and chloride has risen to fill the charge gap.
Why does the "anion gap" part matter? Doctors calculate a number called the anion gap to sort acid buildups into two families. In one family, an unmeasured acid accumulates (for example, the ketoacids of diabetic ketoacidosis or lactic acid in shock), and the anion gap is high. In the other family — the hyperchloremic one — no exotic acid is piling up; instead bicarbonate has simply been swapped for chloride, so the gap stays normal. Recognizing a normal-gap, hyperchloremic acidosis instantly narrows the list of causes and is one of the most useful bedside deductions in medicine.
The common causes of this hyperchloremic, normal-gap acidosis are worth knowing because they are the real situations behind most meaningful high-chloride readings:
- Gastrointestinal bicarbonate loss — especially diarrhea. Intestinal fluid is rich in bicarbonate. Severe or prolonged diarrhea pours bicarbonate out of the body; chloride rises to compensate, producing a hyperchloremic acidosis. This is one of the most common causes worldwide, and the treatment is to rehydrate and treat the diarrhea, not to target chloride.
- Renal tubular acidosis (RTA). In this group of kidney-tubule disorders, the kidney either cannot excrete acid properly or leaks bicarbonate into the urine. The blood again ends up with low bicarbonate and high chloride. RTA is uncommon but is a classic textbook cause of an unexplained hyperchloremic acidosis.
- Large-volume saline resuscitation. As described above, infusing liters of chloride-rich 0.9% saline can both dilute bicarbonate and add chloride, producing an "iatrogenic" (treatment-caused) hyperchloremic acidosis. This is precisely the effect that motivated the balanced-fluid trials.
- Other routes. Certain medications (for example, acetazolamide or, rarely, the carbonic-anhydrase effects of some drugs), recovery from a high-gap acidosis, and a few kidney and adrenal conditions can also produce the picture.
Does a mild hyperchloremic acidosis matter? Usually only modestly, and it is the underlying cause that determines how sick a person is. The honest, evidence-based nuance is this: in critically ill patients, observational studies have repeatedly associated higher chloride levels and hyperchloremic acidosis with worse outcomes — more kidney injury and, in some sepsis cohorts, higher mortality. But association is not the same as cause, and the large randomized trials that directly compared chloride-rich saline with lower-chloride balanced fluids have found, at most, modest differences. The reasonable summary is that a heavy chloride load is probably not perfectly harmless in the sickest patients, but it is not a poison either — and for anyone outside an intensive-care setting, a mildly high chloride is rarely a cause for alarm on its own.
Who, If Anyone, Gets High Chloride
Because hyperchloremia is a marker rather than a self-inflicted overdose, it shows up in a fairly predictable list of people and situations. If you are a generally healthy person eating a normal (even salty) diet, you are essentially not on this list. The genuine scenarios are:
- Hospitalized and critically ill patients receiving IV fluids. This is the big one. Anyone getting large volumes of 0.9% saline — during surgery, sepsis, trauma, or any resuscitation — can develop a high chloride level simply from the fluid. It is common enough that it is monitored routinely and is the reason "balanced" fluids exist.
- People with significant diarrhea or other GI fluid losses. Severe gastroenteritis, prolonged diarrhea, or losses through certain surgical drains can cause the bicarbonate-loss pattern that drives chloride up. Children and older adults with diarrheal illness are particularly relevant here.
- People with kidney disease or renal tubular acidosis. When the kidneys cannot handle acid and bicarbonate normally, chloride tends to run high. This includes both chronic kidney disease and the specific tubular disorders (RTA). See Kidney Disease.
- People with notable dehydration / water deficit. Anyone losing more water than salt — through inadequate intake, certain fevers, or excessive free-water loss — can show a concentrated, high chloride alongside a high-normal or high sodium. The problem is the water deficit, and it travels with the high-sodium picture covered on the Hypernatremia and Salt Excess page.
- People on specific medications. A few drugs (for example, acetazolamide and certain others that alter the kidney's acid handling) can produce a hyperchloremic acidosis. This is uncommon and is managed by reviewing the medication, not by treating chloride.
- Rare and edge cases. Recovery from diabetic ketoacidosis (as the gap acidosis resolves, a transient hyperchloremic acidosis can appear), certain adrenal conditions, and prolonged use of some chloride-containing preparations. These are the kind of situations a clinician identifies in context.
What is conspicuously absent from this list is "ate too much salt," "took a chloride supplement," or "drank too much electrolyte water." In a person with working kidneys, those do not cause hyperchloremia. That absence is the whole point: this is not a dietary toxicity, and framing it as one would be inaccurate.
How It Is Found and Interpreted
Hyperchloremia is almost always discovered on a routine blood test, not because of a symptom. Serum chloride is reported as part of a basic metabolic panel or a comprehensive metabolic panel (CMP) — the same everyday blood panels that report sodium, potassium, bicarbonate, kidney markers, and glucose. (For what those panels measure and how to read them, see the Comprehensive Metabolic Panel and Kidney Function pages.)
The key insight is that a chloride value is almost never interpreted alone. Clinicians read it in the company of the other electrolytes, because the pattern is what carries the meaning:
- Chloride with sodium. If sodium is high too, attention turns to a water deficit or salt excess (a hypernatremia story). If sodium is normal but chloride is disproportionately high, an acid–base process is more likely.
- Chloride with bicarbonate. The reciprocal relationship is the giveaway: a high chloride with a low bicarbonate is the fingerprint of a hyperchloremic (normal-gap) metabolic acidosis.
- The anion gap calculation. Using sodium, chloride, and bicarbonate, a doctor computes the anion gap to decide whether an acidosis is the hyperchloremic, normal-gap kind or the high-gap kind — a single calculation that reshapes the diagnostic search.
- The clinical context. Recent IV fluids, diarrhea, kidney function, and the medication list usually point straight at the cause. A high chloride in someone who just received liters of saline needs a very different response from the same value in someone with weeks of diarrhea.
A practical reassurance: a mildly high chloride on an otherwise normal panel, in a person who feels well, is frequently of little consequence — sometimes it simply reflects the lab's reference range, mild dehydration on the day of the draw, or a recent fluid. It is the pattern and the story, not the isolated number, that decide whether anything needs to be done.
What to Do About It
This is the low-key, practical part — and the honest answer for most people is "nothing special, and certainly nothing at home." There is no chloride-lowering diet, no detox, and no supplement that meaningfully or safely targets a blood chloride level. Because hyperchloremia is a marker, the entire approach is to find and address the cause; when the cause is handled, chloride normalizes on its own. Here is how that plays out:
- If it turned up on a routine panel and you feel well: a mildly high chloride usually needs no action beyond your doctor noting it and, if anything, making sure you are well hydrated. It is often rechecked rather than treated. Do not go looking for a "chloride-lowering" regimen — none is needed.
- If it is from dehydration / water deficit: the treatment is simply water (oral fluids, or in a hospital, appropriate IV fluid). Chloride falls as the water deficit corrects. This is the most common everyday scenario and the most reassuring.
- If it is from diarrhea or GI losses: the priority is rehydration and treating the underlying illness. Oral rehydration solutions are designed for exactly this. As the bicarbonate loss stops, the hyperchloremic acidosis resolves and chloride comes down.
- If it is from IV saline in a hospital: this is a clinical decision the care team makes — for instance, switching from 0.9% saline to a lower-chloride "balanced" fluid, or simply slowing fluids once resuscitation is complete. There is nothing for a patient to do here except be aware that the team monitors it.
- If it is from kidney disease or renal tubular acidosis: management belongs with a clinician (often a nephrologist) and centers on treating the kidney disorder — sometimes including bicarbonate replacement to correct the acidosis, which in turn brings chloride down. This is targeted at the acid–base problem, not at chloride directly.
- If a medication is responsible: the fix is to review and, if appropriate, adjust the drug with the prescriber — never to add a supplement to counteract it.
The unifying principle is worth repeating because it is the most useful thing on this page: you do not treat the chloride number; you treat why it is high. For the overwhelming majority of people who see a slightly elevated chloride on a lab report, the correct response is calm: drink water, follow up with your doctor about the pattern, and resist the urge to "fix" a single electrolyte that is only telling a story about water and acid–base balance.
When to Seek Care / Red Flags
Because hyperchloremia itself is silent and is only a marker, the things that should prompt medical attention are the signs of the underlying conditions that drive chloride up — not a chloride number on its own. Seek medical care promptly if you have any of the following:
- Signs of significant dehydration — persistent thirst, very dark or scant urine, dizziness or lightheadedness on standing, dry mouth, confusion, or (in children) no wet diapers and no tears when crying.
- Severe or prolonged diarrhea or vomiting — especially when you cannot keep fluids down, in a young child or older adult, or lasting more than a couple of days. This is the common driver of hyperchloremic acidosis and of dangerous fluid loss.
- Rapid or deep breathing, marked fatigue, or confusion — these can be signs that an acidosis (from any cause) is becoming significant and needs evaluation.
- Known kidney disease with new illness, vomiting, or diarrhea — people with reduced kidney function can shift electrolytes and acid–base balance quickly and should have a low threshold for being checked.
- A high chloride reported alongside symptoms you cannot explain — bring the result to your doctor so the whole pattern (sodium, bicarbonate, kidney markers, and the anion gap) can be interpreted together.
What does not warrant alarm is an isolated, mildly elevated chloride on a routine panel in someone who feels well — that is a routine finding to mention at your next visit, not an emergency. And to be clear about the reassuring side of this topic: there is no scenario in which a normal diet, table salt, or an electrolyte drink causes a dangerous chloride level in a healthy person. If you are worried after seeing the number, the best single step is a conversation with your clinician, who can place it in context within minutes.
Related Minerals and Balance
Chloride never acts alone, and understanding its companions makes a high value far less mysterious. The most useful relationships to know:
- Sodium. Sodium and chloride travel together as the body's main salt pair, and they are usually gained and lost together. A high chloride that comes with a high sodium points toward a water deficit or salt excess — the territory of Hypernatremia and Salt Excess. The broader role of sodium and chloride in fluid balance is covered on the Sodium page.
- Bicarbonate. Chloride's most important partner in interpreting a high value is bicarbonate — the two reciprocate to keep the blood's charges balanced, so a high chloride with a low bicarbonate is the signature of hyperchloremic acidosis. Bicarbonate is reported on the same metabolic panel.
- Potassium. Potassium balance is intertwined with acid–base status, and some of the conditions that disturb chloride (such as renal tubular acidosis or diarrhea) also shift potassium. For the high side of potassium, see Hyperkalemia (High Potassium); the Potassium overview covers its broader role.
- Chloride deficiency, the other side. Far more clinically common than excess is low chloride (hypochloremia), which often accompanies vomiting, certain diuretics, and a different acid–base picture. See the Chloride Deficiency hub for that side of the story, and the Chloride overview for what this electrolyte does day to day.
Seeing chloride as one entry in a small, interlocking ledger — sodium and chloride for salt and water, chloride and bicarbonate for acid–base — is the antidote to treating a single high number as a poisoning. It is a clue about balance, and balance is what the body, and your doctor, are actually managing.
Key Research Papers
- Berend K, van Hulsteijn LH, Gans RO (2012). Chloride: the queen of electrolytes? European Journal of Internal Medicine;23(3):203-211. — DOI: 10.1016/j.ejim.2011.11.013
- Nagami GT (2016). Hyperchloremia — Why and how. Nefrología;36(4):347-353. — DOI: 10.1016/j.nefro.2016.04.001
- Bandak G, Kashani KB (2017). Chloride in intensive care units: a key electrolyte. F1000Research;6:1930. — DOI: 10.12688/f1000research.11401.1
- Yunos NM, Bellomo R, Hegarty C, et al. (2012). Association Between a Chloride-Liberal vs Chloride-Restrictive Intravenous Fluid Administration Strategy and Kidney Injury in Critically Ill Adults. JAMA;308(15):1566-1572. — DOI: 10.1001/jama.2012.13356
- Raghunathan K, Shaw A, Nathanson B, et al. (2014). Association Between the Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With Sepsis. Critical Care Medicine;42(7):1585-1591. — DOI: 10.1097/CCM.0000000000000305
- Neyra JA, Canepa-Escaro F, Li X, et al. (2015). Association of Hyperchloremia With Hospital Mortality in Critically Ill Septic Patients. Critical Care Medicine;43(9):1938-1944. — DOI: 10.1097/CCM.0000000000001161
- Suetrong B, Pisitsak C, Boyd JH, et al. (2016). Hyperchloremia and moderate increase in serum chloride are associated with acute kidney injury in severe sepsis and septic shock patients. Critical Care;20(1):315. — DOI: 10.1186/s13054-016-1499-7
- Krajewski ML, Raghunathan K, Paluszkiewicz SM, et al. (2015). Meta-analysis of high- versus low-chloride content in perioperative and critical care fluid resuscitation. British Journal of Surgery;102(1):24-36. — DOI: 10.1002/bjs.9651
- Semler MW, Self WH, Wanderer JP, et al. (2018). Balanced Crystalloids versus Saline in Critically Ill Adults. New England Journal of Medicine;378(9):829-839. — DOI: 10.1056/NEJMoa1711584
- Self WH, Semler MW, Wanderer JP, et al. (2018). Balanced Crystalloids versus Saline in Noncritically Ill Adults. New England Journal of Medicine;378(9):819-828. — DOI: 10.1056/NEJMoa1711586
PubMed Topic Searches
- PubMed — Hyperchloremia: causes, diagnosis, and management
- PubMed — Hyperchloremic (normal-anion-gap) metabolic acidosis
- PubMed — Saline chloride load, balanced fluids, and kidney injury
- PubMed — Serum chloride and outcomes in critically ill patients
- PubMed — Renal tubular acidosis and hyperchloremia
Connections
- Chloride Overview
- Hypochloremia (Low Chloride) Hub
- Sodium Overview
- Hypernatremia and Salt Excess
- Potassium Overview
- Hyperkalemia (High Potassium) Hub
- Comprehensive Metabolic Panel
- Kidney Function Tests
- Kidney Disease
- Acute Kidney Injury
- Diabetes
- All Minerals