Hypochloremia (Low Chloride): Vomiting and Dehydration
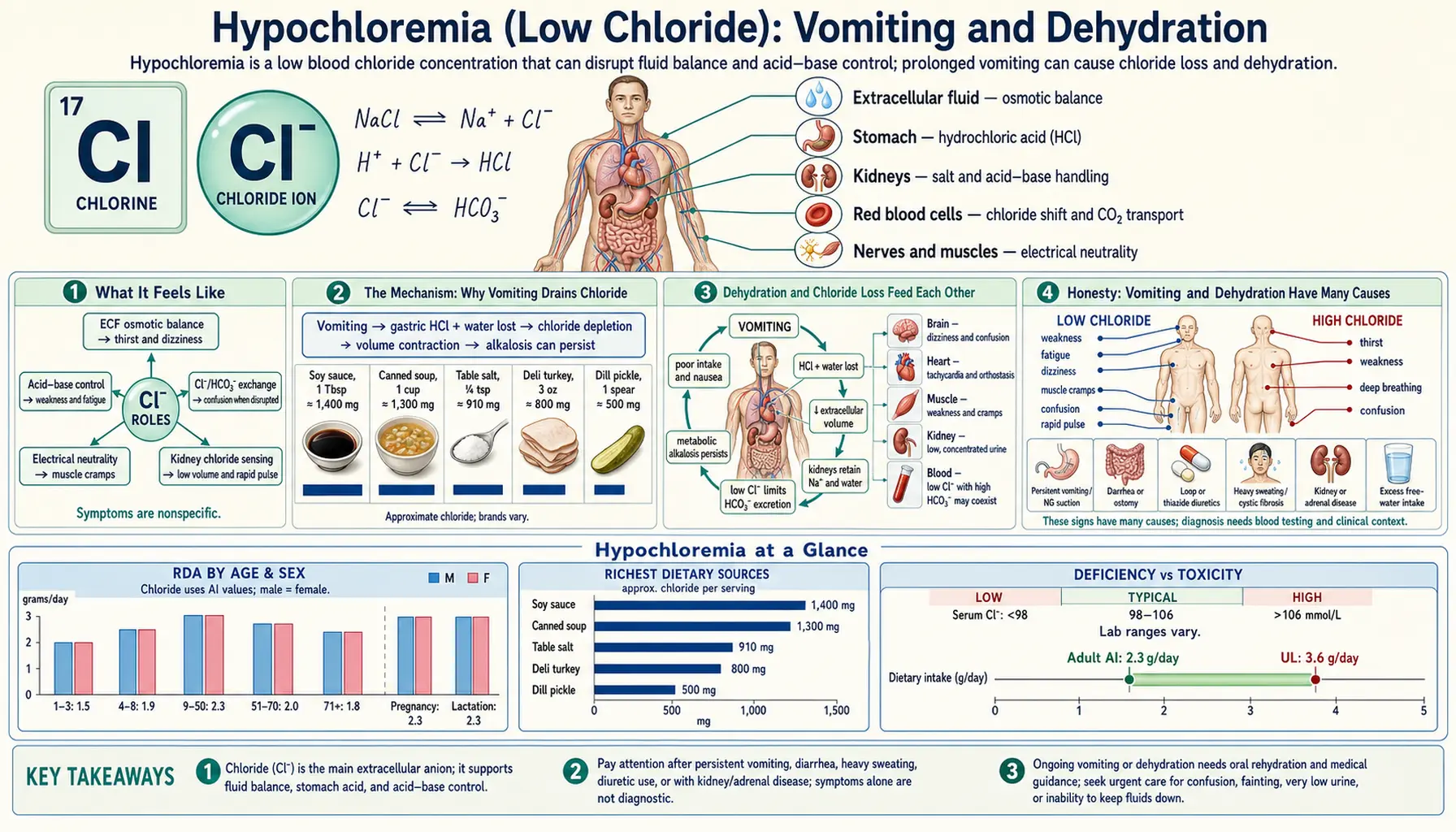
When you vomit, you don't just lose your last meal — you lose stomach acid, and stomach acid is built from chloride. Each wave of vomiting pours hydrochloric acid out of the body, and with it goes a large share of the body's chloride and a great deal of water and salt. After a bad bout of food poisoning, a stomach bug, a migraine that won't stop, or weeks of morning sickness, the result is a recognizable trio: a low blood chloride level (hypochloremia), the dry-mouthed, light-headed, sunken feeling of dehydration and lost fluid volume, and a blood chemistry tipped toward alkali. This page explains why vomiting drains chloride specifically, why that makes you feel so wrung out, how dehydration and chloride loss feed each other, and how the whole thing is corrected — usually with the right kind of fluid rather than chloride pills.
Table of Contents
- What It Feels Like
- The Mechanism: Why Vomiting Drains Chloride
- Dehydration and Chloride Loss Feed Each Other
- Honesty: Vomiting and Dehydration Have Many Causes
- Clues That It's a Chloride Problem
- Common Situations That Cause It
- Getting Tested
- Correcting It Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What It Feels Like
The hypochloremia of vomiting rarely announces itself as a single, distinct symptom. Instead, what people actually feel is the combined picture of losing fluid and salt — because chloride leaves the body alongside water and sodium, the two travel together. After repeated vomiting, the common experience is:
- A parched, sticky mouth and intense thirst — the body is signaling that its fluid tank is running low.
- Light-headedness or dizziness on standing up — rising from a chair or bed brings a head-rush, a gray-out, or the room tilting. This orthostatic dizziness is one of the most reliable signs that fluid volume has dropped.
- Dark, scanty urine — going far less often, and the urine is deep yellow or amber. The kidneys are clamping down to conserve every drop of water and salt.
- Fatigue, weakness, and a wrung-out feeling — a flat, drained heaviness that's hard to describe but easy to recognize after a rough night over the toilet.
- A fast or pounding heartbeat — the heart speeds up to keep blood moving when the circulating volume has shrunk.
- Muscle cramps and twitches — because vomiting depletes potassium and magnesium at the same time, cramping often rides along.
As the chloride and acid losses tip the blood toward alkali (a state called metabolic alkalosis), some people also notice tingling around the lips or in the fingertips, and in more advanced cases slow, shallow breathing as the lungs try to hold on to carbon dioxide to compensate. But for most people in the early going, the dominant feeling is simply dehydration: dry, dizzy, thirsty, and worn out. Hypochloremia itself produces no unique sensation you could point to — it is a number on a blood test that travels with how dried-out you feel.
The Mechanism: Why Vomiting Drains Chloride
Chloride is the most abundant negative ion (anion) in the fluid outside your cells, and it does quiet but essential work: it partners with sodium to hold water in the bloodstream, it keeps the body's acid–base books balanced, and — the key fact here — it is the raw material for stomach acid. The cells lining your stomach pump hydrogen ions (H+) and chloride ions (Cl−) into the stomach to make hydrochloric acid (HCl), the acid that digests food and kills swallowed germs.
Here is the elegant detail that explains everything that follows. Every time a stomach cell secretes one hydrogen ion into the stomach to make acid, it releases one bicarbonate ion (HCO3−) into the bloodstream in exchange. Physiologists call this the “alkaline tide” — the brief rise in blood alkalinity that normally follows a meal. Under ordinary circumstances it's no problem: the acid you made does its job in the gut, gets neutralized further down the intestine, and the bicarbonate is reabsorbed, so the books balance out.
Vomiting breaks that balance. When you throw up, you remove the hydrochloric acid before it can be neutralized downstream. The body keeps making more acid (and keeps dumping bicarbonate into the blood to do so), but the acid never returns — it ends up in the toilet. So with each episode of vomiting you lose chloride and hydrogen out the top end, while bicarbonate quietly accumulates in the blood. The result is the classic combination: low chloride and high bicarbonate — a chloride-depletion metabolic alkalosis.
An analogy. Think of the body's chloride supply like the change in a cash register at a busy shop. Normally the cashier (your stomach) hands out coins (chloride and acid) to customers, but those coins circulate and come back into the till by the end of the day. Vomiting is like every customer walking out the door with the coins and never returning. The shop keeps opening the register and handing out more change, drawing down the float, and meanwhile IOUs (bicarbonate) pile up on the counter to cover the missing cash. Run that long enough and the till is empty of coins and stuffed with paper — low chloride, high bicarbonate — and the only fix is to restock the register with actual coins (chloride) and the water they came dissolved in.
Crucially, the chloride lost in vomit does not leave alone. It is dissolved in stomach fluid, so vomiting also strips out water and, to a lesser extent, sodium and potassium. That is why hypochloremia from vomiting is almost never an isolated finding — it arrives hand in hand with dehydration and volume depletion, the subject of the next section.
Dehydration and Chloride Loss Feed Each Other
Doctors draw a careful distinction between two words people use interchangeably. Dehydration strictly means a deficit of water (which raises the blood's salt concentration and makes you thirsty), while volume depletion means a loss of salt-containing fluid from the bloodstream (which lowers blood pressure and makes you dizzy on standing). Vomiting causes mostly the second — you lose salty stomach fluid, not pure water — though in everyday speech both get called “dehydration,” and the practical experience overlaps. The distinction matters because it tells you what to replace: not just water, but water with salt in it.
What makes the chloride problem and the fluid problem reinforce each other is the kidney. Faced with a shrinking blood volume, the kidneys do exactly what they should: they hold on to sodium and water to defend blood pressure. But here is the catch — to reabsorb sodium, the kidney needs chloride to come along as sodium's partner anion. When chloride is in short supply, the kidney has a workaround: it reabsorbs sodium in exchange for pumping out hydrogen and potassium instead. That defends the blood volume, but it does two unhelpful things: it makes the body even more alkaline (by excreting acid in the urine, producing the puzzling “paradoxical aciduria” — acidic urine in an alkaline body), and it burns through potassium, deepening the low-potassium state.
This is the vicious cycle that researchers describe as chloride-depletion alkalosis: low chloride doesn't just accompany dehydration and alkalosis — it actively maintains them. As long as chloride stays low, the kidney can't switch back to its normal mode, the alkalosis won't correct, and the body keeps wasting potassium. The landmark insight, captured in the title of a much-cited 2012 commentary, is that this is fundamentally chloride depletion, not merely “dehydration” or “contraction” of fluid — and that is why giving plain salt-free water, or even a non-chloride salt, fails to fix it. The cycle only breaks when you give back the missing ingredient: chloride, delivered in a salty fluid the body can use.
Honesty: Vomiting and Dehydration Have Many Causes
It is important to be straight about this: vomiting and dehydration are extremely common, and low chloride is the consequence, not usually the original cause. Almost anything that makes you throw up — a stomach virus, food poisoning, a migraine, motion sickness, a hangover, pregnancy, a reaction to medication, a bowel obstruction — can drain chloride if it goes on long enough. Finding hypochloremia on a blood test tells your clinician that you've been losing acid and fluid; it does not diagnose why you were vomiting. The hunt for the underlying cause is the more important task.
It also works the other way: many things cause dehydration without lowering chloride, and some even raise it. A few examples worth knowing, so the chloride number is read in context:
- Diarrhea tends to do the opposite of vomiting. Stool is rich in bicarbonate and relatively poor in acid, so heavy diarrhea usually causes a high-chloride, acidic state (metabolic acidosis), not the low-chloride alkalosis of vomiting. When both vomiting and diarrhea happen together, the chloride can land anywhere depending on which loss dominates.
- Pure water loss — heavy sweating in heat, fever, or simply not drinking enough — dehydrates you but often raises sodium and chloride concentrations rather than lowering them.
- Diuretics (“water pills”) can lower chloride and cause an alkalosis that mimics the vomiting picture, because they make the kidney waste chloride directly — no vomiting required.
- Other causes of low chloride include heart failure and its treatment, certain kidney and adrenal conditions, and over-breathing — none of which involve vomiting at all.
So while vomiting is the textbook cause of hypochloremia, the symptom of feeling dried-out and queasy is shared by many conditions. Low chloride is a useful fingerprint of acid-and-fluid loss, not a stand-alone diagnosis. (For the closely related symptom picture when sodium falls during vomiting, see Hyponatremia: Nausea and Vomiting; for low potassium's queasiness and weakness, see Hypokalemia and Nausea.)
Clues That It's a Chloride Problem
When does a doctor look at low chloride and dehydration and think specifically about the vomiting–alkalosis cycle? A handful of clues point that way:
- A clear story of vomiting or gastric suction. The single biggest clue is the history: days of a stomach bug, recurrent vomiting from a migraine, self-induced vomiting, hyperemesis of pregnancy, or a hospital nasogastric tube draining the stomach. All of these remove acid directly.
- Low chloride plus high bicarbonate (a low chloride with a high CO2 on the metabolic panel). This pairing — chloride down, bicarbonate up — is the chemical signature of chloride-depletion alkalosis and is what separates the vomiting picture from, say, diarrhea or dehydration from heat.
- A low urine chloride. A simple urine test showing very little chloride (typically under ~20 mmol/L) confirms that the body is desperately conserving chloride and that the problem is “chloride-responsive” — meaning it will get better when chloride-containing fluid is given. (A high urine chloride points instead toward diuretics or certain hormonal causes.)
- Low potassium tagging along. Because the kidney trades potassium to hold sodium when chloride is scarce, a simultaneously low potassium strengthens the case and is part of the same mechanism.
- Orthostatic signs. A drop in blood pressure or a jump in heart rate on standing — alongside dry mouth, dark urine, and the vomiting history — rounds out the volume-depletion picture.
Put together, the combination of a vomiting history, low chloride with high bicarbonate, low urine chloride, and signs of fluid loss is what makes this a recognizable, treatable pattern rather than an unexplained lab abnormality.
Common Situations That Cause It
Anything that produces repeated or prolonged vomiting — or that physically removes stomach contents — can drive chloride low. The everyday culprits include:
- Stomach bugs (gastroenteritis) and food poisoning. The most common cause by far. A day or two of vigorous vomiting from a norovirus or contaminated food can meaningfully drop chloride and fluid, especially in children and older adults who dehydrate quickly.
- Severe morning sickness (hyperemesis gravidarum). When pregnancy nausea becomes relentless vomiting, women can develop marked hypochloremia, alkalosis, and dehydration — one of the classic reasons for IV fluids in early pregnancy.
- Migraine and other causes of cyclic vomiting. A migraine that triggers hours of vomiting, or cyclic vomiting syndrome, can repeatedly drain acid and chloride.
- Self-induced vomiting. In eating disorders such as bulimia, repeated purging produces a textbook chloride-depletion alkalosis with low chloride and low potassium, often the first laboratory clue to what is happening.
- Bowel obstruction and pyloric stenosis. A blockage where the stomach empties causes acid-rich vomiting; in infants, pyloric stenosis is the classic cause of severe hypochloremic alkalosis.
- Nasogastric suction. In the hospital, a tube draining the stomach removes acid continuously — effectively “mechanical vomiting” — and is a frequent cause of low chloride in surgical and ICU patients.
- Heavy alcohol use. Binge drinking and the vomiting that accompanies it, layered on poor intake, can produce low chloride alongside low potassium and magnesium.
Two contributors that lower chloride without vomiting deserve a mention because they're easy to overlook: diuretics, which make the kidney waste chloride, and diabetic emergencies and refeeding, where fluid and electrolyte shifts can disturb chloride. Sorting out which mechanism is at work changes the treatment, which is why the history and the urine chloride matter so much.
Getting Tested
Confirming low chloride is simple and cheap. Chloride is one of the four electrolytes reported on a Comprehensive Metabolic Panel (CMP) — a routine blood draw — alongside sodium, potassium, and bicarbonate (often labeled CO2). The normal range for serum chloride is roughly 96–106 mmol/L; hypochloremia means a value below that range. The CMP also reports kidney function and glucose, which help point to the underlying cause and to dehydration.
The real diagnostic power comes from reading chloride together with the other numbers:
- Chloride down, bicarbonate (CO2) up — the signature of chloride-depletion metabolic alkalosis from vomiting.
- Potassium — frequently low at the same time, for the reasons described above.
- Sodium — may be low, normal, or high depending on how much water versus salt was lost; a low sodium points toward hyponatremia riding along.
- Kidney markers (BUN and creatinine) — often rise transiently when fluid volume is down, then settle once rehydration is complete.
- Urine chloride — a separate, inexpensive test that, when low, confirms the problem is chloride-responsive and will correct with the right fluids.
- Blood gas — in sicker patients, an arterial or venous blood gas measures pH directly and quantifies the alkalosis.
Because magnesium is not included on a standard CMP, a separate magnesium level is often added when vomiting has been prolonged, since it's commonly depleted too and affects how readily potassium recovers. The bottom line: a single ordinary blood panel both confirms hypochloremia and, by the company it keeps, points to the cause and the fix.
Correcting It Safely
The encouraging news is that hypochloremia from vomiting is one of the most readily reversible electrolyte problems — you almost never need a chloride supplement. Because the deficit is really “salty fluid lost from the stomach,” the treatment is to replace salty fluid, and the chloride comes built in. The pace and route depend on how dehydrated and how sick the person is.
- Stop or slow the vomiting and rehydrate by mouth, for mild cases. When someone can keep fluids down, the foundation is oral rehydration: small, frequent sips of a fluid that contains both salt and a little sugar, which helps the gut absorb the salt and water together. A commercial oral rehydration solution (ORS) or an electrolyte drink works well; broth and salty soups also supply sodium chloride. Plain water alone is not ideal after heavy vomiting, because it replaces the water but not the chloride, sodium, and potassium that were lost — and can even dilute the blood's sodium further. Oral rehydration therapy is one of the great public-health advances of the past century precisely because this simple salt-and-sugar fluid corrects exactly this kind of loss.
- Anti-nausea medication — prescribed when vomiting won't stop on its own, to break the cycle and let oral rehydration work.
- Intravenous (IV) saline — the mainstay when vomiting is severe, the person can't keep fluids down, or dehydration is significant. Normal saline (0.9% sodium chloride) is the classic choice because it restores both fluid volume and chloride at once — it directly refills the empty till. Giving the chloride is what finally lets the kidney stop wasting acid and potassium, so the alkalosis corrects as the chloride does. This is why “chloride-responsive” alkalosis gets better with saline.
- Replace potassium (and magnesium) too. Because vomiting depletes potassium and often magnesium alongside chloride, these are checked and replaced — potassium is frequently added to the IV fluids, and stubborn low potassium often won't budge until magnesium is corrected.
- Treat the cause. Rehydration buys time, but the lasting fix is addressing why the vomiting happened — treating the infection, managing the migraine, relieving an obstruction, supporting recovery in pregnancy, or getting help for an eating disorder.
A practical caution: in people with heart failure, kidney disease, or who are on fluid-restricting medications, the amount and type of fluid is individualized by a clinician — more is not automatically better. But for the otherwise healthy person dried out by a stomach bug, the principle is simple and time-tested: replace the lost salty fluid, by mouth if you can, by vein if you can't, and the chloride takes care of itself.
When to Seek Care / Red Flags
Most short-lived vomiting is ridden out at home with sips of an electrolyte fluid. But certain features mean it's time to get medical help rather than wait it out — because at that point dehydration, low chloride, and the electrolyte shifts that travel with them can become dangerous:
- Vomiting that won't stop — lasting more than about a day in an adult, or being unable to keep down even small sips of fluid.
- Signs of significant dehydration — no urination for 8–12 hours or very dark urine, no tears, severe dizziness or fainting on standing, a racing heart, or marked weakness and confusion.
- Vomiting blood, or material that looks like coffee grounds, or severe or constant abdominal pain — which can signal a serious cause needing urgent evaluation.
- A high fever, a stiff neck, or a severe headache with the vomiting.
- Tingling around the mouth or fingers, muscle twitching or cramps, or an irregular heartbeat — possible signs that the alkalosis and the low potassium and calcium that accompany it are affecting nerves and the heart.
- Vulnerable people, lower threshold. Infants and young children, older adults, pregnant women with relentless vomiting (possible hyperemesis gravidarum), people with diabetes, and anyone with kidney or heart disease can deteriorate quickly and should be seen sooner.
The reassuring counterpoint is that the fix is usually straightforward once care is reached: a quick blood panel confirms the picture, and IV saline restores both the fluid and the chloride, with the alkalosis and potassium correcting as they're replaced. When in doubt, err toward being checked — confirming or treating dehydration is fast and low-risk.
Key Research Papers
- Berend K, van Hulsteijn LH, Gans ROB (2012). Chloride: The queen of electrolytes? European Journal of Internal Medicine;23(3):203-211. — DOI: 10.1016/j.ejim.2011.11.013
- Galla JH (2000). Metabolic Alkalosis. Journal of the American Society of Nephrology;11(2):369-375. — DOI: 10.1681/ASN.V112369
- Luke RG, Galla JH (2012). It Is Chloride Depletion Alkalosis, Not Contraction Alkalosis. Journal of the American Society of Nephrology;23(2):204-207. — DOI: 10.1681/ASN.2011070720
- Garella S, Chang BS, Kahn SI (1991). Chloride-depletion metabolic alkalosis induces ECF volume depletion via internal fluid shifts. European Journal of Clinical Investigation;21(3):273-279. — DOI: 10.1111/j.1365-2362.1991.tb01370.x
- Tinawi M (2021). Pathophysiology, Evaluation, and Management of Metabolic Alkalosis. Cureus;13(1):e12841. — DOI: 10.7759/cureus.12841
- Bhave G, Neilson EG (2011). Volume Depletion Versus Dehydration: How Understanding the Difference Can Guide Therapy. American Journal of Kidney Diseases;58(2):302-309. — DOI: 10.1053/j.ajkd.2011.02.395
- Spital A (2007). Dehydration versus Volume Depletion — and the Importance of Getting it Right. American Journal of Kidney Diseases;49(5):721-722. — DOI: 10.1053/j.ajkd.2007.03.012
- Brown D, Wagner CA (2012). Molecular Mechanisms of Acid-Base Sensing by the Kidney. Journal of the American Society of Nephrology;23(5):774-780. — DOI: 10.1681/ASN.2012010029
- Nozaki Y, Kashihara T, Yamamoto S, et al. (2023). Persistent Hypochloremia Is Associated with Adverse Prognosis in Patients Repeatedly Hospitalized for Heart Failure. Journal of Clinical Medicine;12(4):1257. — DOI: 10.3390/jcm12041257
- Sterns RH (2015). Disorders of Plasma Sodium — Causes, Consequences, and Correction. New England Journal of Medicine;372(1):55-65. — DOI: 10.1056/NEJMra1404489
- Nalin DR, Cash RA (2021). Issues and Controversies in the Evolution of Oral Rehydration Therapy (ORT). Tropical Medicine and Infectious Disease;6(1):34. — DOI: 10.3390/tropicalmed6010034
- Ruxin JN (1994). Magic bullet: the history of oral rehydration therapy. Medical History;38(4):363-397. — DOI: 10.1017/S0025727300036905
PubMed Topic Searches
- PubMed — Vomiting, hypochloremia, and metabolic alkalosis
- PubMed — Chloride-depletion alkalosis and volume depletion
- PubMed — Oral rehydration therapy for fluid and electrolyte loss
- PubMed — Hyperemesis gravidarum and electrolyte disturbance
- PubMed — Urine chloride and saline-responsive alkalosis
Connections
- Hypochloremia Symptom Hub
- Hypochloremia and Metabolic Alkalosis
- Chloride Overview
- Sodium
- Hyponatremia: Nausea and Vomiting
- Potassium
- Hypokalemia and Nausea
- Hypokalemia Symptom Hub
- Magnesium
- Comprehensive Metabolic Panel
- Nausea and Vomiting
- Chronic Diarrhea
- Gastroesophageal Reflux Disease (GERD)
- Eating Disorders