Lipase Test: Diagnosing Acute Pancreatitis and Pancreatic Disease
Serum lipase is the most reliable blood test for diagnosing acute pancreatitis. Produced almost exclusively by pancreatic acinar cells, lipase catalyzes the breakdown of dietary fats (triglycerides) in the small intestine. When the pancreas is inflamed or injured, lipase leaks into the bloodstream, where it can be measured. Elevations three times above the upper limit of normal (ULN) are considered diagnostic of acute pancreatitis, with sensitivity and specificity each approaching 95–100% in the right clinical context. Unlike amylase — which also comes from the salivary glands — lipase is far more pancreas-specific, making it the preferred single test for acute pancreatitis worldwide.
Table of Contents
- Overview — What Is Serum Lipase?
- Biochemistry: How Lipase Works
- Reference Ranges and the 3× ULN Threshold
- Lipase vs. Amylase: Which Test to Order
- Pancreatic Causes of Elevated Lipase
- Non-Pancreatic Causes of Elevated Lipase
- When Lipase Is Falsely Normal
- Pancreatitis Severity: Atlanta Classification and BISAP Score
- Clinical Use: What Happens After a High Lipase Result
- Key Research and Citations
- Connections
- Featured Videos
Overview — What Is Serum Lipase?
Lipase is a family of enzymes that hydrolyze ester bonds in lipids — essentially splitting fatty acid chains away from glycerol backbones in triglycerides, phospholipids, and cholesterol esters. The pancreatic form, pancreatic lipase (also called triacylglycerol lipase), is the primary digestive enzyme for dietary fats. It is secreted by pancreatic acinar cells in an active form (unlike proteases such as trypsin, which are secreted as inactive zymogens to prevent self-digestion).
In normal physiology, only trace amounts of lipase enter the bloodstream. When the pancreas is acutely injured — whether from gallstones obstructing the pancreatic duct, alcohol causing direct acinar toxicity, or other triggers — the barrier between pancreatic secretions and the bloodstream breaks down. Lipase floods into the systemic circulation and can be measured within 4–8 hours of injury onset. Unlike amylase, which peaks at 24 hours and returns to normal in 3–5 days, lipase stays elevated for 8–14 days after an acute episode. This longer window makes lipase more useful for patients who present days after symptom onset.
Lipase testing became routine in the 1970s, and modern turbidimetric and colorimetric enzyme assays have made it a standard component of any abdominal pain workup. Normal serum lipase is typically 0–60 U/L (units per liter), though laboratory reference ranges vary slightly by assay and by age.
Biochemistry: How Lipase Works
Pancreatic lipase (PL, gene PNLIP) is a 48 kDa serine hydrolase — one of the most abundant proteins secreted by the exocrine pancreas, accounting for roughly 3–4% of total pancreatic protein output. Its three-dimensional structure features a classic alpha/beta hydrolase fold with a catalytic triad (Ser152 – Asp176 – His263) embedded in a buried active site that becomes accessible only when lipase binds its cofactor, colipase.
The Lipase-Colipase Interface
In the duodenum, bile salts coat fat droplets. Paradoxically, bile salts inhibit pancreatic lipase at an oil-water interface by displacing it. Colipase — a small 10 kDa cofactor secreted alongside lipase — rescues this inhibition by anchoring lipase to the bile-salt-coated surface. The lipase-colipase-bile salt complex then efficiently hydrolyzes surface triglycerides to 2-monoglycerides and two free fatty acids, which are absorbed by intestinal enterocytes via micelles.
Additional Pancreatic Lipases
Beyond classical pancreatic lipase, the pancreas secretes related enzymes that contribute to fat absorption:
- Pancreatic lipase-related protein 2 (PLRP2): Hydrolyzes phospholipids and galactolipids; important in infants before bile salt-stimulated lipase matures.
- Carboxyl ester lipase (CEL, bile salt-stimulated lipase): Broad substrate specificity — cholesterol esters, vitamins A/D/E/K, and lysophospholipids. Activated by bile salts directly.
- Phospholipase A2 (PLA2): Cleaves the sn-2 fatty acid from phospholipids; particularly important for phosphatidylcholine hydrolysis.
Commercial serum lipase assays generally measure the activity of classical pancreatic lipase (PNLIP), not the related enzymes. This specificity underpins the test's clinical utility.
Release Kinetics in Acute Pancreatitis
When pancreatic acinar cells are injured, intracellular vesicle fusion disrupts the normal secretory pathway. Digestive enzymes that would normally be exported apically into pancreatic ducts instead leak basally into the interstitium and then into blood and lymphatics. For lipase:
- Rises: 4–8 hours after acute pancreatic injury (slightly later than amylase at 2–6 hours)
- Peaks: 24–48 hours after onset
- Normalizes: 8–14 days (vs. 3–5 days for amylase)
This prolonged elevation window is clinically valuable: a patient arriving 4–5 days after their abdominal pain began may have normal amylase but still have a clearly elevated lipase, allowing retrospective diagnosis.
Reference Ranges and the 3× ULN Threshold
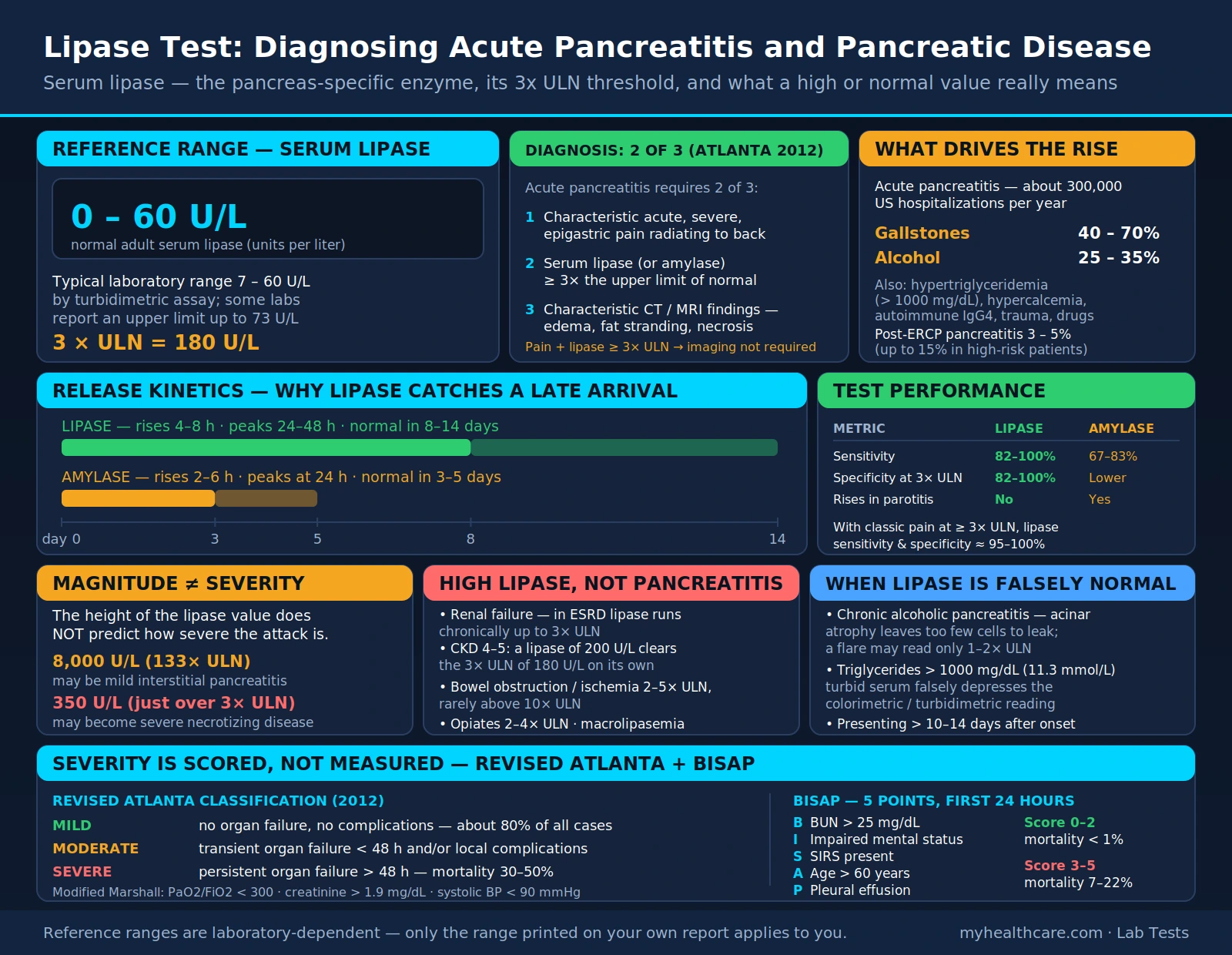
The normal reference range for serum lipase in adults is approximately 0–60 U/L, though individual laboratories may report slightly different upper limits of normal (ULN) depending on the specific assay method and reference population used (typical laboratory range: 7–60 U/L by turbidimetric assay; some labs report up to 73 U/L).
The 3× ULN Diagnostic Threshold for Acute Pancreatitis
A lipase elevation alone — even a 2-fold elevation — is not sufficient to diagnose acute pancreatitis. The 2012 revised Atlanta Classification requires at least two of three criteria for acute pancreatitis diagnosis:
- Characteristic abdominal pain (acute, severe, epigastric, often radiating to the back)
- Serum lipase (or amylase) ≥3× the upper limit of normal
- Characteristic imaging findings on CT or MRI (pancreatic edema, peripancreatic fat stranding, necrosis)
When a patient presents with classic epigastric pain and lipase ≥3× ULN, imaging is not required for diagnosis (though CT may still be obtained to assess severity or rule out complications). Using the 3× ULN threshold dramatically improves specificity compared to any detectable elevation, because mild lipase elevations (1–3× ULN) occur in many non-pancreatic conditions including renal failure and bowel obstruction.
Magnitude Does Not Equal Severity
One of the most important clinical teaching points: the height of the lipase value does not predict the severity of pancreatitis. A patient with a lipase of 8,000 U/L (133× ULN) may have mild interstitial pancreatitis that resolves with fluids in 48 hours, while a patient with a lipase of 350 U/L (just over 3× ULN) may develop severe necrotizing pancreatitis. Severity is predicted by clinical scoring systems (BISAP, APACHE II, Ranson criteria) and by imaging findings, not by enzyme levels.
Lipase vs. Amylase: Which Test to Order
For decades, amylase was the default first test for suspected pancreatitis. That has changed. Current evidence strongly favors lipase as the primary — and in most cases, only — test needed.
Why Lipase Has Replaced Amylase
| Characteristic | Lipase | Amylase |
|---|---|---|
| Primary source | Pancreas (near-exclusive) | Pancreas + salivary glands + intestine |
| Rises after injury | 4–8 hours | 2–6 hours |
| Returns to normal | 8–14 days | 3–5 days |
| Sensitivity for acute pancreatitis | 82–100% | 67–83% |
| Specificity (at 3× ULN) | 82–100% | Lower (non-pancreatic sources) |
| Elevated in chronic alcoholic pancreatitis | May be falsely low (acinar atrophy) | Often falsely low (same reason) |
| Elevated in parotitis (mumps) | No | Yes (salivary amylase) |
When Amylase Still Has a Role
Amylase retains clinical value in limited scenarios:
- Macroamylasemia diagnosis: If amylase is elevated but lipase is normal, macroamylasemia (amylase bound to immunoglobulin, forming large complexes that clear slowly) is the likely explanation — a benign condition. Lipase is normal in macroamylasemia.
- Salivary gland disease: Parotitis (mumps, bacterial), anorexia nervosa (parotid hypertrophy), and Sjögren's syndrome elevate salivary amylase without affecting lipase.
- Post-ERCP monitoring: Both enzymes are routinely checked after endoscopic retrograde cholangiopancreatography.
Most major gastroenterology guidelines — including the American College of Gastroenterology (ACG) 2013 pancreatitis guidelines — recommend lipase alone and do not recommend routine simultaneous amylase testing for suspected acute pancreatitis.
Pancreatic Causes of Elevated Lipase
Acute Pancreatitis
The classic indication for lipase testing. Acute pancreatitis is the most common serious pancreatic disease, with approximately 300,000 hospitalizations per year in the United States. The two most common causes are:
- Gallstones (40–70% of cases): A gallstone temporarily obstructs the ampulla of Vater or the common bile duct, causing biliary and pancreatic ductal hypertension. The resulting backpressure triggers premature activation of pancreatic enzymes within acinar cells, causing autodigestion. Lipase elevation is typically brisk and very high.
- Alcohol (25–35% of cases): Chronic heavy alcohol use causes direct acinar toxicity through oxidative stress, lipid peroxidation, and mitochondrial dysfunction. An acute episode ("alcoholic pancreatitis") produces lipase elevations similar in magnitude to biliary pancreatitis. Notably, in chronic alcoholic pancreatitis with extensive acinar atrophy, lipase may not rise significantly even during an acute flare (see falsely normal section).
Less common causes of acute pancreatitis include hypertriglyceridemia (>1000 mg/dL), hypercalcemia, pancreatic divisum, autoimmune pancreatitis (IgG4-related), post-ERCP pancreatitis (PEP), trauma, medications (azathioprine, valproic acid, thiazides, GLP-1 receptor agonists, didanosine), and infections (mumps, coxsackievirus B, Ascaris).
Chronic Pancreatitis (Acute Exacerbation)
Chronic pancreatitis may produce lipase elevations during exacerbations, but the magnitude tends to be smaller than acute pancreatitis and may be misleadingly mild due to progressive loss of functional acinar mass. The diagnosis of chronic pancreatitis is primarily based on imaging (MRCP, CT showing ductal dilation, parenchymal atrophy, calcifications) and functional tests (fecal elastase-1), not lipase levels.
Pancreatic Cancer
Pancreatic ductal adenocarcinoma can cause mild-to-moderate lipase elevation, particularly when the tumor obstructs the main pancreatic duct. However, lipase is not a cancer screening test — CA 19-9 and CT/MRI are the primary diagnostic tools. Lipase elevation in a patient without a plausible trigger (no gallstones, no alcohol, no medication) warrants imaging to exclude a mass.
Post-ERCP Pancreatitis
Post-ERCP pancreatitis (PEP) is the most common serious complication of endoscopic retrograde cholangiopancreatography, occurring in 3–5% of cases (up to 15% in high-risk patients). Lipase is routinely measured 2–4 hours post-procedure; elevation ≥3× ULN with abdominal pain confirms PEP. Indomethacin rectal suppository pre-procedure reduces PEP risk by ~50% in high-risk patients (PMID: 22494121).
Non-Pancreatic Causes of Elevated Lipase
Lipase is more specific than amylase, but it is not perfectly pancreas-specific. Several non-pancreatic conditions can elevate lipase, occasionally to ≥3× ULN, which can lead to misdiagnosis if abdominal pain is also present.
Renal Failure
The kidneys are the primary clearance route for lipase. In acute kidney injury (AKI) and chronic kidney disease (CKD), reduced glomerular filtration leads to lipase accumulation in the blood. In ESRD, lipase may be chronically elevated up to 3× ULN even without pancreatic disease. This is a critical clinical pitfall: a patient with CKD stage 4–5 and abdominal pain may have a lipase of 200 U/L — technically exceeding the 3× ULN of 180 U/L — purely from reduced renal clearance, not pancreatitis. Imaging is essential in this population to avoid over-diagnosing pancreatitis.
Intestinal Diseases
- Small bowel obstruction and intestinal ischemia/infarction: Bowel wall breakdown releases intestinal lipase into the portal circulation. Elevations typically 2–5× ULN; rarely exceeds 10× ULN.
- Perforated peptic ulcer: Peritoneal irritation causes secondary pancreatic enzyme release; duodenal contents contacting the peritoneum can trigger mild lipase elevation.
- Celiac disease: Mild lipase elevation (generally <3× ULN) has been reported in untreated celiac disease, possibly from duodenal inflammation affecting pancreatic secretion regulation or secondary pancreatic involvement. Typically normalizes on a gluten-free diet.
Macrolipasemia
Analogous to macroamylasemia, macrolipasemia occurs when lipase forms large complexes with immunoglobulins (typically IgA or IgG). These high-molecular-weight complexes are not filtered by the kidney, leading to persistently elevated serum lipase. Macrolipasemia is benign — there is no underlying pancreatic pathology. It should be suspected when lipase is chronically elevated without clinical signs or imaging findings of pancreatic disease. Diagnosis is confirmed by ultracentrifugation of serum, which separates the macrocomplexes. No treatment is needed.
Medications
Several drug classes can directly injure the pancreas or cause lipase elevation through other mechanisms:
- Opiates (morphine, codeine): Cause sphincter of Oddi spasm, raising intraductal pressure. Lipase may rise 2–4× ULN within hours of an opioid dose — a common source of diagnostic confusion in hospitalized patients receiving opioid analgesia for abdominal pain.
- Azathioprine and 6-mercaptopurine: Can cause true drug-induced pancreatitis; the association is dose-independent and unpredictable (idiosyncratic).
- Statins: Rarely associated with pancreatitis (estimated incidence <1/10,000 patient-years). Case reports of lipase elevation with statin use exist, though causality is difficult to establish given the high prevalence of statin use.
- GLP-1 receptor agonists (semaglutide, liraglutide, exenatide): Post-marketing surveillance has identified cases of acute pancreatitis. Patients on these agents who develop abdominal pain should have lipase measured promptly; discontinuation is recommended if pancreatitis is confirmed.
- Valproic acid: Associated with drug-induced pancreatitis; particularly in pediatric patients.
- Thiazide diuretics: Classically associated with pancreatitis, possibly via hypertriglyceridemia or direct acinar toxicity; the association is weak in contemporary data.
When Lipase Is Falsely Normal
Just as important as recognizing elevated lipase is understanding when pancreatitis may be occurring despite a normal lipase value — a falsely reassuring result that can delay diagnosis.
Chronic Alcoholic Pancreatitis with Acinar Atrophy
The most clinically important cause of false-negative lipase. In patients with long-standing alcoholic pancreatitis, repeated bouts of inflammation cause progressive fibrosis and destruction of acinar cells — the very cells that produce lipase. When such a patient has an acute flare, there may be very little remaining acinar mass to release lipase into the blood. A lipase in the normal range or only marginally elevated (1–2× ULN) does not exclude acute exacerbation in a patient with known chronic pancreatitis and classic symptoms. MRI/MRCP or CT is the definitive diagnostic tool in this scenario.
Hypertriglyceridemia-Induced Pancreatitis
When serum triglycerides exceed approximately 1000 mg/dL (11.3 mmol/L), the hyperlipemic serum can interfere with enzyme-based lipase assays. The lipid-laden serum causes optical turbidity that falsely depresses colorimetric and turbidimetric lipase readings. A patient with triglyceride-induced acute pancreatitis — which can be severe — may have a paradoxically normal lipase on standard assay. When hypertriglyceridemia-induced pancreatitis is suspected (patient with known familial hypertriglyceridemia, diabetes, alcohol use, or uncontrolled hypothyroidism), the blood should be centrifuged to clear the chylomicrons, and a diluted sample assayed. The triglyceride level itself is diagnostic when >1000 mg/dL in the context of pancreatitis.
Delayed Presentation
If a patient waits more than 10–14 days from the onset of pancreatitis before presenting for evaluation, the lipase may have already returned to normal. Amylase normalizes even faster (3–5 days). In these late-presenting cases, CT/MRI showing pancreatic edema, fat stranding, or fluid collections may be the only diagnostic evidence available.
Pancreatitis Severity: Atlanta Classification and BISAP Score
Because lipase magnitude does not predict severity, standardized scoring systems are used to risk-stratify patients with confirmed acute pancreatitis. Two tools dominate current clinical practice.
Revised Atlanta Classification (2012)
The 2012 Revised Atlanta Classification (Banks et al., PMID: 22007898) defines three severity categories based on clinical course and complications:
- Mild acute pancreatitis: No organ failure, no local or systemic complications. Resolves within the first week. Represents ~80% of all cases. Management: IV fluids, pain control, early oral feeding when tolerated.
- Moderately severe acute pancreatitis: Transient organ failure (<48 hours) AND/OR local complications (fluid collections, pancreatic and/or peripancreatic necrosis) AND/OR exacerbation of co-morbid disease. Hospital stay typically 1–2 weeks.
- Severe acute pancreatitis: Persistent organ failure (>48 hours) — defined by the modified Marshall scoring system for respiratory (PaO2/FiO2 <300), renal (creatinine >1.9 mg/dL), or cardiovascular failure (systolic BP <90 mmHg not responding to fluids). Mortality 30–50%. ICU care required.
BISAP Score
The Bedside Index for Severity in Acute Pancreatitis (BISAP) is a simple 5-point scoring system calculated from data available within 24 hours of admission (Wu et al., PMID: 18312984):
- BUN >25 mg/dL (1 point)
- Impaired mental status / altered sensorium (1 point)
- SIRS — systemic inflammatory response syndrome (2+ of: HR >90, RR >20 or PaCO2 <32, temp >38°C or <36°C, WBC >12k or <4k) (1 point)
- Age >60 years (1 point)
- Pleural effusion on imaging (1 point)
Interpretation: Score 0–2 = low risk of mortality (<1%); Score 3–5 = high risk (mortality 7–22%). BISAP is a quick bedside tool, not a replacement for clinical judgment or CT severity index (CTSI).
CT Severity Index (Balthazar Score)
When CT is performed, the CT Severity Index (CTSI) grades both pancreatic inflammation (grades A–E) and the extent of necrosis (<30%, 30–50%, >50%), generating a composite score of 0–10. CTSI ≥7 correlates with significantly increased morbidity and mortality. Pancreatic necrosis — especially when infected — is the most feared local complication, managed by IV antibiotics (carbapenems) and, if failing medical therapy, minimally invasive necrosectomy.
Clinical Use: What Happens After a High Lipase Result
Understanding what comes next helps patients make sense of their diagnosis and the tests and treatments they will encounter.
Initial Workup When Lipase Is ≥3× ULN
When acute pancreatitis is confirmed or strongly suspected, standard initial workup includes:
- Right upper quadrant ultrasound: First-line imaging to look for gallstones or biliary dilation as the cause. Ultrasound does not visualize the pancreas well (obscured by bowel gas) but is quick and avoids radiation.
- Complete metabolic panel: ALT/AST (if significantly elevated — typically >3× ULN — gallstone pancreatitis is more likely); bilirubin; creatinine and BUN (renal function, BISAP score); calcium (hypercalcemia as a cause); glucose.
- Triglyceride level: Particularly if no gallstones and no alcohol history. Triglycerides >1000 mg/dL are diagnostic of hypertriglyceridemia-induced pancreatitis.
- CBC: WBC (SIRS criteria, infection surveillance); hematocrit (hemoconcentration predicts severe disease).
- CT abdomen/pelvis with contrast: Not required for initial diagnosis if clinical + lipase criteria are met, but obtained when diagnosis is uncertain, patient is not improving at 48–72 hours, or severity assessment is needed (CTSI).
Treatment Principles for Acute Pancreatitis
There is no specific antidote or medication that treats pancreatitis itself — management is supportive:
- Aggressive IV fluids: Lactated Ringer's (not normal saline — lower inflammatory response) at 250–500 mL/hour initially. Goal: urine output 0.5–1 mL/kg/hour. Fluid resuscitation in the first 12–24 hours is the most important intervention for preventing organ failure.
- Pain control: IV opioids (hydromorphone preferred over morphine — less sphincter of Oddi spasm); NSAIDs as adjunct if renal function allows.
- Early oral feeding: Start as soon as the patient can tolerate it (often within 24–48 hours). Low-fat, soft diet. Nothing-by-mouth status prolonged beyond clinical necessity worsens outcomes. Nasojejunal tube feeding is preferred over parenteral nutrition when oral intake is not possible for >72 hours.
- Gallstone pancreatitis: Cholecystectomy during the same hospitalization (or within 2–4 weeks) to prevent recurrence, which occurs in 30–50% of patients if the gallbladder is not removed. ERCP for stone clearance if choledocholithiasis is suspected (elevated bilirubin, dilated CBD on imaging).
- Alcohol-induced pancreatitis: Alcohol cessation counseling and referral; patients who continue drinking have a 50% recurrence rate and risk progression to chronic pancreatitis and pancreatic insufficiency.
Key Research and Citations
- Banks PA, Bollen TL, Dervenis C, et al.; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis — 2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. — Search PubMed
- Tenner S, Baillie J, DeWitt J, Vege SS; American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108(9):1400–1415. PMID: 23896955
- Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008;57(12):1698–1703. PMID: 18312984
- Lippi G, Valentino M, Cervellin G. Laboratory diagnosis of acute pancreatitis: in search of the Holy Grail. Crit Rev Clin Lab Sci. 2012;49(1):18–31. PMID: 22339380
- Mounzer R, Langmead CJ, Wu BU, et al. Comparison of existing clinical scoring systems to predict persistent organ failure in patients with acute pancreatitis. Gastroenterology. 2012;142(7):1476–1482. PMID: 22425589
- Phillip V, Steiner JM, Algül H. Early phase of acute pancreatitis: assessment and management. World J Gastrointest Pathophysiol. 2014;5(3):158–168. — Search PubMed
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144(6):1252–1261. PMID: 23622135
- Elmunzer BJ, Scheiman JM, Lehman GA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366(15):1414–1422. PMID: 22494121
- Petrov MS, Windsor JA. Classification of the severity of acute pancreatitis: how many categories make sense? Am J Gastroenterol. 2010;105(1):74–76. — Search PubMed
- Fortson MR, Freedman SN, Webster PD 3rd. Clinical assessment of hyperlipidemic pancreatitis. Am J Gastroenterol. 1995;90(12):2134–2139. — Search PubMed
- Smotkin J, Tenner S. Laboratory diagnostic tests in acute pancreatitis. J Clin Gastroenterol. 2002;34(4):459–462. PMID: 11907368
- Al-Bahrani AZ, Ammori BJ. Clinical laboratory assessment of acute pancreatitis. Clin Chim Acta. 2005;362(1–2):26–48. — Search PubMed
PubMed Search Links
- Serum lipase acute pancreatitis diagnosis
- Lipase vs. amylase pancreatitis sensitivity and specificity
- BISAP score acute pancreatitis severity prediction
- Hypertriglyceridemia-induced pancreatitis and lipase
- Macrolipasemia benign lipase elevation
Connections
- All Lab Tests
- Comprehensive Metabolic Panel
- Liver Function Tests
- Gamma-Glutamyl Transferase (GGT)
- Kidney Function Tests
- Inflammatory Markers Panel
- Lipid Panel
- Iron Panel
- Pancreatitis — the disease this test diagnoses: lipase ≥3× ULN plus epigastric pain meets the Atlanta criteria.