Fibrinogen Test — Plasma Fibrinogen and Coagulation
Fibrinogen is a large plasma glycoprotein synthesized by the liver that sits at the intersection of two major biological systems: coagulation, where it is converted to fibrin to form blood clots, and inflammation, where it rises 3- to 5-fold as an acute-phase reactant. The plasma fibrinogen test measures its concentration in citrated plasma and is essential for evaluating bleeding disorders, disseminated intravascular coagulation (DIC), liver synthetic function, and cardiovascular risk.
Table of Contents
- What Is Fibrinogen
- How the Test Is Performed
- Reference Ranges and Critical Values
- Fibrinogen in DIC and Hyperfibrinolysis
- Fibrinogen as an Acute-Phase Reactant
- Fibrinogen and Cardiovascular Risk
- Liver Disease and Fibrinogen
- Treatment: Fibrinogen Replacement
- Clinical Pearls for Interpretation
- References
- Featured Videos
What Is Fibrinogen
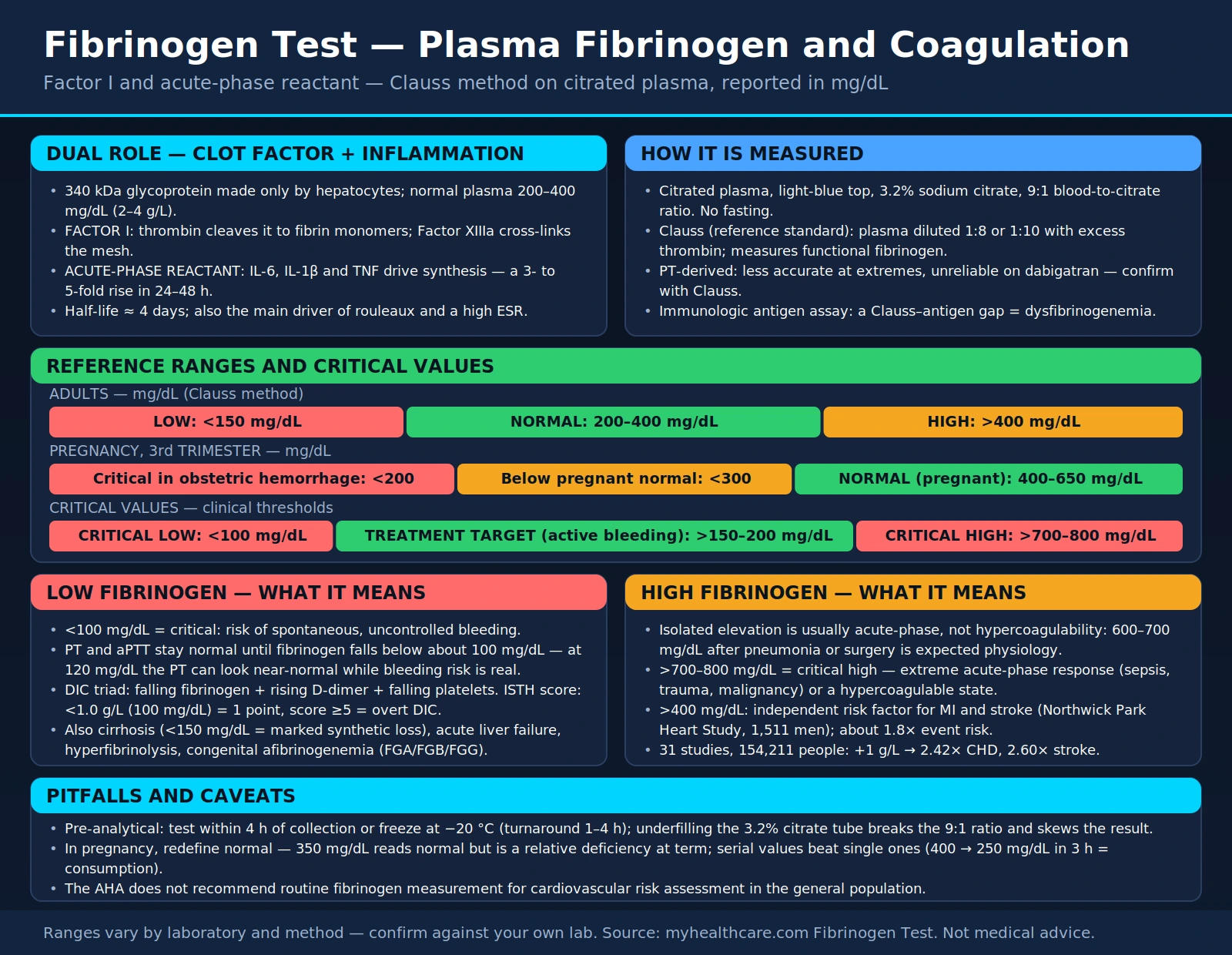
Fibrinogen is a large glycoprotein with a molecular weight of approximately 340 kDa, synthesized exclusively by hepatocytes in the liver. It circulates in plasma at a concentration of 200–400 mg/dL (2–4 g/L) and plays two distinct and critical physiological roles.
Fibrinogen as a coagulation factor (Factor I): When a vessel is injured, thrombin — generated through the coagulation cascade — cleaves fibrinogen into fibrin monomers. These monomers spontaneously polymerize into a fibrin mesh, which is then cross-linked and stabilized by Factor XIIIa (activated by thrombin) to form the definitive blood clot. Without adequate fibrinogen, clot formation is impossible regardless of the status of other coagulation factors.
Fibrinogen as an acute-phase reactant: The liver dramatically upregulates fibrinogen synthesis in response to inflammatory cytokines, particularly interleukin-6 (IL-6) and interleukin-1 beta (IL-1β). Within 24–48 hours of an inflammatory stimulus, plasma fibrinogen can rise 3- to 5-fold above baseline. This is the same mechanism that drives rouleaux formation of red blood cells and is the principal reason that fibrinogen is the dominant driver of an elevated ESR.
Conditions that reduce fibrinogen: Disseminated intravascular coagulation (DIC) consumes fibrinogen as it is incorporated into microthrombi throughout the vasculature. Severe liver disease impairs synthesis. Congenital afibrinogenemia (mutations in the FGA, FGB, or FGG genes encoding the three fibrinogen chains) causes complete absence of fibrinogen, leading to severe bleeding from birth. Hyperfibrinolysis degrades existing fibrinogen. Primary dysfibrinogenemia produces structurally abnormal fibrinogen that cannot form normal clots despite near-normal antigen levels.
Fibrinogen's dual role — as both a hemostatic protein and an inflammatory reactant — makes it one of the most informative single analytes in the clinical laboratory.
How the Test Is Performed
Fibrinogen is measured from citrated plasma using a light-blue-top tube containing 3.2% sodium citrate. The critical pre-analytical requirement is the correct 9:1 blood-to-citrate ratio — underfilling the tube dilutes the anticoagulant and produces falsely altered results. No fasting is required.
Clauss Method (Reference Standard)
The Clauss method is the most widely used and most accurate technique for measuring functional fibrinogen:
- Plasma is diluted (typically 1:8 or 1:10) and a large, standardized excess of thrombin is added
- Because thrombin is in vast excess, the clotting time depends only on fibrinogen concentration — more fibrinogen means a shorter clotting time
- The clotting time is read optically or mechanically and converted to a fibrinogen concentration using a reference calibration curve
- The Clauss method measures functional fibrinogen — fibrinogen that can actually be converted to fibrin — which is its key advantage
- In dysfibrinogenemia, Clauss fibrinogen will be lower than immunologic (antigen-based) fibrinogen, revealing the structural defect
PT-Derived Fibrinogen
- Calculated from the optical change in absorbance during a prothrombin time (PT) assay
- Less accurate than the Clauss method, particularly at extremes (very high or very low fibrinogen)
- Unreliable in patients receiving direct thrombin inhibitors such as dabigatran — the drug interferes with the clotting-based signal the calculation depends on, and the reported direction of the error varies by reagent and instrument. Use the Clauss method instead.
- Convenient as a screening estimate alongside a PT but should be confirmed with Clauss when clinical decisions depend on the result
Immunologic Assays
- Measure total fibrinogen antigen (functional + dysfunctional) by nephelometry, turbidimetry, or ELISA
- Useful for diagnosing dysfibrinogenemia when antigen is normal but Clauss is low
- Not appropriate as a routine functional test
Specimen stability: Fibrinogen is labile at room temperature. The sample should be tested within 4 hours of collection or frozen at −20°C for later analysis. Normal laboratory turnaround is 1–4 hours. Because no fasting is needed, the test can be drawn at any time of day.
Reference Ranges and Critical Values
Fibrinogen reference ranges vary modestly between laboratories, but the following values reflect widely accepted clinical thresholds:
Fibrinogen — Adults mg/dL (Clauss method)
Fibrinogen — Pregnancy (3rd Trimester) mg/dL
In obstetric hemorrhage a fibrinogen below 200 mg/dL is treated as critical — a higher threshold than the <100 mg/dL used outside pregnancy, because pregnancy raises the baseline so far that a "normal-looking" 250 mg/dL already represents a large fall.
Fibrinogen — Critical Values Clinical thresholds
Critical low (<100 mg/dL): Risk of spontaneous and uncontrolled bleeding. The PT and aPTT begin to prolong at fibrinogen concentrations below approximately 100 mg/dL. Immediate clinical assessment and likely fibrinogen replacement are warranted.
DIC laboratory pattern: The classic triad of DIC is: falling fibrinogen + rising D-dimer + falling platelet count, accompanied by prolonged PT and aPTT. Fibrinogen <100 mg/dL in this context represents life-threatening consumptive coagulopathy.
Critical high (>700–800 mg/dL): Indicates an extreme acute-phase response (sepsis, major trauma, malignancy) or a hypercoagulable state. Very high fibrinogen is associated with thromboembolic risk.
Cardiovascular risk threshold: Multiple epidemiological studies, including the landmark Northwick Park Heart Study, identified fibrinogen >400 mg/dL as an independent risk factor for myocardial infarction and stroke.
Fibrinogen in DIC and Hyperfibrinolysis
Disseminated intravascular coagulation (DIC) and primary hyperfibrinolysis are the two conditions where falling fibrinogen is most acutely life-threatening and where measurement is most urgently needed.
Disseminated Intravascular Coagulation
DIC is a syndrome of widespread pathological activation of the coagulation system, triggered by underlying conditions including sepsis, major trauma, obstetric emergencies, and malignancy. Fibrinogen falls because it is continuously consumed as microthrombi form throughout the microvasculature. As clotting factors are exhausted, the patient simultaneously develops microvascular thrombosis (organ damage) and clinical bleeding (consumption of hemostatic proteins).
- ISTH DIC scoring system: Platelet count, fibrinogen, PT prolongation, and D-dimer are combined into a score; fibrinogen <1.0 g/L (100 mg/dL) = 1 point; a score ≥5 is consistent with overt DIC
- Fibrinogen falls after D-dimer rises — D-dimer is a more sensitive early marker of DIC; fibrinogen falling signals advanced disease
- Serial measurements every 4–6 hours in acutely ill patients are more informative than a single value
- DIC management targets the underlying cause; fibrinogen replacement (cryoprecipitate or fibrinogen concentrate) targets fibrinogen <100–150 mg/dL with active bleeding
Obstetric DIC
Placental abruption and amniotic fluid embolism are classic triggers for rapid obstetric DIC. Because pregnant fibrinogen is physiologically elevated (450–600 mg/dL at term), a fibrinogen value of 300–350 mg/dL — which would be "normal" in a non-pregnant patient — represents significant fibrinogen depletion in an obstetric emergency. A fibrinogen <200 mg/dL in the obstetric setting predicts postpartum hemorrhage severity with high accuracy (Collins et al., PMID 24810606).
Congenital Fibrinogen Disorders
- Congenital afibrinogenemia: Complete absence of fibrinogen; autosomal recessive mutations in the FGA, FGB, or FGG genes; presents with severe umbilical bleeding at birth, intracranial hemorrhage risk; treated with fibrinogen concentrate or cryoprecipitate prophylactically
- Hypofibrinogenemia: Partial deficiency; bleeding tendency proportional to fibrinogen level
- Dysfibrinogenemia: Normal or near-normal fibrinogen antigen with reduced functional (Clauss) fibrinogen; can cause either bleeding or thrombosis depending on the molecular defect; diagnosed by discordance between Clauss and immunologic fibrinogen assays
Primary Hyperfibrinolysis
In primary hyperfibrinolysis — caused by excess plasminogen activators (tPA, urokinase) — plasmin degrades both fibrin clots and circulating fibrinogen directly. Unlike DIC, platelets are not consumed, and the euglobulin lysis time is shortened. Alpha-2-antiplasmin levels fall. D-dimer is elevated in both DIC and hyperfibrinolysis; distinguishing them requires the full clinical picture and ancillary tests. Antifibrinolytic therapy with tranexamic acid is effective in primary hyperfibrinolysis.
Fibrinogen as an Acute-Phase Reactant and Inflammatory Marker
The liver's acute-phase response to infection, tissue injury, or autoimmune activation involves dramatic changes in plasma protein synthesis. Fibrinogen is one of the major positive acute-phase reactants — proteins whose synthesis increases during inflammation.
Cytokine regulation: IL-6 is the primary driver of fibrinogen upregulation in the liver. IL-1β and tumor necrosis factor (TNF) contribute. The fibrinogen response is slower than CRP (which rises within 4–6 hours) because fibrinogen has a longer synthesis induction lag and a plasma half-life of approximately 4 days. Fibrinogen typically begins rising 24–48 hours after inflammation onset and takes days to weeks to normalize after resolution.
Connection to ESR: Fibrinogen is the principal plasma protein responsible for rouleaux formation — the stacking of red blood cells that causes them to sediment rapidly in the Westergren tube. The ESR is therefore largely a surrogate measure of fibrinogen (and other high-molecular-weight proteins like fibronectin and immunoglobulins). This explains why fibrinogen and ESR track together in inflammatory diseases and why the ESR lags similarly behind inflammatory events.
Clinical conditions associated with elevated fibrinogen:
- Acute infections (bacterial, viral, fungal) — fibrinogen rises within 24–48 hours
- Rheumatoid arthritis and other inflammatory arthropathies
- Inflammatory bowel disease (Crohn's disease, ulcerative colitis)
- Malignancy — fibrinogen is elevated in many cancers and may reflect tumor-driven inflammation
- Myocardial infarction — fibrinogen rises acutely and remains elevated during the post-MI inflammatory period
- Major trauma and post-surgical states
- Diabetes mellitus — chronically elevated fibrinogen as part of low-grade systemic inflammation
- Acute COVID-19 — fibrinogen rose markedly in severe COVID-19 and correlated with pulmonary microthrombus formation (Simurda et al., PMID 33525398)
- Pregnancy — fibrinogen rises 50–100% above baseline to support hemostasis at delivery; a fibrinogen of 350 mg/dL that appears normal by standard reference ranges may actually represent relative deficiency in a pregnant patient at term
Because fibrinogen rises substantially with age, smoking, obesity, and sedentary lifestyle — all independent cardiovascular risk factors — interpreting fibrinogen in context of these variables is essential.
Fibrinogen and Cardiovascular Risk
Fibrinogen occupies a unique position in cardiovascular medicine: it is both a mechanistic contributor to atherothrombosis and an independent epidemiological risk factor for myocardial infarction and stroke.
Mechanistic Role
Fibrinogen contributes to atherothrombosis through several mechanisms:
- Promotes platelet aggregation by binding to glycoprotein IIb/IIIa receptors on activated platelets (fibrinogen acts as a molecular bridge between adjacent platelets)
- Increases plasma viscosity, raising shear stress on vessel walls and contributing to endothelial dysfunction
- Promotes rouleaux formation, impairing red blood cell flow through small vessels
- Incorporates into atherosclerotic plaques, where fibrin deposition contributes to plaque stability and instability
- Stimulates smooth muscle cell proliferation and migration — a key step in atherogenesis
Epidemiological Evidence
- Northwick Park Heart Study (1986): Meade et al. followed 1,511 men aged 40–64 for 5 years; fibrinogen was a stronger predictor of ischemic heart disease events than cholesterol, particularly in men over 55 (PMID 2874872)
- Fibrinogen Studies Collaboration meta-analysis (JAMA 2005): Pooled data from 31 prospective studies (154,211 participants); each 1 g/L increment in fibrinogen was associated with a 2.42-fold increase in coronary heart disease risk and a 2.60-fold increase in stroke risk after adjustment for conventional risk factors (PMID 16219884)
- Fibrinogen >400 mg/dL is associated with an approximately 1.8-fold increased risk of cardiovascular events
Lifestyle and Treatment Effects on Fibrinogen
- Smoking: Increases fibrinogen by 10–15% — one of the most powerful modifiable determinants; smoking cessation reduces fibrinogen within weeks to months
- Obesity: Adipose tissue produces IL-6, directly stimulating hepatic fibrinogen synthesis; weight loss reduces fibrinogen
- Exercise: Regular aerobic exercise reduces fibrinogen by 5–10%
- Statins: Modestly reduce fibrinogen by approximately 9% independent of their lipid-lowering effect
- Omega-3 fatty acids: Reduce fibrinogen at doses of ≥3 g/day
- Fibrates: Gemfibrozil and bezafibrate reduce fibrinogen 20–30% — their cardioprotective effect may partly be mediated through fibrinogen reduction
Clinical Guidance
The American Heart Association (AHA) does not recommend routine fibrinogen measurement for cardiovascular risk assessment in the general population, citing insufficient evidence that knowing the fibrinogen level changes treatment decisions beyond what standard risk factors provide. However, fibrinogen measurement is clinically appropriate in patients with borderline cardiovascular risk where an additional marker might tip the balance toward statin initiation, or in patients with metabolic syndrome, diabetes, or strong family history where inflammation-driven risk is suspected.
Liver Disease and Fibrinogen
Because fibrinogen is synthesized exclusively by hepatocytes, plasma fibrinogen is a direct reflection of hepatic synthetic capacity. In progressive liver disease, fibrinogen falls as functional liver mass declines.
Fibrinogen in Cirrhosis
- Fibrinogen falls as cirrhosis progresses; levels <150 mg/dL indicate significant impairment of synthetic function
- Fibrinogen may be more sensitive than PT/INR for detecting early synthetic dysfunction because PT is also affected by vitamin K deficiency — which is common in cirrhosis but does not reflect hepatocyte loss
- Cirrhotic patients are not simply "auto-anticoagulated"; thromboembolic events are common in cirrhosis because pro-coagulant factors (fibrinogen, Factor VIII, vWF) are also disproportionately affected differently than anti-coagulant factors (protein C, protein S, antithrombin)
Acute Liver Failure
In acute liver failure (ALF), fibrinogen can fall precipitously as hepatocyte mass is lost. DIC may co-exist with impaired synthesis, making management complex. A fibrinogen <100 mg/dL in ALF represents a critical emergency — replacement therapy and urgent evaluation for liver transplantation are warranted.
Pre-Procedural Assessment
- Fibrinogen should be measured before liver biopsy, paracentesis, or other invasive procedures in cirrhotic patients
- Thromboelastography (TEG) or rotational thromboelastometry (ROTEM) provide better functional guidance for procedural bleeding risk in cirrhotics than individual factor levels, because they assess the integrated clotting process including fibrinogen's contribution to clot strength (PMID 25316089)
- ROTEM FIBTEM amplitude directly quantifies fibrin-based clot strength, guiding fibrinogen replacement in complex coagulopathy
Liver Transplantation
Fibrinogen is part of the standard pre-transplant coagulation workup. During the anhepatic phase of transplant surgery, fibrinogen synthesis ceases entirely; massive transfusion and fibrinogen concentrate are core components of intraoperative management in liver transplantation (PMID 22825929).
Treatment: Fibrinogen Replacement
When fibrinogen falls below critical thresholds in a bleeding patient, replacement therapy restores hemostatic capacity. Two product types are available.
Cryoprecipitate
- Prepared by slowly thawing fresh frozen plasma at 1–6°C and collecting the precipitate
- Each unit contains 200–300 mg of fibrinogen, plus Factor VIII, von Willebrand factor (vWF), Factor XIII, and fibronectin
- Standard adult dose: 10 units of pooled cryoprecipitate; expected fibrinogen increment: 50–75 mg/dL
- Pooled product from multiple donors — associated with small but measurable transfusion-transmitted infection risk
- Must be ABO-compatible (preferred; not strictly required for fibrinogen content)
- Useful in DIC, massive hemorrhage, and acquired hypofibrinogenemia
Fibrinogen Concentrate
- Commercial lyophilized fibrinogen (RiaSTAP, Haemocomplettan P) derived from pooled human plasma with viral inactivation
- Dose for congenital afibrinogenemia: 70 mg/kg body weight; titrated by fibrinogen level in acquired deficiency
- More precise dosing than cryoprecipitate (known fibrinogen content per vial), lower volume load, faster reconstitution, pathogen-reduced
- Increasingly used in obstetric hemorrhage and cardiac surgery coagulopathy where rapid, precise fibrinogen repletion is critical (PMID 28130843)
Dosing Targets
- Active bleeding (general): target fibrinogen >150–200 mg/dL
- Active obstetric hemorrhage: target >200 mg/dL (some guidelines recommend >250 mg/dL)
- Congenital afibrinogenemia: target >100 mg/dL for prophylaxis; >200 mg/dL for major bleeding or surgery
- Cardiac surgery: target fibrinogen >200 mg/dL intraoperatively to prevent microvascular oozing
Adjunctive Antifibrinolytic Therapy
Tranexamic acid (TXA) inhibits plasmin-mediated fibrin degradation and is used alongside fibrinogen replacement in major hemorrhage to prevent clot dissolution. TXA does not replace fibrinogen but prevents loss of existing fibrin. In primary hyperfibrinolysis, TXA may be the primary treatment even when fibrinogen replacement is also needed.
Clinical Pearls for Fibrinogen Interpretation
Fibrinogen is most informative when interpreted alongside the full coagulation panel. The following pearls help avoid the most common clinical pitfalls:
- Always interpret fibrinogen in concert with platelet count, PT, aPTT, and D-dimer. An isolated fibrinogen abnormality has a different differential diagnosis than a fibrinogen fall occurring simultaneously with rising D-dimer, prolonging PT, and falling platelets — the latter is DIC until proven otherwise.
- Isolated fibrinogen elevation = likely acute-phase reaction, not clotting problem. A fibrinogen of 600–700 mg/dL in a patient with pneumonia or recent surgery is expected physiology; it does not indicate hypercoagulability requiring treatment in isolation.
- In pregnancy, redefine "normal." A fibrinogen of 300–400 mg/dL is normal in a non-pregnant adult but represents relative deficiency at term when normal is 450–600 mg/dL. Apply pregnancy-specific reference ranges.
- Serial fibrinogen is more informative than a single value. In a patient with sepsis or obstetric emergency, a fibrinogen of 250 mg/dL drawn three hours after a prior value of 400 mg/dL signals rapid consumption — the trend matters as much as the absolute number.
- Clauss vs. PT-derived fibrinogen in patients on direct thrombin inhibitors (dabigatran): Dabigatran interferes with PT-based clotting assays, so a PT-derived fibrinogen cannot be trusted in a patient taking it; the direction of the error depends on the reagent and analyser, which is why no single correction factor is offered. Always use the Clauss method in patients receiving direct thrombin inhibitors.
- Dysfibrinogenemia: look for Clauss-antigen discordance. When the clinical picture suggests a congenital coagulopathy and PT/aPTT are mildly prolonged with normal platelet count, compare Clauss fibrinogen (functional) to immunologic fibrinogen (antigen). A 20–30% discordance suggests dysfibrinogenemia.
- Very high fibrinogen (>700 mg/dL) in critically ill patients signals an extreme inflammatory response. Although elevated fibrinogen itself is not treated, very high fibrinogen may indicate the need for aggressive treatment of the underlying inflammatory or infectious process.
- PT/aPTT prolong late in fibrinogen deficiency. Both PT and aPTT remain normal until fibrinogen falls below approximately 100 mg/dL. A patient with fibrinogen of 120 mg/dL may have a near-normal PT while still being at significant bleeding risk — fibrinogen level is the more sensitive measure at these intermediate values.
References
Selected PubMed citations and searches for fibrinogen and coagulation:
- Meade TW et al. Haemostatic function and ischaemic heart disease: principal results of the Northwick Park Heart Study. Lancet. 1986;2(8506):533–7. — Search PubMed
- Danesh J et al. Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. JAMA. 2005;294(14):1799–809. PMID 16219884
- Levi M, van der Poll T. Disseminated intravascular coagulation: a review for the internist. Intern Emerg Med. 2013;8(1):23–32. — Search PubMed
- Toh CH et al. The ISTH DIC scoring system — a 5-year retrospective analysis of 2500 patients. Thromb Haemost. 2009;101(3):553–8. — Search PubMed
- Machlus KR, Colby EA. Fibrinogen in inflammation and cardiovascular disease. Arterioscler Thromb Vasc Biol. 2011;31(12):2751–6. PMID 22096095
- Ranucci M et al. Fibrinogen supplementation in cardiac surgery: where are we now and where are we going? Semin Cardiothorac Vasc Anesth. 2012;16(4):221–9. — Search PubMed
- Wikkelsøe AJ et al. Fibrinogen concentrate as first-line haemostatic therapy in major haemorrhage: a systematic review and meta-analysis. J Thromb Haemost. 2017;15(5):823–833. — Search PubMed
- Peyvandi F et al. Congenital disorders of fibrinogen. Haemophilia. 2011;17 Suppl 3:6–13. — Search PubMed
- Franchini M et al. Thromboelastography: a clinical review. Semin Thromb Hemost. 2014;40(8):873–80. — Search PubMed
- Simurda T et al. Fibrinogen in COVID-19 coagulopathy: revisiting Virchow's triad in SARS-CoV-2 infection. J Clin Med. 2021;10(3):454. — Search PubMed
- Collins PW et al. Fibrinogen is independently associated with the risk of severe primary postpartum haemorrhage. Br J Haematol. 2014;166(4):518–26. — Search PubMed
- Spiezia L et al. Fibrinogen in obstetrics, malignancy and inflammatory conditions. Semin Thromb Hemost. 2016;42(6):631–637. — Search PubMed
Fibrinogen coagulation clinical laboratory — PubMed search
Plasma fibrinogen DIC disseminated intravascular coagulation — PubMed search