PT/INR Test: Prothrombin Time and International Normalized Ratio
The Prothrombin Time (PT) measures how quickly blood clots through the extrinsic coagulation pathway — the route initiated by tissue factor after vessel injury. The International Normalized Ratio (INR) is a standardized calculation derived from the PT that corrects for differences in laboratory reagents, making warfarin monitoring consistent across institutions. Together, PT and INR are among the most frequently ordered coagulation tests in clinical medicine, serving triple duty: monitoring anticoagulant therapy, evaluating liver synthetic function, and assessing bleeding risk before procedures.
Table of Contents
- Overview — Extrinsic Coagulation Pathway
- How PT and INR Are Measured
- Normal and Therapeutic Ranges
- Pre-Procedure INR Thresholds
- Warfarin Therapy and INR Monitoring
- PT as a Liver Function Test
- Vitamin K and PT/INR
- Factor V Leiden and Coagulation Genetics
- Point-of-Care INR Testing
- Causes of Prolonged PT/INR
- aPTT: The Intrinsic Pathway Partner Test
- Urgent Reversal Strategies
- Key Research and Citations
- Connections
- Featured Videos
Overview — Extrinsic Coagulation Pathway
The extrinsic pathway is triggered when tissue factor (TF, Factor III) — normally expressed only on subendothelial cells — is exposed to circulating blood after vessel injury. TF binds Factor VII to form the TF-VIIa complex, which activates Factor X and Factor IX. Factor Xa, together with its essential cofactor Factor Va, assembles into the prothrombinase complex on the surface of activated platelets and phospholipid membranes. This complex converts prothrombin (Factor II) to thrombin at a rate approximately 300,000 times faster than Factor Xa alone. Thrombin then cleaves fibrinogen to fibrin monomers, which polymerize end-to-end and side-to-side, forming a loose gel. Factor XIII, also activated by thrombin, cross-links the fibrin polymers covalently, creating the stable, mechanically robust clot that anchors the platelet plug.
The PT measures this entire extrinsic and common pathway in a single number. A prolonged PT means clot formation is slower than normal, reflecting reduced activity of one or more factors in this chain. Because Factors I (fibrinogen), II (prothrombin), V, VII, and X are all synthesized exclusively in the liver, the PT is an exquisitely sensitive window into hepatic synthetic function. Additionally, Factors II (prothrombin), VII, IX, and X require vitamin K for the final post-translational step of gamma-carboxylation of glutamate residues. Without this modification, these proteins cannot bind calcium or phospholipid membranes effectively, making them functionally inert as coagulation factors. This dual sensitivity — to liver disease and to vitamin K status — gives the PT its broad clinical utility far beyond simple anticoagulation monitoring.
Factors Measured by the PT
The name "prothrombin time" is historically a misnomer — the test does not measure prothrombin (Factor II) in isolation. It reports the combined activity of the extrinsic-pathway factor (VII) and every factor of the common pathway (X, V, II, and fibrinogen/Factor I). A deficiency anywhere along that chain prolongs the result:
- Factor VII: Vitamin K-dependent serine protease; the only factor unique to the extrinsic pathway. Shortest half-life of all the coagulation factors, which is why it is the first to fall in warfarin therapy or vitamin K deficiency and why the PT is the earliest laboratory sign of impaired factor synthesis or carboxylation.
- Factor X: Vitamin K-dependent. The convergence point of the extrinsic and intrinsic pathways; as Factor Xa it converts prothrombin to thrombin.
- Factor V: A non-vitamin K-dependent cofactor known as the "labile factor" because it degrades rapidly in stored plasma — one reason delayed specimen processing spuriously prolongs the PT. It is reduced in liver failure, and because it is not vitamin K-dependent, its level distinguishes synthetic failure from vitamin K deficiency. The Factor V Leiden mutation is a thrombophilia, not a bleeding disorder, and does not prolong the PT.
- Factor II (prothrombin): Vitamin K-dependent. Converted to thrombin, the pivotal enzyme that cleaves fibrinogen to fibrin, activates platelets, and amplifies the cascade through positive feedback.
- Factor I (fibrinogen): The substrate thrombin converts to fibrin. A fibrinogen below roughly 100 mg/dL prolongs the PT on its own. The two dominant causes of low fibrinogen are consumption (DIC) and synthetic failure (advanced liver disease).
Understanding the extrinsic pathway also clarifies why Factor VII deficiency or depletion produces an isolated PT prolongation. Factor VII is unique to the extrinsic pathway; all other factors downstream (X, V, II, fibrinogen) are shared with the intrinsic pathway. The aPTT (activated partial thromboplastin time), which measures the intrinsic pathway, remains normal when only Factor VII is affected. Conversely, the PT and aPTT both prolong when common pathway factors (X, V, II, or fibrinogen) are depleted, as occurs in severe liver failure or disseminated intravascular coagulation (DIC).
The cascade model of coagulation described above — extrinsic, intrinsic, and common pathways — is useful for interpreting laboratory tests, but it is a simplification of in vivo hemostasis. The cell-based model of coagulation recognizes that tissue factor bearing cells initiate clotting, platelets amplify it, and propagation occurs on the platelet surface. However, the cascade model remains the framework for understanding PT and aPTT results clinically.
How PT and INR Are Measured
The prothrombin time was described by the American physician Armand Quick in 1935, in the same period that heparin was being developed for clinical anticoagulant use. Quick's original method — recalcify citrated plasma in the presence of a tissue extract and time the appearance of a clot — is, in principle, the method still in use today. Nearly a century of refinement has changed the reagents and the clot-detection hardware, not the underlying logic of the assay.
Blood is drawn into a blue-top tube containing sodium citrate (buffered 3.2% sodium citrate). Citrate is an anticoagulant that chelates free calcium ions, halting the coagulation cascade in the tube. The ratio of blood to citrate is critical — the standard ratio is 9:1 (blood:citrate). If the tube is underfilled, excess citrate relative to plasma causes falsely prolonged results; if the tube is overfilled or the patient has severe polycythemia (elevated hematocrit), the citrate concentration is relatively low. In patients with a hematocrit above 55%, the laboratory must use a corrected citrate volume, or the PT will be spuriously shortened.
In the laboratory, the citrated plasma is separated by centrifugation. The PT assay then proceeds in three steps: (1) the plasma is warmed to 37°C; (2) calcium chloride is added to overcome the citrate chelation; (3) thromboplastin — a mixture of human or recombinant tissue factor, phospholipid, and calcium — is added. The stopwatch starts. The time from thromboplastin addition to clot detection (via optical or electromechanical methods) is the PT in seconds.
The INR was introduced by the World Health Organization in 1983 to solve a persistent and dangerous problem: thromboplastin reagents from different manufacturers had wildly different sensitivities to Factor VII depletion. Early rabbit-brain thromboplastins were less sensitive than later human placental or recombinant preparations. A patient anticoagulated at exactly the same therapeutic level might have a PT of 18 seconds at one hospital using a sensitive reagent and 26 seconds at another hospital using an insensitive reagent. Clinicians using raw PT seconds to titrate warfarin were inadvertently over- or under-anticoagulating patients depending on which hospital they used.
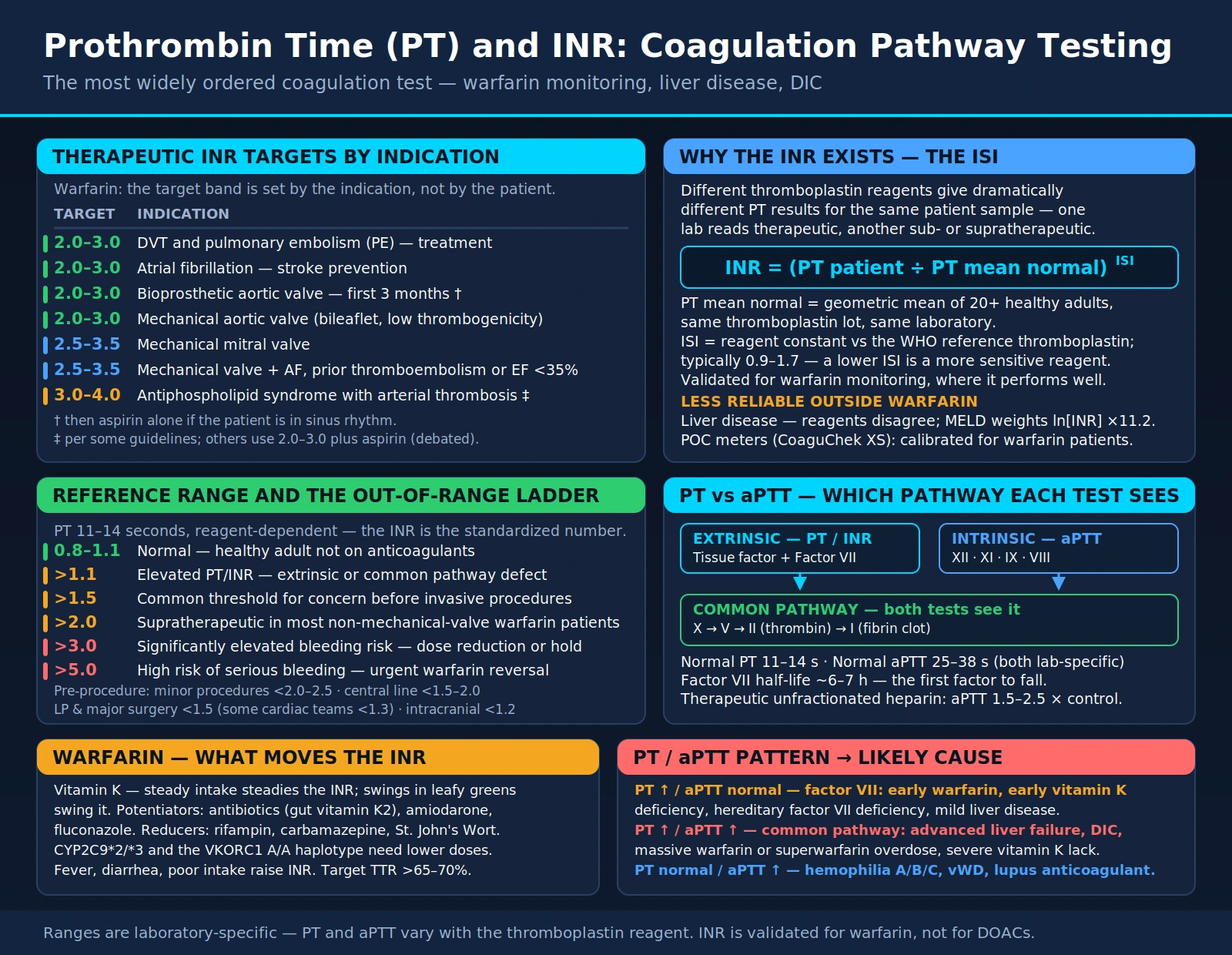
The INR solves this by incorporating the International Sensitivity Index (ISI) assigned to each lot of thromboplastin reagent by the manufacturer through calibration against a WHO international reference preparation. The formula is: INR = (Patient PT ÷ Mean Normal PT)ISI. The Mean Normal PT (MNPT) is the geometric mean PT of at least 20 healthy adult volunteers run on the same instrument with the same reagent lot. A perfectly calibrated assay with an ISI of 1.0 yields an INR numerically equal to the raw PT ratio. The lower the ISI, the more sensitive the reagent and the less exponential correction the formula has to apply. Modern recombinant thromboplastin reagents typically have ISI values between 0.9 and 1.1, making INR and PT ratio nearly equivalent. Older rabbit-brain reagents had ISI values as high as 2.8, which required substantial correction.
Two limitations of the INR are worth stating plainly, because they are routinely overlooked. First, the INR was derived and validated for one purpose — monitoring vitamin K antagonist therapy in patients whose livers work — and it performs reliably only in that context. Second, the INR is not a bleeding-risk meter. It is a clotting-speed measurement that happens to correlate with bleeding risk in warfarin-treated patients, and that correlation does not transfer to liver disease, DIC, or direct oral anticoagulants.
Point-of-care analyzers (whole blood finger-prick devices) use dry reagent strips and electrochemical clot detection. They calculate INR using a device-specific ISI. Multiple studies have shown strong correlation with laboratory INR (Pearson r > 0.97, mean bias typically under 0.2 INR units), sufficient for clinical management. However, they should not be used to diagnose coagulopathies other than warfarin effect, and results in patients with lupus anticoagulant or extreme polycythemia/anemia may be unreliable.
Normal and Therapeutic Ranges
Reference ranges vary slightly between laboratories, but widely accepted values are:
- PT (seconds): 11–13.5 seconds (laboratory-specific; always compare to the lab's stated reference range)
- INR (baseline, not on anticoagulation): 0.8–1.2
Therapeutic INR targets by indication (per ACCP, ACC/AHA, and ASH guidelines):
- Atrial fibrillation (non-valvular): INR 2.0–3.0 (though DOACs are now preferred for most patients)
- Deep vein thrombosis (DVT) treatment: INR 2.0–3.0
- Pulmonary embolism (PE) treatment: INR 2.0–3.0
- Bioprosthetic heart valve: INR 2.0–3.0 for the first 3 months post-implant; may discontinue or shift to aspirin thereafter
- Mechanical aortic valve (bileaflet, no additional risk factors): INR 2.0–3.0 (ACC/AHA 2014)
- Mechanical mitral valve: INR 2.5–3.5
- Mechanical aortic valve with additional risk factors (AF, prior thromboembolism, LV dysfunction, hypercoagulable state): INR 2.5–3.5
- Antiphospholipid syndrome with prior arterial thrombosis: INR 3.0–4.0 (some guidelines 2.0–3.0 with aspirin)
INR values above the therapeutic range carry progressively increasing bleeding risk:
- INR 3.0–4.0: Elevated bleeding risk; review interacting medications and dietary vitamin K; consider dose reduction of 10–15%
- INR 4.0–5.0: Hold next 1–2 warfarin doses; recheck in 2–3 days; no vitamin K needed unless bleeding
- INR 5.0–9.0: Hold warfarin; give oral vitamin K 1–2.5 mg (lowers INR within 24 hours); recheck next day
- INR > 9.0 without bleeding: Hold warfarin; oral vitamin K 2.5–5 mg; recheck in 24 hours
- INR > 9.0 with serious bleeding (intracranial, GI, retroperitoneal): Emergent reversal with 4-factor prothrombin complex concentrate (4F-PCC; Kcentra) — faster and more predictable than fresh frozen plasma (FFP); supplement with IV vitamin K 5–10 mg; target INR < 1.5 for surgical intervention
A useful clinical heuristic: the risk of clinically significant bleeding roughly doubles for each 0.5-unit rise in INR above 3.0 in patients on warfarin. An INR of 6.0 confers approximately 8-fold higher bleeding risk compared to a therapeutic INR of 2.5.
Pre-Procedure INR Thresholds
An INR above 1.5 is the threshold most commonly cited as a reason to pause before an invasive procedure. It is a convention rather than a validated cut-off: the actual bleeding risk depends far more on the procedure than on the number. A liver biopsy, a spinal anesthetic, and a cardiac catheterization each place a different premium on hemostasis, and the evidence linking a mildly abnormal coagulation screen to actual procedural bleeding is thinner than the ubiquity of the 1.5 threshold suggests (Segal and Dzik reviewed this literature in 2005 and found remarkably little of it).
With that caveat, the thresholds in general institutional use are:
- Minor procedures (skin biopsy, dental extraction): INR below 2.0–2.5 is generally acceptable; procedure-specific guidance often permits higher, and dental extractions in particular are usually safe at a full therapeutic INR with local hemostatic measures
- Central venous catheter placement: INR below 1.5–2.0 per most institutional protocols
- Lumbar puncture and spinal or epidural procedures: INR below 1.5 (ASRA guideline)
- Major surgery: INR below 1.5; some cardiac surgical teams require below 1.3
- Intracranial surgery: INR as close to normal as possible — many neurosurgeons target below 1.2
Two further orientation points on the scale: an INR above 2.0 is supratherapeutic for most warfarin patients who do not have a mechanical valve, and an INR above 5.0 carries a high risk of serious spontaneous bleeding and warrants urgent reversal (see Urgent Reversal Strategies).
Warfarin Therapy and INR Monitoring
Warfarin (Coumadin) has been the mainstay of oral anticoagulation for over six decades. It acts by inhibiting vitamin K epoxide reductase complex subunit 1 (VKORC1), the enzyme that recycles oxidized vitamin K epoxide back to its active reduced (hydroquinone) form. Without active vitamin K, the gamma-carboxylation of glutamic acid residues on Factors II, VII, IX, and X (as well as the anticoagulant proteins C and S) is blocked. These under-carboxylated proteins are called PIVKA (Proteins Induced by Vitamin K Absence or Antagonism) and are functionally inactive in the coagulation cascade.
The onset and offset of warfarin anticoagulation are governed by the half-lives of the affected coagulation factors:
- Factor VII: 4–6 hours — this is why the PT/INR rises quickly when warfarin is started (within 24–36 hours of the first dose) even before full anticoagulation is achieved
- Protein C: ~8 hours — depletion of this natural anticoagulant precedes depletion of prothrombin in the first 48–72 hours, creating a transient prothrombotic state ("warfarin-induced skin necrosis" in patients with underlying protein C deficiency)
- Factor IX: 24 hours
- Factor X: 36–48 hours
- Prothrombin (Factor II): 60–72 hours — full anticoagulation is not achieved until prothrombin levels fall; this takes 4–5 days of warfarin dosing
This dissociation between early INR rise (driven by Factor VII depletion) and true anticoagulation (requiring prothrombin depletion) is why bridging with a parenteral anticoagulant (heparin or LMWH) was historically used when initiating warfarin for acute DVT or PE. Current guidelines (ACCP 2016) no longer routinely recommend heparin bridging for non-valvular AF in patients starting or temporarily stopping warfarin.
Drug interactions with warfarin are extensive and clinically important. Warfarin is predominantly metabolized by CYP2C9 (S-warfarin, the more potent enantiomer) and CYP3A4 (R-warfarin). Inhibitors of these enzymes increase warfarin exposure and raise the INR:
- Azole antifungals (fluconazole, voriconazole) — potent CYP2C9 inhibitors; can raise INR dramatically
- Amiodarone — inhibits both CYP2C9 and CYP3A4; dose reduction of 30–50% often needed
- Metronidazole (Flagyl) — inhibits CYP2C9; even a 7-day course requires INR monitoring
- Broad-spectrum antibiotics (fluoroquinolones, cephalosporins) — reduce gut flora synthesis of vitamin K2; may raise INR by 0.5–1.0 units
- NSAIDs and aspirin — do not elevate INR but dramatically increase bleeding risk by impairing platelet function and irritating GI mucosa
Inducers of CYP enzymes reduce warfarin effect and lower the INR:
- Rifampin (rifampicin) — the most potent inducer; can completely nullify warfarin anticoagulation; double or triple dosing may be required
- Carbamazepine and phenytoin — require significant warfarin dose increases
- St. John's Wort — herbal CYP3A4 inducer; patients on warfarin must avoid it
- Barbiturates
Dietary vitamin K is a frequent source of INR variability. High-vitamin K foods (kale, spinach, broccoli, Brussels sprouts, Swiss chard, collard greens) oppose warfarin's effect. The key clinical principle is consistency, not avoidance. Patients who eat a consistent amount of leafy greens will have a stable INR, even at a high vitamin K intake, because the warfarin dose can be adjusted accordingly. Sudden large increases in dietary vitamin K (e.g., beginning a green smoothie habit) lower the INR; sudden cessation raises it.
Acute illness is an underappreciated source of INR instability. Fever raises the catabolic rate of clotting factors; diarrhea impairs absorption of both warfarin and dietary vitamin K and disturbs the gut flora that make vitamin K2; and reduced oral intake during any illness cuts vitamin K1 supply. Each of these pushes the INR up, and they frequently arrive together, which is why a patient who was rock-steady for a year can present with an INR of 6 after a week of gastroenteritis. Any significant intercurrent illness in a warfarin patient is a reason to recheck the INR sooner than the routine schedule would call for.
Pharmacogenomics of warfarin: Two genes account for most of the interindividual variability in warfarin dosing:
- CYP2C9 variants (*2, *3, and others): slow S-warfarin metabolism → higher plasma warfarin concentrations → lower dose required. CYP2C9*3 homozygotes may need 50–75% less warfarin than wild-type.
- VKORC1 variants: the A haplotype (-1639G>A promoter variant) reduces VKORC1 expression, making the enzyme more easily inhibited → increased warfarin sensitivity → lower starting dose needed. The A/A genotype requires about 40% less warfarin than G/G. The A haplotype is markedly more common in East Asian populations than in European or African ones, which is a large part of why average therapeutic warfarin doses differ so much between these groups.
The FDA warfarin label (updated 2010) recommends considering genotyping when initiating warfarin. The EU PHAR study and COAG trial showed mixed results on whether genotype-guided dosing reduces adverse events versus clinical algorithms, but pharmacogenomic dosing reduces early supratherapeutic INR and bleeding in the first 90 days.
Time in therapeutic range (TTR) is the single most useful quality metric for warfarin management — more informative than any individual INR result. It is the proportion of time a patient's INR sits inside the target window, conventionally calculated by the Rosendaal linear-interpolation method. A TTR above 65–70% is associated with substantially lower rates of both thrombotic and hemorrhagic events, and warfarin managed to that standard approaches the outcomes seen with DOACs in the major atrial fibrillation trials. A persistently poor TTR — despite good adherence and a stable diet — is one of the strongest arguments for switching a patient to a direct oral anticoagulant.
Direct oral anticoagulants (DOACs) — rivaroxaban, apixaban, edoxaban (Factor Xa inhibitors) and dabigatran (direct thrombin inhibitor) — have replaced warfarin for most indications including non-valvular AF and VTE. Their fixed dosing, predictable pharmacokinetics, fewer drug interactions, and the absence of routine INR monitoring have made them the first-line choice in multiple guideline updates. Warfarin retains its role for patients with mechanical heart valves (DOACs are contraindicated), antiphospholipid syndrome with triple positivity (evidence of harm with DOACs), severe CKD (GFR < 15–25, where most DOACs are not studied), and patients who cannot afford newer agents.
PT as a Liver Function Test
The liver is the exclusive site of synthesis for virtually all coagulation factors. The major exceptions are Factor VIII and von Willebrand factor, both produced by vascular endothelium (and megakaryocytes for vWF). This means that impaired hepatic synthetic function — whether from acute liver failure, decompensated cirrhosis, or hepatitis-induced injury — rapidly depletes clotting factors and prolongs the PT. The PT is among the earliest and most sensitive markers of hepatic synthetic failure, appearing before hypoalbuminemia (albumin half-life ~20 days), before hyperbilirubinemia (which also reflects excretory dysfunction), and before overt coagulopathy is clinically apparent.
The PT/INR is incorporated into two key prognostic scoring systems for liver disease:
- Child-Pugh score: Assesses cirrhosis severity across five domains (PT/INR, albumin, bilirubin, ascites, hepatic encephalopathy). INR values contribute up to 3 points: a PT prolonged by less than 4 seconds (INR below 1.7) scores 1 point, prolongation of 4–6 seconds (INR 1.7–2.3) scores 2 points, and prolongation beyond 6 seconds (INR above 2.3) scores 3 points. Child-Pugh class C (score 10–15) predicts 1-year survival of approximately 45%. The score guides liver transplant listing decisions and predicts operative mortality for non-hepatic surgery.
- MELD score (Model for End-Stage Liver Disease): MELD = 3.78 × ln(bilirubin mg/dL) + 11.2 × ln(INR) + 9.57 × ln(creatinine mg/dL) + 6.43. Scores range from 6 to 40+. A MELD score above 15 generally identifies patients who benefit from liver transplantation over continued medical management. MELD-Na adds serum sodium for improved mortality prediction (MELD-Na = MELD + 1.32 × (137 – Na) – [0.24 × (137 – Na) × MELD]). UNOS uses MELD-Na for organ allocation in the United States.
The INR term carries a large coefficient in MELD (11.2), which makes the score unusually sensitive to it — and that is a recognized structural flaw. Thromboplastin reagents are calibrated against warfarin-treated plasma, not against the coagulopathy of liver disease, and the two mechanisms are not the same: warfarin depletes a specific set of vitamin K-dependent factors, while cirrhosis depresses synthesis across the board. The consequence is that two patients with identical hepatic synthetic function can receive materially different MELD scores depending solely on which reagent their local laboratory happens to stock, and therefore different positions on a transplant waiting list. This has driven proposals for liver-specific coagulation indices — an INR calibrated on cirrhotic rather than warfarin plasma (the so-called INRliver), or replacement of the INR term altogether with a thrombin generation assay or a direct Factor V level.
An important limitation: the INR is validated only for warfarin monitoring in patients with normal liver function. In patients with cirrhosis, the standard INR is NOT a reliable measure of actual bleeding risk. Cirrhotic patients have complex hemostatic rebalancing — they are simultaneously deficient in pro-coagulant factors (II, V, VII, X) but also deficient in anti-coagulant proteins (protein C, protein S, antithrombin), and they have elevated vWF and reduced ADAMTS13. The result is a fragile equilibrium that the INR does not capture. A cirrhotic patient with an INR of 1.8 may be perfectly hemostatic in vivo despite the elevated lab value. Thromboelastography (TEG) or rotational thromboelastometry (ROTEM) provide better real-time assessment of whole-blood clotting in this population, and frequently show near-normal global clot formation in clinically stable cirrhosis despite an alarming-looking INR.
This has a direct practical consequence: transfusing fresh frozen plasma purely to "correct" the INR before a procedure in a stable cirrhotic patient is usually unnecessary and is not harmless. Plasma is a large-volume product; in a patient with portal hypertension it raises portal pressure and can precipitate variceal bleeding, and it carries the standard transfusion hazards including volume overload and transfusion-related acute lung injury. Contemporary hepatology guidance discourages prophylactic plasma transfusion aimed at an INR target in stable cirrhosis, and directs attention instead to fibrinogen level, platelet count, and viscoelastic testing.
Acute liver failure (ALF) — a catastrophic syndrome of acute hepatic necrosis with encephalopathy — is defined in part by an INR above 1.5 (King's College criteria use INR > 6.5 as a poor prognosis indicator for acetaminophen ALF, or INR > 3.5 plus bilirubin > 17.5 mg/dL for non-acetaminophen ALF). Factor V levels, which reflect only synthetic function without vitamin K influence, are particularly useful in this setting — the Clichy criteria use Factor V < 20% in patients under 30, or < 30% in patients over 30, as an indicator for transplant listing.
Neonates normally have a mildly prolonged PT (11–15 seconds) at birth, reflecting both immature hepatic synthesis and relative vitamin K deficiency. This is physiologic and corrects within days with standard vitamin K supplementation.
Vitamin K and PT/INR
Vitamin K is a fat-soluble vitamin named for the German word Koagulationsvitamin, reflecting its essential role in blood clotting — identified by Danish biochemist Henrik Dam in the 1920s. It exists in two primary dietary forms with distinct sources and bioavailabilities:
- Vitamin K1 (phylloquinone): Found in leafy green vegetables (kale, spinach, Swiss chard, parsley, collard greens, broccoli, Brussels sprouts). K1 accounts for approximately 90% of dietary vitamin K intake in Western diets. It is absorbed from the small intestine in association with dietary fat; absorption requires bile acids and pancreatic lipase. The liver preferentially uses K1 for hepatic coagulation factor carboxylation.
- Vitamin K2 (menaquinones, MK-4 through MK-13): Found in fermented foods (natto, aged cheeses, fermented soybean products), animal organs, egg yolks, and some meats. MK-7 (from natto) has a longer half-life (~72 hours) than K1 (~1–2 hours), resulting in more stable plasma levels and potentially greater extra-hepatic effects. K2 is synthesized endogenously by gut microbiota but in limited, variable amounts.
The biochemical role of vitamin K is as the essential cofactor for gamma-glutamyl carboxylase (GGCX), the enzyme that adds a carboxyl group to specific glutamate residues (Gla residues) on vitamin K-dependent proteins. This reaction requires vitamin K hydroquinone (KH2) and converts it to vitamin K epoxide (K>O). The vitamin K cycle: K>O is recycled to K by vitamin K epoxide reductase (VKOR1), then to KH2 by either VKOR1 or DT-diaphorase. Warfarin blocks the VKOR1 step.
Vitamin K deficiency produces a predictable sequence of PT/INR changes governed by factor half-lives:
- Within 24–48 hours of severe deficiency: Factor VII (half-life 4–6 h) falls — PT/INR prolongs; aPTT remains normal. This is identical to the initial effect of warfarin.
- By 48–72 hours: Factors IX and X (half-life 24–48 h) decline — aPTT begins to prolong.
- By 4–5 days: Prothrombin (half-life 60–72 h) falls — full coagulopathy established; both PT and aPTT significantly prolonged.
- Fibrinogen and Factor V are unaffected (not vitamin K-dependent).
The PT/aPTT pattern (PT prolonged, aPTT normal → then both prolonged, fibrinogen normal) distinguishes vitamin K deficiency from DIC (where fibrinogen is consumed) and heparin (which prolongs aPTT >> PT).
Causes of clinical vitamin K deficiency include:
- Fat malabsorption: Cystic fibrosis, celiac disease, Crohn's disease (especially ileal involvement), short bowel syndrome, cholestatic liver disease (bile acid deficiency impairs fat-soluble vitamin absorption)
- Prolonged antibiotic therapy: Broad-spectrum antibiotics suppress vitamin K2-producing gut bacteria (Bacteroides, Prevotella, Fusobacterium); clinically significant only when combined with inadequate dietary K1 intake
- Newborns: Neonates have minimal vitamin K stores (poor placental transfer), a sterile gut (no K2 production), and little vitamin K in breast milk. Without prophylaxis, 1 in 10,000–20,000 neonates develop hemorrhagic disease of the newborn (HDN) — intracranial, GI, or skin bleeding. A single intramuscular vitamin K1 injection (1 mg) at birth virtually eliminates this risk. Oral prophylaxis is less effective, particularly for late-onset HDN (2–12 weeks).
- Malnutrition or prolonged NPO: Hospitalized patients on total parenteral nutrition (TPN) without vitamin K supplementation
Treatment of vitamin K deficiency (non-warfarin): oral or IV vitamin K1. IV administration (phytonadione) is faster but carries a small risk of anaphylactoid reactions (give slowly over 20–60 minutes, diluted). Oral dosing (2.5–25 mg) is effective for most non-emergent situations and reverses PT prolongation within 12–24 hours. Subcutaneous vitamin K is absorbed erratically and is no longer recommended.
Factor V Leiden and Coagulation Genetics
Factor V Leiden is the most prevalent inherited thrombophilia in populations of European ancestry, with a heterozygous carrier frequency of approximately 5% (1 in 20 individuals) and homozygous frequency of about 1 in 1,000. The mutation is a single nucleotide change at position 1691 in the Factor V gene (G→A), producing an arginine-to-glutamine substitution at amino acid position 506 (R506Q). This site is the primary cleavage site where activated Protein C (APC) normally inactivates Factor Va, terminating thrombin generation. The Leiden mutation makes Factor Va resistant to APC cleavage, resulting in prolonged thrombin generation and a net hypercoagulable state.
The thrombotic risk increase depends on zygosity and clinical context:
- Heterozygous FVL: 3–8-fold increased lifetime risk of VTE (DVT and PE) compared to the general population. Absolute risk remains low (~0.5–1.5% per year). Does not routinely require anticoagulation in the absence of VTE.
- Homozygous FVL: 18–80-fold increased VTE risk. Higher thrombotic burden; long-term anticoagulation often recommended after first VTE.
- Combined with OCP: Oral contraceptives increase VTE risk 3–6-fold on their own; heterozygous FVL + OCP = approximately 35-fold increased risk. Screening for FVL before OCP prescription is debated but recommended by some guidelines for women with a family history of VTE.
- Combined with other thrombophilias (e.g., prothrombin mutation, protein C/S deficiency): synergistic increase in VTE risk.
The PT and INR are typically normal in Factor V Leiden heterozygotes and homozygotes. The mutation increases thrombotic risk but does not impair clot formation speed (the PT measures clot formation, not clot dissolution or regulation). The APC resistance assay (a functional test measuring the ratio of aPTT with and without exogenous APC) and direct genetic PCR testing are the appropriate diagnostic methods.
Other inherited thrombophilias relevant to the coagulation testing context:
- Prothrombin G20210A mutation: The second most common inherited thrombophilia (~2–3% prevalence in European populations). A gain-of-function mutation in the 3' untranslated region of the prothrombin gene increases prothrombin mRNA stability, resulting in elevated prothrombin plasma levels (~130–145% of normal). PT may be mildly shortened. VTE risk increases 2–4-fold in heterozygotes.
- Protein C deficiency: Protein C is a vitamin K-dependent serine protease that, when activated by the thrombomodulin-thrombin complex, inactivates Factors Va and VIIIa. Deficiency is rare (~0.2–0.4% prevalence) but confers a 7–10-fold VTE risk increase. A critical clinical gotcha: warfarin rapidly depletes Protein C (short half-life ~8 h) before prothrombin falls. In patients with undiagnosed Protein C deficiency, the initial warfarin doses cause a transient hypercoagulable state, manifesting as warfarin-induced skin necrosis (hemorrhagic skin infarction, typically over adipose-rich areas) within the first 3–5 days of warfarin initiation. Treatment: stop warfarin, give FFP or Protein C concentrate, bridge with heparin.
- Protein S deficiency: Protein S is a vitamin K-dependent cofactor that enhances APC activity. Like Protein C deficiency, it carries 5–10-fold VTE risk increase and the warfarin skin necrosis risk.
- Antithrombin III deficiency: Antithrombin is the primary physiological inhibitor of thrombin and Factor Xa. Hereditary deficiency is rare (1:2,000–5,000) but carries the highest VTE risk of inherited thrombophilias (~25–50-fold increased lifetime risk). Heparin requires antithrombin as its cofactor — antithrombin-deficient patients may have resistance to heparin anticoagulation, requiring higher doses or antithrombin concentrate.
When evaluating for hereditary thrombophilia, the timing of testing matters. Acute thrombosis, pregnancy, OCP use, and acute illness all alter protein levels and may produce falsely abnormal or falsely normal results. Warfarin therapy reduces levels of all vitamin K-dependent proteins (Protein C, S, and coagulation factors). Testing is ideally performed 4–6 weeks after completing anticoagulation and in a clinical steady state.
Point-of-Care INR Testing
Self-monitoring of anticoagulation with home INR devices represents one of the most successful applications of point-of-care testing in chronic disease management. Two FDA-approved devices dominate the US market: the Roche CoaguChek XS (optical reflectance, liquid crystal display) and the now-discontinued INRatio2 (replaced by similar devices). Both analyze a small whole-blood sample (5–10 µL) from a fingerstick and produce a result in 60–120 seconds.
The technology works as follows: the test strip contains dried thromboplastin reagent. Blood applied to the strip reactivates the reagent. An optical or electrochemical sensor detects the change in blood properties as a clot forms and calculates the clotting time. The device applies a device-specific ISI to convert the clotting time to an INR. Each device is calibrated to the international thromboplastin reference standard.
Analytical performance: multiple comparative studies and meta-analyses have shown that point-of-care INR devices correlate closely with laboratory INR (Pearson r typically 0.97–0.99, mean absolute bias 0.1–0.3 INR units). In a large systematic review by Heneghan et al. (2012), POC devices were accurate across the therapeutic range (INR 1.5–4.5) but showed reduced reliability at very high INR values (>4.5) and in patients with elevated hematocrit, lupus anticoagulant, or lipaemic samples.
Patient self-management (PSM) programs allow patients to not only self-test but also self-adjust their warfarin dose based on a predefined algorithm, with provider oversight. The evidence base for PSM is robust:
- The STABLE study (Cromheecke et al., 2000) showed PSM patients spent 56% of time in therapeutic range vs. 49% in usual care
- A Cochrane meta-analysis of 18 trials (Heneghan et al., 2006, updated 2016) found PSM significantly reduced thromboembolic events (OR 0.51) and all-cause mortality (OR 0.74) compared to usual care
- PSM did not increase major bleeding events — in fact, hemorrhage rates were non-significantly lower
- PSM is most cost-effective for patients who require long-term (lifetime) warfarin: mechanical heart valves, chronic AF with multiple risk factors, recurrent VTE
Insurance coverage and patient selection: Medicare covers POC INR testing (CPT 93793) for patients with mechanical heart valves; commercial insurance coverage is variable. Ideal candidates are motivated patients with stable warfarin requirements, good manual dexterity, ability to understand and follow a dosing algorithm, and reliable follow-up. Patients with cognitive impairment, poor compliance history, or unstable INR due to comorbidities are not good candidates.
Limitations of POC INR testing:
- Not validated for non-warfarin coagulopathies (liver disease, DIC, Factor VII deficiency) — gives spuriously normal or misleading results in these contexts
- Hematocrit below 25% or above 55% may cause inaccurate readings
- Lupus anticoagulant causes falsely elevated INR on some devices
- Highly lipemic or icteric samples can interfere
- Does not monitor DOAC effect — rivaroxaban, apixaban, dabigatran, edoxaban do not require or benefit from INR testing
Causes of Prolonged PT/INR
A systematic approach to PT/INR prolongation considers whether the aPTT is normal or also prolonged, whether fibrinogen is affected, and the clinical context:
Isolated PT prolongation (aPTT normal, fibrinogen normal):
- Warfarin therapy — by far the most common cause in ambulatory patients; Factor VII depletion alone initially
- Vitamin K deficiency — early/mild; Factor VII falls first because of shortest half-life
- Hereditary Factor VII deficiency — rare autosomal recessive condition; homozygotes have variable bleeding phenotype (some have near-normal hemostasis despite Factor VII levels of 1–5%)
- Early liver disease — mild synthetic impairment with selective Factor VII reduction before other factors fall
- Acquired Factor VII inhibitor — extremely rare; can be seen in autoimmune conditions, pregnancy, or cancer
- Lupus anticoagulant — usually prolongs aPTT, but can occasionally present with isolated PT prolongation
Both PT and aPTT prolonged (fibrinogen normal or elevated):
- Advanced liver disease or acute liver failure — common pathway factors (X, V, II) depleted in addition to VII
- Vitamin K deficiency (severe or prolonged)
- Warfarin plus heparin or LMWH combination
- Massive warfarin overdose, or superwarfarin ingestion — long-acting rodenticides such as brodifacoum and difenacoum are vitamin K antagonists with half-lives measured in weeks rather than hours. Deliberate or accidental ingestion produces a profound coagulopathy that recurs for weeks to months after a single exposure, and treatment requires high-dose oral vitamin K1 sustained for that entire period rather than the days that suffice for warfarin.
- Hereditary deficiencies of Factors X, V, or II (prothrombin deficiency) — rare
- Amyloidosis — Factor X absorption onto amyloid fibrils causes selective Factor X depletion; both PT and aPTT prolong
- Excess heparin (supratherapeutic dosing or contaminated sample) — may prolong PT and aPTT
Both PT and aPTT prolonged with low fibrinogen and elevated D-dimer:
- Disseminated intravascular coagulation (DIC) — systemic activation of coagulation causing consumption of factors and fibrinogen simultaneously; platelet count is also typically low; schistocytes on peripheral blood smear confirm microangiopathic hemolysis. DIC can be triggered by sepsis, trauma, malignancy (particularly AML M3/APL), obstetric emergencies (placental abruption, amniotic fluid embolism), and snake envenomation. DIC is scored rather than diagnosed by any single test: the ISTH (International Society on Thrombosis and Haemostasis) overt DIC scoring system assigns points for platelet count, PT prolongation, fibrinogen level, and a fibrin-related marker (D-dimer or fibrin degradation products), with a total of 5 or more indicating overt DIC in a patient with a compatible underlying condition.
- Massive transfusion with dilutional coagulopathy — packed red blood cells lack clotting factors; more than 10 units of PRBCs without FFP replacement causes dilutional coagulopathy; trauma protocols use balanced resuscitation (1:1:1 ratio of PRBCs:FFP:platelets)
- Severe liver failure — fibrinogen is also a liver-synthesized protein; it falls late in liver failure but contributes to DIC-like picture in ALF
Spuriously prolonged PT (artifact):
- Underfilled citrate tube (most common pre-analytic error)
- Delayed processing (>4 hours at room temperature for citrate plasma)
- Clotted or hemolyzed sample
- Wrong tube (EDTA tube instead of citrate) — produces extremely prolonged PT and should be suspected if values are implausibly high
- Lipemia or icterus (interfere with optical clot detection)
- Very high hematocrit (>55%) with standard citrate volume
Interpretation tip — the mixing study: When the cause of PT or aPTT prolongation is unclear, mixing the patient's plasma 1:1 with normal pooled plasma and re-running the test identifies whether the prolongation is due to a factor deficiency (mixing corrects it) or an inhibitor (mixing fails to correct, or shows a characteristic "incubated mixing study" correction failure for time-sensitive inhibitors like Factor VIII inhibitors).
aPTT: The Intrinsic Pathway Partner Test
The PT is almost never interpreted alone. Its partner test, the activated partial thromboplastin time (aPTT), measures the intrinsic pathway (Factors XII, XI, IX, and VIII) together with the same common pathway the PT covers (X, V, II, and fibrinogen). Reading the two together is what converts a prolonged clotting time into a differential diagnosis.
The aPTT is performed by adding three things to citrated plasma: an activating agent (kaolin, ellagic acid, or micronized silica — the "activated" in the name), a phospholipid source without tissue factor (the "partial thromboplastin"), and calcium. Because no tissue factor is supplied, the reaction must start through contact activation, which is what makes the assay report on the intrinsic limb. A typical reference range is 25–38 seconds, laboratory-specific as always.
A prolonged aPTT with a normal PT localizes the defect to the intrinsic pathway:
- Factor VIII deficiency (hemophilia A): the most common severe inherited coagulation disorder; X-linked recessive, so it affects males predominantly
- Factor IX deficiency (hemophilia B, Christmas disease): clinically indistinguishable from hemophilia A without a specific factor assay — the aPTT cannot tell them apart
- Factor XI deficiency (hemophilia C): variable and often mild bleeding tendency that correlates poorly with the factor level; notably more common in Ashkenazi Jewish populations
- Von Willebrand disease, types 2 and 3: von Willebrand factor is the plasma carrier for Factor VIII, so severe vWD secondarily depletes Factor VIII and prolongs the aPTT
- Factor XII deficiency: prolongs the aPTT substantially but causes no bleeding whatsoever — a common source of alarm on a pre-operative screen in an asymptomatic patient
- Lupus anticoagulant: the central paradox of coagulation testing. The antiphospholipid antibody interferes with the phospholipid reagent and prolongs the aPTT in the tube, while causing thrombosis, not bleeding, in the patient. A 1:1 mixing study separates it from a true factor deficiency — deficiency corrects, lupus anticoagulant does not
- Unfractionated heparin: the principal clinical use of the aPTT. Therapeutic UFH is titrated to an aPTT of 1.5–2.5 times the control value, or to an equivalent anti-Xa level
Combining the two tests gives a compact decision table: PT prolonged with normal aPTT points to Factor VII (warfarin, early vitamin K deficiency, early liver disease); aPTT prolonged with normal PT points to the intrinsic factors or heparin; both prolonged points to the common pathway, to advanced liver failure, to severe vitamin K deficiency, or — when fibrinogen is low and D-dimer high — to DIC. When either test is unexpectedly prolonged, the mixing study described in the previous section is the next step in every case.
Urgent Reversal Strategies
When warfarin-associated coagulopathy causes life-threatening bleeding or an operation cannot wait, anticoagulation has to be undone quickly. The choice of agent is dictated by how fast the correction is needed and how much volume the patient can tolerate.
4-Factor Prothrombin Complex Concentrate (4F-PCC)
4F-PCC — marketed as Kcentra in the United States and as Beriplex or Octaplex elsewhere — is a plasma-derived concentrate of all four vitamin K-dependent procoagulant factors (II, VII, IX, and X) plus the anticoagulant proteins C and S. It corrects the INR to below 1.5 within roughly 15–30 minutes of infusion, and it does so in a small volume, typically 25–50 mL, which is the decisive advantage over plasma in an elderly patient with an intracranial hemorrhage and a marginal ejection fraction. It is the first-line agent for urgent reversal in life-threatening bleeding — intracranial hemorrhage, major gastrointestinal bleeding with hemodynamic compromise — and before emergency surgery. Dosing is weight- and INR-based. Always give intravenous vitamin K1 alongside it: the infused factors are cleared over the following hours while warfarin is still on board, so without vitamin K to restore endogenous synthesis the INR rebounds. The Sarode trial established 4F-PCC as non-inferior to plasma for hemostatic efficacy and superior for speed of INR correction.
Fresh Frozen Plasma (FFP)
FFP contains every coagulation factor, but at physiological rather than concentrated levels, so meaningful INR correction requires 10–20 mL/kg — typically 4 to 6 units, or 1,000–1,500 mL. It must be thawed (20–30 minutes) and ABO-compatible, which adds delay at exactly the moment delay is most costly. Compared with 4F-PCC it is slower, less complete, and carries the risks of volume overload and transfusion-related acute lung injury (TRALI). It remains the right choice when PCC is unavailable, when the patient needs factors that PCC does not contain — Factor V above all — and as part of a massive transfusion protocol alongside red cells and platelets in a balanced 1:1:1 ratio.
Vitamin K1 (Phytonadione)
Vitamin K1 does not act by replacing factors; it restores the substrate the liver needs to make them, so its effect is inherently delayed but durable. Given orally it lowers an elevated INR over roughly 24 hours, and intravenously — infused slowly and diluted, because of the small risk of an anaphylactoid reaction — within about 6–12 hours. For asymptomatic INR elevation, holding warfarin with or without low-dose oral vitamin K (1–2.5 mg) is standard; for minor bleeding at a high INR, 2.5–5 mg orally is appropriate; the intravenous route is reserved for serious bleeding, for emergency reversal alongside 4F-PCC, and for situations where oral absorption cannot be relied on. Subcutaneous administration is absorbed too erratically to be recommended.
Reversal of Direct Oral Anticoagulants
The DOACs do not belong on this page's monitoring scale at all: rivaroxaban, apixaban, and edoxaban (direct Factor Xa inhibitors) and dabigatran (a direct thrombin inhibitor) prolong the PT and aPTT unpredictably, and neither test is validated for measuring their effect. A normal PT does not exclude a therapeutic DOAC level. Reversal uses agent-specific antidotes: idarucizumab (Praxbind), a monoclonal antibody fragment, for dabigatran, and andexanet alfa (Andexxa), a decoy Factor Xa molecule, for the anti-Xa agents. Where the specific agent is unavailable, 4F-PCC is used as a non-specific reversal strategy. Dabigatran, uniquely among the DOACs, is also dialyzable.
Key Research and Citations
- Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(6 Suppl):160S–198S. PMID: 18574265
- Hirsh J, Dalen J, Anderson DR, et al. Managing oral anticoagulant therapy. Chest. 2001;119(1 Suppl):22S–38S. PMID: 11157641
- Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease. Chest. 2012;141(2 Suppl):e419S–e496S. PMID: 22315268
- Kaatz S, Kouides PA, Garcia DA, et al. Guidance on the emergent reversal of oral thrombin and factor Xa inhibitors. Am J Hematol. 2012;87(Suppl 1):S141–S145. PMID: 22473649
- Tripodi A, Mannucci PM. The coagulopathy of chronic liver disease. N Engl J Med. 2011;365(2):147–156. PMID: 21751907
- Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–2352. PMID: 19966341
- Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy. Chest. 2012;141(2 Suppl):e152S–e184S. PMID: 22315269
- Dahlback B. Blood coagulation. Lancet. 2000;355(9215):1627–1632. — Search PubMed
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease. J Am Coll Cardiol. 2012;60(24):e44–e164. Reference for warfarin AF management: Wann LS et al. 2011 ACCF/AHA/HRS focused update. J Am Coll Cardiol. 2011;57(2):223–242. — Search PubMed
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–1151. PMID: 19717844
- Seligsohn U, Lubetsky A. Genetic susceptibility to venous thrombosis. N Engl J Med. 2001;344(16):1222–1231. PMID: 11309638
- Tripodi A. The international normalized ratio. Clin Chem. 2007;53(7):1260–1261. — Search PubMed
- Hirsh J, Fuster V, Ansell J, Halperin JL. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. J Am Coll Cardiol. 2003;41(9):1633–1652. PMID: 12742309
- Quick AJ. The prothrombin in hemophilia and in obstructive jaundice. J Biol Chem. 1935;109:73–74. (Historical — the original description of the prothrombin time; accessible through the Journal of Biological Chemistry archives.)
- Segal JB, Dzik WH; Transfusion Medicine/Hemostasis Clinical Trials Network. Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures. Transfusion. 2005;45(9):1413–1425. PMID: 16131373
- Taylor FB Jr, Toh CH, Hoots WK, et al. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86(5):1327–1330. PMID: 11816725
- Sarode R, Milling TJ Jr, Refaai MA, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study. Circulation. 2013;128(11):1234–1243. PMID: 23935011
- Nuttall GA, Brost BC, Connis RT, et al. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiology. 2006;105(1):198–208. — Search PubMed
- Schulman S, Angeras U, Bergqvist D, et al. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J Thromb Haemost. 2010;8(1):202–204. — Search PubMed
- Nishijima DK, Shahlaie K, Sarkar K, et al. Elevated admission international normalized ratio and outcomes after traumatic brain injury. — Search PubMed
- Weitz JI, Semchuk W, Turpie AG, et al. Trends in prescribing oral anticoagulants in Canada, 2008–2014. Clin Ther. 2015;37(11):2506–2514. — Search PubMed
- Mannucci PM, Canciani MT, Forza I, et al. Changes in health and disease of the metalloprotease that cleaves von Willebrand factor. Blood. 2001;98(9):2730–2735. — Search PubMed
PubMed searches for further reading:
- Warfarin INR monitoring therapeutic range — PubMed
- Prothrombin time liver disease MELD score — PubMed
- Factor V Leiden thrombophilia VTE risk — PubMed
- Point-of-care INR patient self-management — PubMed
- Vitamin K deficiency coagulopathy treatment — PubMed
- Prothrombin complex concentrate warfarin reversal — PubMed
- Disseminated intravascular coagulation diagnosis criteria — PubMed
- aPTT intrinsic pathway hemophilia lupus anticoagulant — PubMed
- PT/INR liver disease cirrhosis coagulopathy — PubMed
Connections
- All Lab Tests
- Coagulation Panel
- D-Dimer
- aPTT
- Fibrinogen Test
- Vitamin K
- Vitamin K2
- Complete Blood Count
- Hematology Diseases
- Cardiovascular Disease
- Liver Disease — why a prolonged PT/INR tracks failing hepatic synthesis, and where MELD uses it.