Cystatin C
Cystatin C is a simple blood test that gives your doctor a window into how well your kidneys are filtering. For decades, the go-to way to check kidney filtration has been a blood test called creatinine, and it works well for most people. But creatinine has a quirk: it is a byproduct of muscle, so how much you carry in your blood depends partly on how muscular you are. Cystatin C sidesteps that problem. It is a small protein that essentially every cell in your body makes at a fairly steady pace, so its blood level tracks kidney filtration more directly — with far less influence from your muscle mass, age, sex, or what you ate.
That makes cystatin C especially useful for people in whom creatinine can mislead: older adults, very muscular athletes, frail or low-muscle patients, amputees, and some people with liver disease. This page explains what cystatin C is, why doctors order it, how it plugs into the modern (and now race-free) equations that estimate your GFR — the number that summarizes kidney function — how to read your result, and where the test still has blind spots. It is meant to inform, not to replace, a conversation with your own clinician.
Table of Contents
- What Cystatin C Is
- Why the Test Is Used
- Its Big Advantage Over Creatinine
- Cystatin C and the eGFR Equations
- Race-Free eGFR
- When Doctors Order It
- How It's Measured and How to Read It
- Limitations and What Can Affect It
- Related Tests
- When to Talk to a Doctor
- Research Papers
- Connections
- Featured Videos
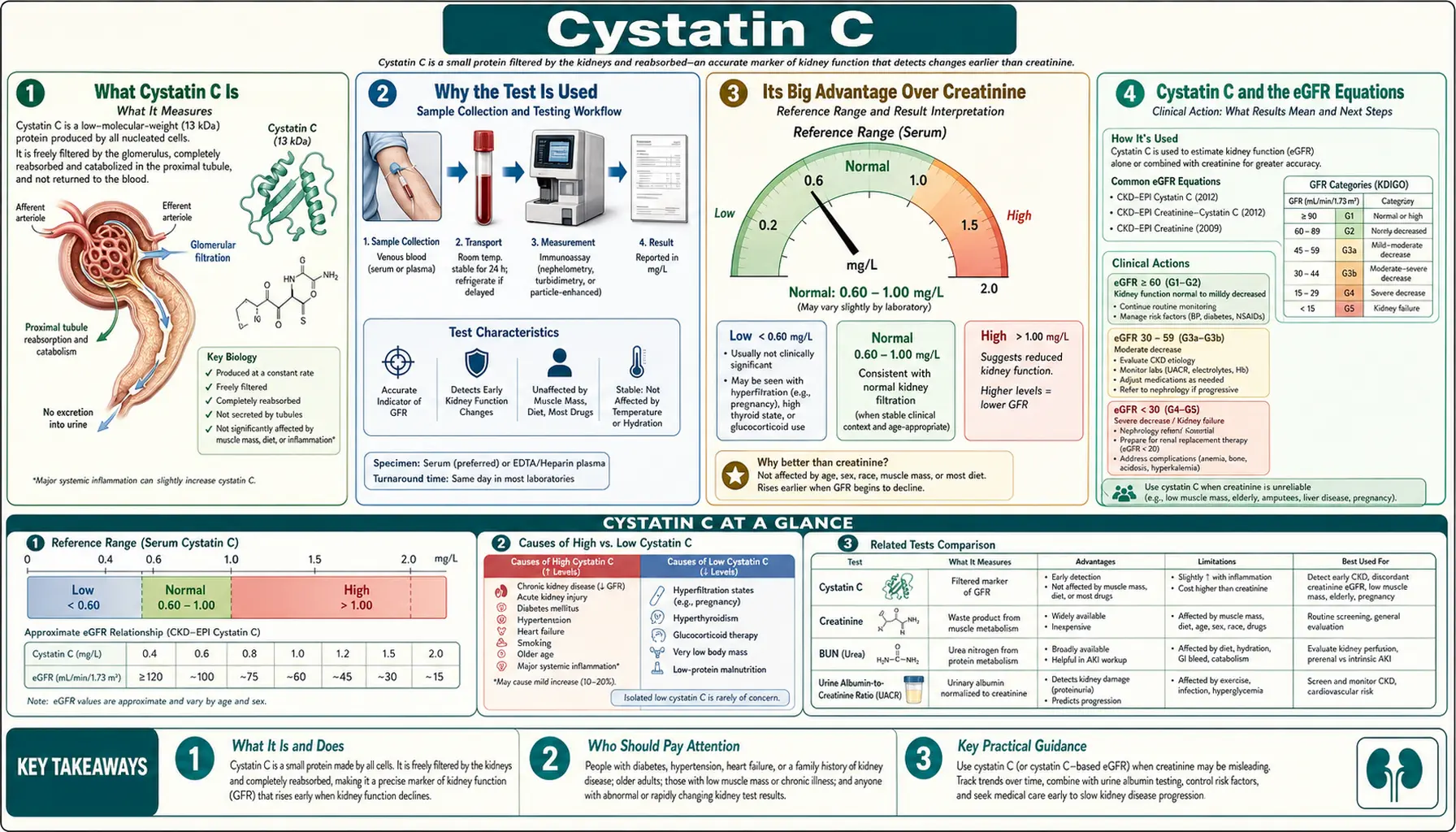
What Cystatin C Is
Cystatin C is a small protein — about 13 kilodaltons, which is tiny as proteins go — that is produced by all nucleated cells in your body. Because nearly every cell type makes it, and makes it at a fairly constant rate, the amount your body releases into the bloodstream stays relatively steady from person to person and day to day. Its job in the body is to act as a natural brake on certain enzymes (it inhibits cysteine proteases), but for the purpose of a lab test, what matters is what happens to it after it enters your blood.
Here is the elegant part. Cystatin C is small enough to pass freely through the kidney's filters (the glomeruli). Once it passes through, the kidney's tubules reabsorb it and break it down — almost none of it comes back into the blood or shows up in the urine. So the concentration left circulating in your blood depends mostly on one thing: how fast your kidneys are filtering it out. When filtration is strong, blood cystatin C stays low. When filtration slows, cystatin C backs up and its blood level rises.
That is why a single blood draw for cystatin C serves as a stand-in for the kidney's overall filtering power, known as the glomerular filtration rate (GFR). You cannot measure true GFR directly in everyday practice — doing so requires injecting a tracer and collecting timed samples — so clinicians rely on blood markers like creatinine and cystatin C to estimate it. Cystatin C is one of the most reliable of those markers.
Why the Test Is Used
The core reason to measure cystatin C is to assess kidney function. In practice it is used as an alternative to or a complement to creatinine rather than a wholesale replacement. Creatinine is cheap, fast, and available in every lab, so it remains the first-line marker for most people. Cystatin C steps in when a clinician wants a second, independent read on filtration — either to confirm a borderline result or because creatinine is known to be unreliable in that particular patient.
Doctors use cystatin C to help answer several practical questions:
- Is an abnormal creatinine result real? If a creatinine-based estimate lands in a gray zone, a cystatin C measurement can confirm or soften the concern.
- Is there early kidney disease that creatinine is missing? Creatinine can stay in the "normal" range until a fair amount of kidney function is already lost. Cystatin C sometimes flags a decline sooner.
- How aggressively should a medication be dosed? Many drugs are cleared by the kidneys, and their doses are set from estimated GFR. A more accurate GFR means safer dosing.
- How is a person with known kidney disease or a transplant trending over time?
Beyond kidney function itself, higher cystatin C levels have been linked in large studies to a greater risk of heart problems and death, even among people whose creatinine looked reassuring. That does not make cystatin C a "heart test," but it is one reason researchers and some clinicians take an elevated level seriously.
Its Big Advantage Over Creatinine
To understand why cystatin C is valuable, it helps to understand where creatinine falls short. Creatinine is a waste product of muscle metabolism. The more muscle mass you carry, the more creatinine you generate — regardless of how your kidneys are doing. That means creatinine reflects two things at once: your kidney filtration and your muscle mass. For an average-sized adult those cancel out nicely, but at the edges they don't.
Cystatin C is far less dependent on muscle mass, age, sex, and diet. Because it is made by cells throughout the body rather than by muscle specifically, and because it is not meaningfully affected by a protein-rich meal the way creatinine can be, it gives a cleaner signal of filtration in the very people where creatinine tends to mislead:
- Older adults, who often lose muscle with age. Low muscle can make their creatinine look deceptively normal, hiding real kidney decline.
- Very muscular people, such as competitive athletes or heavy weight-trainers, whose high muscle mass can make creatinine look alarming when their kidneys are fine.
- Frail, malnourished, or low-muscle patients, including many people with serious chronic illness, where creatinine underestimates the problem.
- Amputees and people with muscle-wasting conditions, where creatinine-based estimates are notoriously unreliable.
- People with liver disease, in whom creatinine can be low and misleading.
- Children, whose muscle mass changes rapidly as they grow, making cystatin C-based equations attractive in pediatrics.
- People following very high- or very low-protein diets, or taking creatine supplements, which can shift creatinine independently of kidney function.
A well-known meta-analysis concluded that cystatin C correlates more closely with true GFR than creatinine does, and the practical takeaway from the research literature is not "cystatin C always wins" but rather "when creatinine and cystatin C disagree, the disagreement itself is informative — and the combination of the two is usually the most accurate of all."
Cystatin C and the eGFR Equations
A raw cystatin C number in milligrams per liter is not very intuitive on its own, so labs feed it into a formula that converts it into an estimated GFR (eGFR) — the familiar number reported in "mL/min/1.73 m²," where higher is better and roughly 90 or above is considered normal for many adults. There are three main flavors of estimate:
- Creatinine-based eGFR (eGFR-cr): the traditional estimate, calculated from your creatinine.
- Cystatin C-based eGFR (eGFR-cys): calculated from cystatin C alone, useful as an independent check.
- Combined creatinine-cystatin C eGFR (eGFR-cr-cys): calculated from both markers together.
The landmark 2012 study by Inker and colleagues, published in the New England Journal of Medicine, developed and validated the widely used CKD-EPI cystatin C and combined equations. Its central finding is one worth remembering: the combined creatinine-cystatin C equation is more accurate than either marker used alone. That is why guidelines often recommend the combined estimate when a precise number really matters — for example, when a borderline eGFR would change whether someone is diagnosed with chronic kidney disease or how a drug is dosed.
In everyday care, the sequence often looks like this: your creatinine-based eGFR comes back borderline; your doctor adds a cystatin C; and the lab reports a combined eGFR that either eases the concern or confirms it. Neither number is a perfect measurement of true GFR, but together they narrow the uncertainty.
Race-Free eGFR
For years, the most common creatinine equations included a "race coefficient" that adjusted the result for people identified as Black. This practice drew serious criticism, because race is a social category, not a biological measurement of kidney function, and the adjustment could delay recognition of kidney disease. In response, a joint National Kidney Foundation and American Society of Nephrology task force recommended in 2021 moving to equations that do not use race at all.
Cystatin C is central to this shift. Because it does not depend on muscle characteristics the way creatinine does, it provides a race-independent way to refine the estimate. The 2021 New England Journal of Medicine paper by Inker and colleagues introduced new creatinine and cystatin C equations that omit race, and the combined creatinine-cystatin C version was found to be the most accurate and least biased across groups. As a result, many health systems now offer, and sometimes prefer, a cystatin C-inclusive eGFR precisely because it lets them estimate kidney function fairly without invoking race. If you have seen headlines about "removing race from kidney testing," cystatin C is a big part of how that was accomplished.
When Doctors Order It
Cystatin C is not usually part of a routine annual panel. It is ordered deliberately, when there is a specific reason to want a better estimate of kidney function than creatinine alone can give. Common situations include:
- Confirming or refining a borderline creatinine-based eGFR — for example, an eGFR hovering near the threshold that separates "normal" from early chronic kidney disease.
- Detecting early kidney disease in someone at risk (diabetes, high blood pressure, family history) when creatinine still looks normal but suspicion is high.
- Before dosing certain medications that are cleared by the kidneys and have a narrow safety margin, where an inaccurate GFR could mean too much or too little drug — some chemotherapy agents and certain antibiotics are examples.
- Monitoring people with chronic kidney disease (CKD) or a kidney transplant, where tracking function accurately over time guides treatment.
- Assessing patients where creatinine is known to mislead — the elderly, the very muscular, amputees, the frail, and people with significant liver disease or muscle-wasting conditions.
- Sorting out conflicting results, such as a normal creatinine paired with signs that point toward reduced kidney function.
The test is a simple blood draw, usually from a vein in your arm, and typically does not require fasting or special preparation. Ask your ordering clinician whether any of your medications or conditions should be noted, since a few can nudge the result (covered below).
How It's Measured and How to Read It
Cystatin C is measured in a blood sample using immunoassay methods (commonly nephelometry or turbidimetry), which detect the protein using antibodies. Since 2010 there has been an internationally certified reference material (known as ERM-DA471/IFCC) that helps different labs and instruments report cystatin C on a common scale — an important step, because before standardization, results from different machines were not always comparable.
Reading the result comes down to one simple direction, plus an important caveat:
- Higher cystatin C means slower filtration (worse kidney function). As kidney filtration declines, cystatin C accumulates in the blood, so the number climbs.
- Lower cystatin C generally means better filtration.
- Reference ranges are lab-dependent. Many labs report a normal adult serum cystatin C in the neighborhood of roughly 0.6 to 1.0 mg/L, but the exact interval varies by laboratory, method, and instrument, and normal values tend to run a little higher in older adults. Always interpret your value against your lab's stated reference range, printed on the report.
- The eGFR is what most people act on. Rather than the raw mg/L figure, your clinician will usually focus on the cystatin C-based or combined eGFR the lab calculates from it, because that number (mL/min/1.73 m²) maps onto the standard stages of kidney function.
One value on one day is a snapshot, not a diagnosis. Trends over weeks and months, viewed alongside creatinine and a urine test, tell a far more reliable story than any single reading.
Limitations and What Can Affect It
Cystatin C is excellent, but it is not flawless, and honesty about its blind spots matters. Several factors other than kidney filtration can nudge the level, and a few practical drawbacks limit how widely it is used:
- Thyroid dysfunction. An overactive thyroid (hyperthyroidism) tends to raise cystatin C, while an underactive thyroid (hypothyroidism) tends to lower it — independent of kidney function — so untreated thyroid disease can distort the result.
- High-dose corticosteroids. Steroids such as prednisone, particularly at high doses, can increase cystatin C production and push the level up.
- Other influences. Research has identified additional factors — including higher body weight and fat mass, smoking, inflammation, and possibly some cancers — that can affect cystatin C to a modest degree beyond kidney filtration alone.
- Cost and availability. Cystatin C is more expensive than creatinine and is not offered by every laboratory, so it is used selectively rather than as a universal screen.
- Still an estimate. Like creatinine, cystatin C only estimates GFR. In situations that demand a true measured GFR — certain transplant or research settings — a formal tracer study is still the reference standard.
Because of these caveats, no single marker is treated as the last word. The most confident picture of kidney health usually comes from combining cystatin C with creatinine, a urine test for protein, and the clinical context.
Related Tests
Cystatin C rarely travels alone. It is most useful alongside a handful of companion tests that together sketch a fuller picture of kidney health:
- Creatinine and creatinine-based eGFR. The traditional first-line filtration markers; cystatin C confirms, refines, or combines with them.
- Blood urea nitrogen (BUN). Another waste product filtered by the kidneys, often reported with creatinine on routine panels.
- Estimated GFR (eGFR). The calculated summary number that cystatin C helps produce, especially in its combined and race-free forms.
- Urine albumin and the albumin-to-creatinine ratio (ACR). These detect protein leaking into the urine, an early and independent sign of kidney damage. Filtration (from cystatin C) and leakage (from ACR) measure different things, which is why both are recommended together.
- Basic and comprehensive metabolic panels. Broad blood panels that include creatinine, BUN, and electrolytes and give kidney function its everyday context.
When to Talk to a Doctor
A cystatin C result is a piece of information, not a verdict, and it is best understood with your clinician. Reach out if any of the following apply:
- Your cystatin C or the calculated eGFR is outside your lab's reference range, or has changed noticeably from previous results.
- Your creatinine and cystatin C estimates disagree, and you want to understand what the difference means for you.
- You have diabetes, high blood pressure, or a family history of kidney disease and want to know whether a more accurate filtration estimate is worthwhile.
- You are older, very muscular, frail, an amputee, or have liver disease — situations where creatinine may be misleading and cystatin C may add clarity.
- You are starting a medication cleared by the kidneys and want your dose set from the most accurate GFR available.
- You have symptoms that can accompany kidney trouble — swelling in the legs or around the eyes, foamy urine, unusual fatigue, or changes in how much you urinate.
Kidney disease is often silent in its early stages, which is exactly why an accurate filtration estimate can matter. If your numbers prompt concern, your clinician can decide whether to repeat the test, add a urine test, or refer you to a kidney specialist (nephrologist). This page is educational and is not a substitute for individualized medical advice.
Research Papers
- Inker LA, Schmid CH, Tighiouart H, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. New England Journal of Medicine. 2012;367(1):20–29. doi:10.1056/NEJMoa1114248 — the landmark study that developed the CKD-EPI cystatin C and combined equations and showed the combined marker is more accurate than either alone.
- Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. New England Journal of Medicine. 2021;385(19):1737–1749. doi:10.1056/NEJMoa2102953 — introduced the race-free eGFR equations, with the combined creatinine-cystatin C version proving most accurate and least biased.
- Shlipak MG, Matsushita K, Ärnlöv J, et al. Cystatin C versus creatinine in determining risk based on kidney function. New England Journal of Medicine. 2013;369(10):932–943. doi:10.1056/NEJMoa1214234 — a large meta-analysis showing cystatin C-based eGFR strengthens the link between kidney function and the risk of death and end-stage disease.
- Shlipak MG, Sarnak MJ, Katz R, et al. Cystatin C and the risk of death and cardiovascular events among elderly persons. New England Journal of Medicine. 2005;352(20):2049–2060. doi:10.1056/NEJMoa043161 — found that higher cystatin C predicted death and cardiovascular events in older adults, even when creatinine looked normal.
- Stevens LA, Coresh J, Schmid CH, et al. Estimating GFR using serum cystatin C alone and in combination with serum creatinine: a pooled analysis of 3,418 individuals with CKD. American Journal of Kidney Diseases. 2008;51(3):395–406. doi:10.1053/j.ajkd.2007.11.018 — early pooled analysis supporting cystatin C-based and combined GFR estimates.
- Peralta CA, Shlipak MG, Judd S, et al. Detection of chronic kidney disease with creatinine, cystatin C, and urine albumin-to-creatinine ratio and association with progression to end-stage renal disease and mortality. JAMA. 2011;305(15):1545–1552. doi:10.1001/jama.2011.468 — showed that combining cystatin C with creatinine and urine ACR improves prediction of kidney outcomes.
- Dharnidharka VR, Kwon C, Stevens G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: a meta-analysis. American Journal of Kidney Diseases. 2002;40(2):221–226. doi:10.1053/ajkd.2002.34487 — pooled evidence that cystatin C correlates with true GFR more closely than creatinine.
- Knight EL, Verhave JC, Spiegelman D, et al. Factors influencing serum cystatin C levels other than renal function and the impact on renal function measurement. Kidney International. 2004;65(4):1416–1421. doi:10.1111/j.1523-1755.2004.00517.x — identified non-kidney factors (weight, smoking, inflammation, and others) that can affect cystatin C.
- Fricker M, Wiesli P, Brändle M, et al. Impact of thyroid dysfunction on serum cystatin C. Kidney International. 2003;63(5):1944–1947. doi:10.1046/j.1523-1755.2003.00925.x — showed hyperthyroidism raises and hypothyroidism lowers cystatin C independent of kidney function.
- Schwartz GJ, Muñoz A, Schneider MF, et al. New equations to estimate GFR in children with CKD. Journal of the American Society of Nephrology. 2009;20(3):629–637. doi:10.1681/ASN.2008030287 — developed pediatric GFR equations incorporating cystatin C, important where children's muscle mass changes rapidly.
- Delgado C, Baweja M, Crews DC, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. Journal of the American Society of Nephrology. 2021;32(12):2994–3015. doi:10.1681/ASN.2021070988 — the task-force recommendation to adopt race-free equations and expand cystatin C testing.
- Grubb A, Blirup-Jensen S, Lindström V, et al. First certified reference material for cystatin C in human serum ERM-DA471/IFCC. Clinical Chemistry and Laboratory Medicine. 2010;48(11):1619–1621. doi:10.1515/CCLM.2010.318 — established the international reference standard that lets labs report cystatin C on a common, comparable scale.
Connections
- Kidney Function Tests (BUN, Creatinine, eGFR)
- Microalbumin & Albumin-to-Creatinine Ratio
- Basic Metabolic Panel
- Comprehensive Metabolic Panel
- Albumin
- Chronic Kidney Disease
- Diabetic Nephropathy
- Nephrology & Hepatology
- Cystatin C in the Kidney Function Panel — the same marker read alongside BUN, creatinine and eGFR, including the combined CKD-EPI equation.
- All Lab Tests