ANCA Test: Antineutrophil Cytoplasmic Antibody Testing for Vasculitis
Antineutrophil cytoplasmic antibodies (ANCA) are autoantibodies directed against proteins stored in the primary granules of neutrophils and in monocyte lysosomes. The ANCA test is the cornerstone laboratory investigation for diagnosing ANCA-associated vasculitides (AAV) — a group of small- to medium-vessel inflammatory diseases that can cause rapidly progressive organ failure, particularly of the kidneys and lungs. Understanding the two major ANCA patterns and their corresponding antigens, and always confirming indirect immunofluorescence (IIF) results with antigen-specific immunoassays, is essential for accurate diagnosis and avoidance of false positives.
Table of Contents
- Overview — What Is the ANCA Test?
- Testing Methodology: IIF and Antigen-Specific EIA
- ANCA Patterns: c-ANCA vs. p-ANCA
- ANCA-Associated Vasculitides
- Reference Ranges and Interpretation
- False Positives and Mimics
- Drug-Induced ANCA Vasculitis
- Serial ANCA Monitoring for Disease Activity
- Key Research and Citations
- Connections
- Featured Videos
Overview — What Is the ANCA Test?
ANCA were first described by Davies et al. in 1982 in patients with segmental necrotizing glomerulonephritis. The subsequent discovery that they react against specific neutrophil granule proteins — proteinase 3 (PR3) and myeloperoxidase (MPO) — transformed understanding of a previously enigmatic group of vasculitides. The 2017 revised International Chapel Hill Consensus Conference (CHCC) nomenclature recognizes ANCA-associated vasculitis as a distinct category of small-vessel vasculitis driven by these autoantibodies.
ANCA are thought to be pathogenic rather than merely diagnostic markers. In vitro and animal model evidence indicates that ANCA (particularly anti-PR3 and anti-MPO) activate primed neutrophils, causing them to degranulate and release oxidants and proteases against vascular endothelium. This mechanism explains why ANCA vasculitis predominantly affects small vessels: neutrophils adhere to and damage the thin-walled capillaries and venules of the kidneys, lungs, sinuses, and skin.
The ANCA test is indicated in patients presenting with:
- Rapidly progressive glomerulonephritis (RPGN) — rising creatinine, hematuria, red cell casts
- Pulmonary-renal syndrome — simultaneous lung hemorrhage and glomerulonephritis
- Unexplained upper respiratory tract destruction — saddle-nose deformity, chronic sinusitis, subglottic stenosis
- Pulmonary nodules or cavities with constitutional symptoms
- Mononeuritis multiplex with systemic inflammation
- Unexplained palpable purpura or skin ulcers
Testing Methodology: IIF and Antigen-Specific EIA
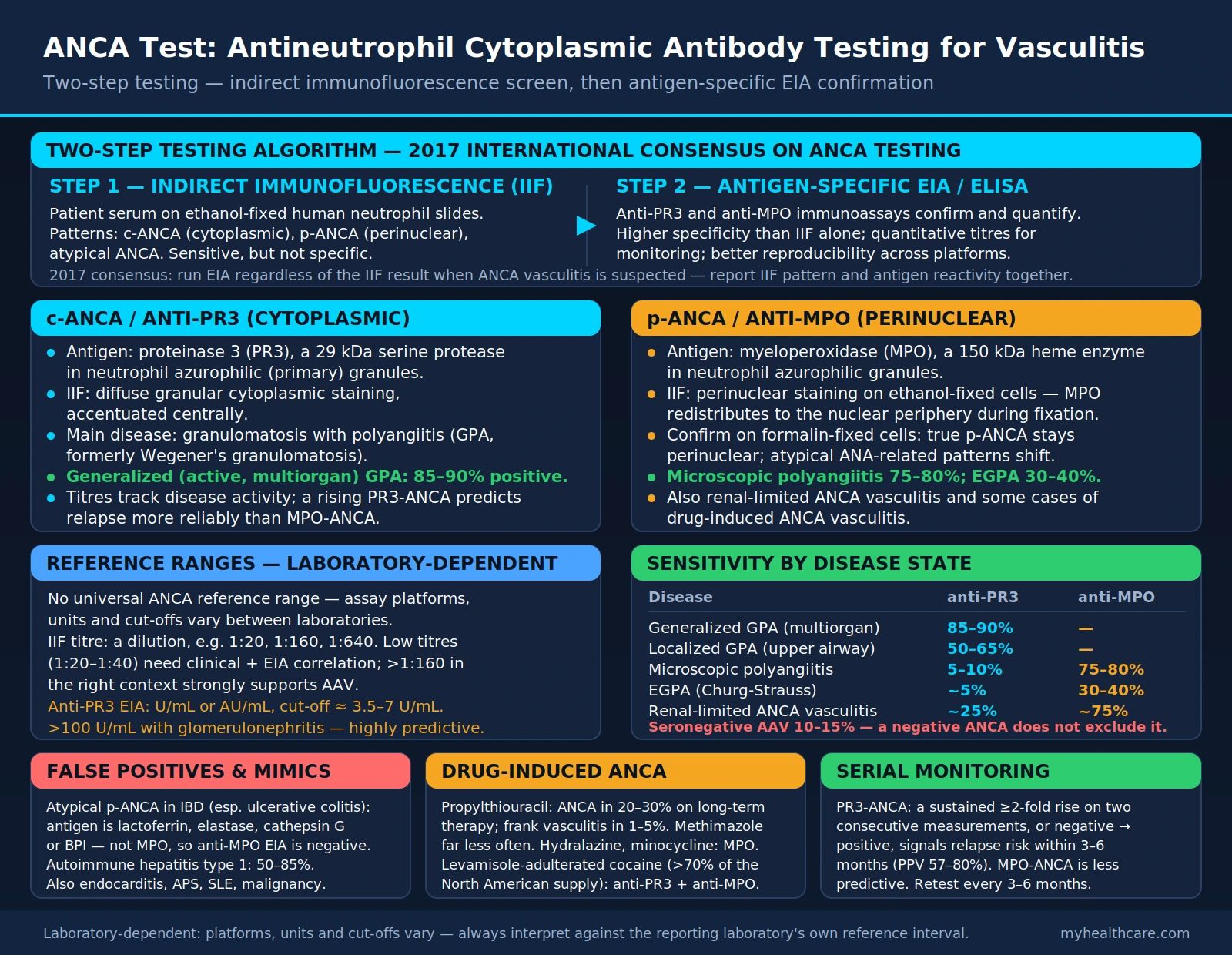
ANCA testing employs a two-step strategy mandated by major international guidelines including the 2017 International Consensus Statement on ANCA Testing:
Step 1 — Indirect Immunofluorescence (IIF)
Patient serum is incubated on ethanol-fixed human neutrophil substrate slides. Fluorescence microscopy reveals one of several staining patterns:
- c-ANCA (cytoplasmic): Diffuse granular cytoplasmic staining, accentuated centrally. The classic pattern associated with anti-PR3 antibodies. Originally described in Wegener's granulomatosis (now granulomatosis with polyangiitis).
- p-ANCA (perinuclear): Perinuclear staining on ethanol-fixed substrate, which arises from MPO redistributing to the nuclear periphery during fixation. Confirmed as truly MPO-directed by testing on formalin-fixed cells (true p-ANCA remains perinuclear; atypical ANA-related patterns shift).
- Atypical ANCA: Does not fit classic c- or p-ANCA patterns; seen in IBD, autoimmune hepatitis, drug reactions. Clinically significant mainly as a source of false positives.
IIF is sensitive but not specific. The 2017 consensus changed the recommended testing algorithm: antigen-specific EIA is now validated as a first-line test and should always be performed regardless of IIF result when ANCA vasculitis is clinically suspected.
Step 2 — Antigen-Specific Immunoassay (EIA/ELISA)
Anti-PR3 (proteinase 3) and anti-MPO (myeloperoxidase) ELISAs or multiplexed bead assays confirm and quantify the specific autoantibody. These tests provide:
- Higher specificity for AAV than IIF alone (particularly when IIF is atypical)
- Quantitative titers useful for monitoring disease activity over time
- Better reproducibility across laboratory platforms
- The ability to detect ANCA in IIF-negative patients (rare but documented in MPO-ANCA vasculitis)
The shift to high-sensitivity, high-specificity EIA platforms means that a negative IIF with a positive anti-PR3 or anti-MPO EIA should be taken seriously and not dismissed as a false positive. The 2017 consensus recommends that clinical laboratories report both IIF pattern and specific antigen reactivity together.
ANCA Patterns: c-ANCA vs. p-ANCA
c-ANCA / Anti-PR3 Antibodies
Proteinase 3 (PR3) is a 29 kDa serine protease stored in neutrophil azurophilic (primary) granules. It plays roles in killing pathogens and in modulating inflammation through cleavage of cytokines. PR3 is constitutively expressed on the surface of neutrophils in ANCA vasculitis patients to a greater degree than in healthy individuals — a phenomenon called "membrane PR3 expression" that may predispose to ANCA-mediated neutrophil activation.
Anti-PR3 antibodies produce the classic c-ANCA pattern on IIF. They are strongly associated with granulomatosis with polyangiitis (GPA, formerly Wegener's granulomatosis) — present in approximately 85–90% of generalized (active, multiorgan) GPA, and in a substantially smaller share of localized (upper respiratory only) GPA (see the sensitivity figures under Reference Ranges). Anti-PR3 titers tend to correlate more closely with disease activity than anti-MPO, and rising PR3-ANCA titers predict relapse more reliably.
p-ANCA / Anti-MPO Antibodies
Myeloperoxidase (MPO) is a 150 kDa heme-containing enzyme in neutrophil azurophilic granules. It catalyzes the production of hypochlorous acid (HOCl) from hydrogen peroxide and chloride — a potent antimicrobial mechanism that also causes bystander tissue damage in ANCA vasculitis. Anti-MPO antibodies produce the p-ANCA pattern on ethanol-fixed IIF.
Anti-MPO is the dominant ANCA specificity in microscopic polyangiitis (MPA) — present in approximately 75–80% of cases — and is also seen in eosinophilic GPA (formerly Churg-Strauss syndrome, approximately 30–40%), renal-limited ANCA vasculitis, and some drug-induced ANCA vasculitis cases. Anti-MPO-associated disease is more likely than anti-PR3 to manifest as renal-limited disease without granulomatous inflammation.
ANCA-Associated Vasculitides
Granulomatosis with Polyangiitis (GPA)
Formerly Wegener's granulomatosis, GPA is characterized by necrotizing granulomatous inflammation of the upper and lower respiratory tract combined with pauci-immune necrotizing glomerulonephritis. The classic triad of sinusitis, pulmonary disease, and renal disease is present in only 15–20% of cases at presentation; localized upper airway disease may precede systemic manifestations by years. Hallmarks include saddle-nose deformity from cartilage destruction, subglottic stenosis, pulmonary nodules or cavities (which may be mistaken for malignancy or infection), and rapidly progressive GN. Anti-PR3 is positive in 85–90% of generalized GPA. Tissue biopsy showing necrotizing granulomatous vasculitis remains the gold standard for diagnosis when feasible.
Microscopic Polyangiitis (MPA)
MPA is a necrotizing small-vessel vasculitis with pauci-immune glomerulonephritis and frequent pulmonary capillaritis, but without the granulomatous inflammation that defines GPA. It is the most common cause of pulmonary-renal syndrome. Anti-MPO is present in 75–80% of MPA cases; PR3-ANCA occurs in a minority. MPA has a higher risk of ESRD than GPA and a lower relapse rate after remission induction.
Eosinophilic Granulomatosis with Polyangiitis (EGPA)
Formerly Churg-Strauss syndrome, EGPA combines asthma, peripheral blood eosinophilia (>10%), and necrotizing granulomatous vasculitis. ANCA (predominantly anti-MPO) is positive in only 30–40% of EGPA — the ANCA-positive subset has more renal and peripheral nerve involvement (mononeuritis multiplex), while ANCA-negative EGPA tends to have more prominent cardiac and pulmonary eosinophilic infiltration. The FFS (Five-Factor Score) guides prognosis and treatment decisions.
Rapidly Progressive Glomerulonephritis (RPGN)
RPGN is a clinical syndrome — not a single disease — characterized by a rapid decline in GFR over days to weeks, hematuria, red cell casts, and proteinuria. Approximately 70–80% of pauci-immune crescentic GN (the most common RPGN subtype) is ANCA-positive. When RPGN is suspected, ANCA testing should be obtained urgently alongside anti-GBM antibodies (to exclude Goodpasture syndrome), complement levels (to exclude immune complex disease), and kidney biopsy. In a patient with RPGN and strong clinical suspicion for AAV, treatment should not be delayed awaiting biopsy results — immunosuppression (pulse methylprednisolone + cyclophosphamide or rituximab) should begin as soon as other diagnoses are reasonably excluded.
Reference Ranges and Interpretation
There is no universal ANCA reference range because assay platforms, units, and cut-offs vary significantly between laboratories. Results should always be interpreted with the specific assay's reference interval in mind.
- IIF titer: Expressed as a dilution (e.g., 1:20, 1:160, 1:640). The diagnostic significance of low titers (1:20–1:40) requires correlation with clinical findings and antigen-specific EIA results. High titers (>1:160) in the appropriate clinical context strongly support AAV.
- Anti-PR3 EIA: Typically reported as U/mL or AU/mL with a cut-off of approximately 3.5–7 U/mL depending on the platform (positive ≥ the laboratory's upper reference limit). Values >100 U/mL in a patient with glomerulonephritis are highly predictive of GPA or MPA.
- Anti-MPO EIA: Similar reporting. Positive results in the context of renal disease, pulmonary infiltrates, or constitutional symptoms should prompt urgent nephrology or rheumatology referral.
Sensitivity by disease state:
- Generalized GPA (active multiorgan): anti-PR3 sensitivity ~85–90%
- Localized GPA (upper airway only): anti-PR3 sensitivity ~50–65%
- MPA: anti-MPO sensitivity ~75–80%, anti-PR3 ~5–10%
- EGPA: anti-MPO ~30–40%, anti-PR3 ~5%
- Renal-limited ANCA vasculitis: anti-MPO ~75%, anti-PR3 ~25%
A negative ANCA does not exclude AAV in a patient with strong clinical features — particularly in localized GPA, early disease, or seronegative ANCA vasculitis (10–15% of AAV). Clinical and biopsy findings remain the gold standard.
False Positives and Mimics
The p-ANCA pattern on IIF is the greatest source of clinically misleading results because many conditions produce perinuclear staining without true MPO-directed autoantibodies:
Inflammatory Bowel Disease (IBD)
Both Crohn's disease and ulcerative colitis — particularly ulcerative colitis — are associated with a perinuclear ANCA pattern (sometimes called "atypical pANCA" or "xANCA"). These antibodies are directed against neutrophil lactoferrin, elastase, cathepsin G, and bactericidal/permeability-increasing protein rather than MPO. They are negative on anti-MPO EIA. The clinical significance of pANCA in IBD is debated; it does not indicate vasculitis but may be a marker of disease extent in UC.
Autoimmune Hepatitis
Atypical pANCA is reported in 50–85% of autoimmune hepatitis type 1 (AIH-1, anti-smooth muscle antibody positive). As with IBD-associated pANCA, the antigen is not MPO, and anti-MPO EIA is negative. The presence of elevated transaminases, gamma-globulin, and the characteristic autoantibody profile (ANA, ASMA) differentiates AIH from vasculitis.
Cocaine-Induced Midline Destructive Lesion (CIMDL)
Chronic cocaine inhalation causes midline facial destruction — saddle-nose deformity, septal perforation, palatal destruction — that mimics GPA clinically and radiographically. Crucially, cocaine is frequently adulterated with levamisole, a veterinary anthelmintic that induces anti-PR3-positive ANCA as well as anti-MPO-positive ANCA. A patient with midline facial destruction, systemic symptoms, and anti-PR3-positive ANCA who uses intranasal cocaine should be evaluated for CIMDL before diagnosing GPA. Clinical clues: agranulocytosis (levamisole effect), bilateral earlobe necrosis, positive cocaine metabolites in urine, anti-PR3-positive on EIA but with unusual antigen specificity (human neutrophil elastase) on detailed profiling.
Other Conditions
- Endocarditis: Can produce perinuclear ANCA pattern; may present with glomerulonephritis, mimicking MPA — distinguish with blood cultures and echocardiography.
- Antiphospholipid syndrome: May produce low-titer pANCA.
- Systemic lupus erythematosus: Can produce atypical pANCA; ANA and dsDNA help differentiate.
- Malignancy: Rare cause of ANCA positivity, usually at low titers.
Drug-Induced ANCA Vasculitis
A number of medications can induce ANCA production and frank ANCA vasculitis. Drug-induced ANCA vasculitis is a clinical diagnosis requiring medication exposure, ANCA positivity (typically anti-MPO), and evidence of vasculitis that resolves after drug discontinuation.
Propylthiouracil (PTU)
The antithyroid drug PTU carries the highest documented risk of ANCA induction. Up to 20–30% of patients on long-term PTU develop ANCA (predominantly anti-MPO, but also multi-ANCA with anti-PR3, anti-elastase, anti-lactoferrin). Approximately 1–5% develop frank vasculitis — glomerulonephritis, pulmonary infiltrates, cutaneous vasculitis. Methimazole induces ANCA vasculitis at far lower frequency.
Hydralazine
The antihypertensive hydralazine causes anti-MPO-positive ANCA vasculitis, typically after years of therapy and at higher cumulative doses. Presents with glomerulonephritis, arthralgias, and occasionally pulmonary-renal syndrome. Histone-reactive ANA (as in drug-induced lupus) may also be present.
Minocycline
Long-term minocycline for acne is associated with MPO-ANCA and drug-induced lupus-like syndrome. Discontinuation typically leads to clinical improvement.
Levamisole-Adulterated Cocaine
As detailed above under false positives, levamisole induces ANCA (anti-PR3 and anti-MPO), agranulocytosis, and vasculitis. This has become increasingly common as levamisole prevalence in the cocaine supply exceeds 70% in North America.
Other Implicated Drugs
Allopurinol, D-penicillamine, carbimazole, clozapine, and rifampicin have been reported in case series. The common final pathway is hapten-induced autoantibody generation or molecular mimicry with MPO.
Serial ANCA Monitoring for Disease Activity
One of the most clinically debated applications of ANCA testing is serial monitoring to predict relapse in patients in remission. The evidence is stronger for PR3-ANCA than MPO-ANCA:
PR3-ANCA and Relapse Prediction
Multiple prospective studies and the 2014 EUVAS (European Vasculitis Study Group) consensus indicate that a sustained rise in PR3-ANCA titer (typically ≥2-fold increase on two consecutive measurements, or conversion from negative to positive) is associated with an increased risk of relapse within 3–6 months. The positive predictive value of rising PR3-ANCA for relapse is approximately 57–80% depending on the study, meaning a rising titer should prompt clinical assessment and consideration of pre-emptive treatment escalation, but not automatic immunosuppression without clinical symptoms.
MPO-ANCA and Relapse Prediction
Anti-MPO titers are less reliably predictive of relapse than anti-PR3. MPO-ANCA levels may remain elevated in clinical remission without heralding relapse, and some patients relapse without preceding titer rise. Clinical symptoms, urinalysis (hematuria, casts), CRP, and creatinine remain essential monitoring tools alongside ANCA titers in MPO-ANCA disease.
Monitoring Protocol
Typical practice: ANCA testing every 3–6 months in remission, more frequently if symptoms emerge. Urinalysis with microscopy at every visit — the kidneys are the organ most vulnerable to subclinical relapse. Chest imaging for respiratory symptoms. Any combination of rising ANCA titer plus new clinical findings (hematuria, creatinine rise, new respiratory symptoms) should be evaluated promptly; immunosuppression should not be pre-emptively escalated based on titer rise alone without clinical correlation.
Key Research and Citations
- Jennette JC, Falk RJ, Bacon PA, et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1–11. PMID: 23045170
- Bossuyt X, Cohen Tervaert JW, Arimura Y, et al. Revised 2017 International Consensus on Testing of ANCAs in Granulomatosis with Polyangiitis and Microscopic Polyangiitis. Nat Rev Rheumatol. 2017;13(11):683–692. PMID: 28905856
- Specks U, Merkel PA, Seo P, et al. Efficacy of remission-induction regimens for ANCA-associated vasculitis. N Engl J Med. 2013;369(5):417–427. PMID: 23902481
- Zwerina J, Eger G, Englbrecht M, et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome) in childhood: a systematic literature review and clinical comparison with adult patients. Semin Arthritis Rheum. 2009;39(2):108–115. — Search PubMed
- Guillevin L, Pagnoux C, Karras A, et al. Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis. N Engl J Med. 2014;371(19):1771–1780. PMID: 25372085
- Stone JH, Merkel PA, Spiera R, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med. 2010;363(3):221–232. PMID: 20647199
- Falk RJ, Gross WL, Guillevin L, et al. Granulomatosis with polyangiitis (Wegener's): an alternative name for Wegener's granulomatosis. Arthritis Rheum. 2011;63(4):863–864. — Search PubMed
- Kemna MJ, Damoiseaux J, Austen J, et al. ANCA as a predictor of relapse: useful in patients with renal involvement but not in patients with nonrenal disease. J Am Soc Nephrol. 2015;26(3):537–542. — Search PubMed
- Haas M, Eustace JA. Immune complex deposits in ANCA-associated crescentic glomerulonephritis: a study of 126 cases. Kidney Int. 2004;65(6):2145–2152. — Search PubMed
- Wiesner O, Russell KA, Lee AS, et al. Antineutrophil cytoplasmic antibodies reacting with human neutrophil elastase as a diagnostic marker for cocaine-induced midline destructive lesions but not autoimmune vasculitis. Arthritis Rheum. 2004;50(9):2954–2965. — Search PubMed
- Niles JL, Böttinger EP, Saurina GR, et al. The syndrome of lung hemorrhage and nephritis is usually an ANCA-associated condition. Arch Intern Med. 1996;156(4):440–445. PMID: 8607730
- Hagen EC, Daha MR, Hermans J, et al. Diagnostic value of standardized assays for anti-neutrophil cytoplasmic antibodies in idiopathic systemic vasculitis. Kidney Int. 1998;53(3):743–753. PMID: 9507222
PubMed Search Links
- ANCA-associated vasculitis diagnosis and treatment
- Anti-PR3 and anti-MPO ANCA vasculitis relapse prediction
- Granulomatosis with polyangiitis ANCA
- Drug-induced ANCA vasculitis
- ANCA false positive IBD autoimmune hepatitis
Connections
- All Lab Tests
- ANA Test
- Urinalysis
- Creatinine / eGFR
- Complete Blood Count
- Complement C3 / C4
- Immunology Diseases
- Glomerulonephritis
- Vasculitis — the disease family this test diagnoses; anti-PR3 and anti-MPO define its ANCA-associated small-vessel subtypes.