AFP Test: Alpha-Fetoprotein Lab Guide
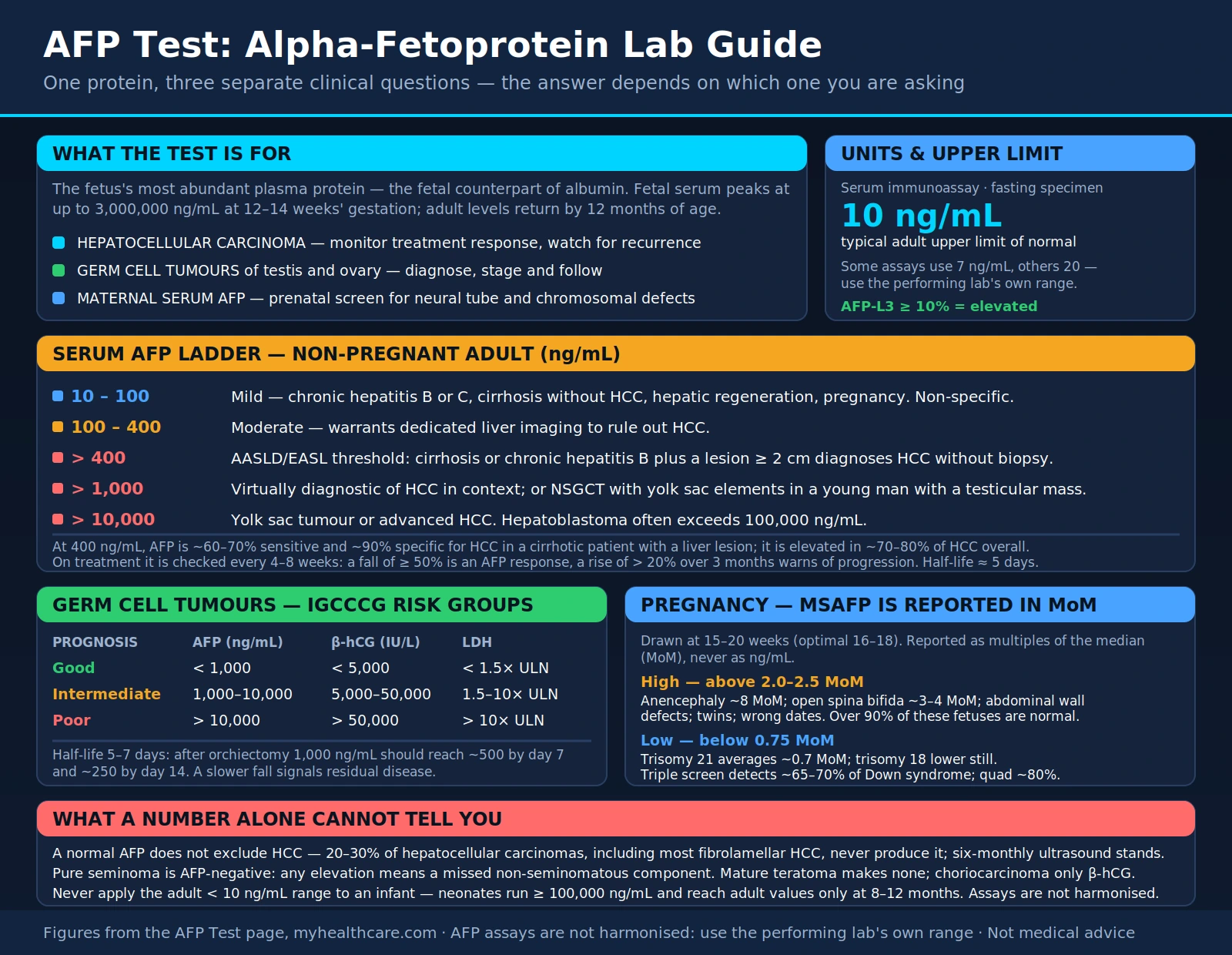
Table of Contents
- What is AFP?
- Biology and Normal Values
- AFP in Hepatocellular Carcinoma
- AFP in Germ Cell Tumors
- AFP in Pediatric Cancers
- Maternal Serum AFP and Prenatal Screening
- Monitoring Treatment Response
- Interpretation Pitfalls
- Research Papers
- Connections
- Featured Videos
What is AFP?
Alpha-fetoprotein (AFP) is the most abundant plasma protein in the developing human fetus, serving a role analogous to albumin in adults. The protein is synthesized primarily by the yolk sac and the fetal liver during gestation, reaching peak concentrations in fetal serum of up to 3 million ng/mL between 12 and 14 weeks of gestation. After birth, AFP levels fall sharply and by 12 months of age reach the very low levels seen throughout adult life — typically below 10 ng/mL. In healthy adults, tiny amounts of AFP continue to be produced by hepatocytes and gastrointestinal epithelial cells, but the quantities are too small to have any physiological significance.
AFP was first identified in 1956 by Bergstrand and Czar, who detected it in human fetal serum. The clinical significance of the protein took shape when Garri Abelev demonstrated in 1963 that AFP was produced by transplanted mouse hepatomas, and Yuri Tatarinov independently confirmed the finding in human liver cancer patients in 1964. That discovery launched AFP into clinical medicine as one of the earliest tumor markers used in oncology.
The AFP gene resides on chromosome 4q and belongs to the albuminoid gene superfamily, which also includes albumin, vitamin D-binding protein, and afamin. These proteins share structural homology and are thought to have evolved from a common ancestral gene through tandem duplication.
Today AFP serves three distinct clinical purposes: monitoring the treatment response and surveillance for recurrence in hepatocellular carcinoma (HCC); diagnosing, staging, and following germ cell tumors of the testis and ovary; and screening pregnancies for neural tube defects and chromosomal abnormalities through the maternal serum AFP (MSAFP) test. Understanding which context you are operating in is essential to interpreting any AFP result correctly.
Biology and Normal Values
AFP is measured by immunoassay from a serum sample. A single fasting specimen is standard practice, although AFP does not show significant diurnal variation and fasting is not strictly mandatory. Most clinical laboratories report a normal upper limit of 10 ng/mL, though some assays use 7 ng/mL and others use 20 ng/mL — always compare results to the reference range provided by the performing laboratory rather than applying a universal cutoff.
Mildly elevated AFP (10–100 ng/mL) is a common finding in chronic hepatitis (B or C), liver cirrhosis without HCC, active hepatocellular regeneration, and pregnancy. Benign GI conditions such as gastric cancer and pancreatitis can also cause mild elevations. This range is non-specific and requires clinical context.
Moderately elevated AFP (100–400 ng/mL) is more concerning. While still possible in very active hepatitis or advanced cirrhosis, values in this range warrant dedicated liver imaging to rule out HCC. In patients with cirrhosis and a liver lesion, AFP in this range strengthens the case for malignancy.
Markedly elevated AFP (>400 ng/mL) reaches the threshold used in the AASLD/EASL guidelines: in a high-risk patient (cirrhosis or chronic hepatitis B) with a liver lesion of 2 cm or larger on imaging, an AFP above 400 ng/mL is sufficient to diagnose HCC without a tissue biopsy. This non-invasive diagnostic pathway is unique to HCC among solid tumors.
Very high AFP (>1000 ng/mL) is virtually diagnostic of HCC in the appropriate clinical setting. In a young man with a testicular mass, very high AFP points to a non-seminomatous germ cell tumor (NSGCT) with yolk sac components. Values exceeding 10,000 ng/mL are most often seen in yolk sac tumors or advanced HCC.
AFP-L3 isoform: AFP exists in several glycoforms. The lectin-reactive fraction, AFP-L3, is preferentially produced by malignant hepatocytes. An AFP-L3 percentage of 10% or higher is considered elevated and increases the specificity of AFP for HCC relative to benign liver disease. AFP-L3 testing is available at reference laboratories and is particularly useful when total AFP is mildly or moderately elevated and the clinical picture is ambiguous.
AFP in Hepatocellular Carcinoma
Hepatocellular carcinoma is the most common primary liver cancer and ranks third among the leading causes of cancer death worldwide. Approximately 70–80% of HCC cases arise against a background of liver cirrhosis, with chronic hepatitis B and C infection and non-alcoholic fatty liver disease accounting for the majority of risk. AFP is the most widely used biomarker for HCC, but its clinical role has evolved considerably as imaging techniques have improved.
AFP is elevated in roughly 70–80% of HCC patients overall. However, about 20–30% of HCC cases — particularly early-stage tumors and the fibrolamellar variant — have a normal AFP throughout their entire course. This means AFP cannot be used as a standalone screening tool; liver ultrasound every six months, with or without AFP, remains the standard surveillance strategy recommended by AASLD for patients with cirrhosis or chronic hepatitis B.
At the 400 ng/mL diagnostic threshold, AFP has a sensitivity of approximately 60–70% and specificity of around 90% for HCC in patients with cirrhosis and a liver lesion on imaging. In practice, the test is most valuable when used alongside imaging findings rather than in isolation.
AFP also carries prognostic weight in the transplant setting. Pre-transplant AFP above 400 ng/mL is associated with poor post-transplant outcomes and may disqualify patients from listing at some centers. The AFP-based Metroticket 2.0 score incorporates AFP trajectory alongside tumor size and number to refine transplant candidate selection beyond the classic Milan criteria.
Several pivotal clinical trials have used AFP as both an enrollment criterion and an outcome measure. The REACH-2 trial (Zhu 2019, PMID 29498428) was the first biomarker-selected HCC trial, enrolling only patients with AFP 400 ng/mL or higher. Ramucirumab, an anti-VEGFR-2 antibody, demonstrated improved overall survival in this population (hazard ratio 0.71), establishing AFP ≥400 as a predictive biomarker for ramucirumab benefit in second-line HCC. The RESORCE trial (Llovet 2016, PMID 27584541) evaluated regorafenib for HCC progressing on sorafenib; AFP-based subgroup analyses showed differential benefit patterns by baseline AFP level.
During treatment with systemic agents or locoregional therapies, AFP is measured every 4–8 weeks. A decrease of 50% or more from baseline qualifies as a partial response by AFP criteria under the 2010 Lencioni amendment to mRECIST. A rising AFP — particularly a rise of more than 20% over 3 months — is an early warning of tumor progression and should trigger repeat imaging even if the scheduled interval has not elapsed. After surgical resection or ablation, AFP normalization within the expected timeframe (accounting for the protein's half-life of approximately 5 days) is a favorable prognostic sign; persistent AFP elevation strongly suggests residual disease.
AFP in Germ Cell Tumors
Germ cell tumors (GCTs) of the testis and, less commonly, the ovary represent the second major clinical domain for AFP measurement. Unlike in HCC, where AFP alone is insufficient for diagnosis, AFP plays a central and sometimes definitive role in staging, prognosis, and ongoing monitoring of these tumors.
Yolk sac tumor (endodermal sinus tumor) is the AFP-producing subtype par excellence, with markedly elevated AFP — often exceeding 10,000 ng/mL and occasionally reaching millions. These are the most AFP-active tumors in the body outside of the fetal liver.
Embryonal carcinoma produces moderate AFP elevations and also secretes beta-hCG. Mature teratoma does not produce AFP. Choriocarcinoma produces beta-hCG exclusively and has a normal AFP. Understanding these distinctions is critical for histological correlation.
Pure seminoma is AFP-negative. This is one of the most clinically important AFP rules: if a patient has a testicular mass histologically diagnosed as pure seminoma but AFP is elevated, the biopsy has missed a non-seminomatous component. Such patients must be managed as mixed NSGCT with BEP (bleomycin, etoposide, cisplatin) chemotherapy rather than surveillance or radiation — a difference that profoundly changes treatment. Any AFP elevation in a patient with apparent seminoma should trigger re-evaluation of the pathology.
AFP is measured alongside beta-hCG and lactate dehydrogenase (LDH) before orchiectomy and at defined intervals afterward. Together, these three markers form the backbone of the IGCCCG (International Germ Cell Cancer Collaborative Group) prognostic classification for NSGCT:
- Good prognosis: AFP <1,000 ng/mL, beta-hCG <5,000 IU/L, LDH <1.5× upper limit of normal (ULN)
- Intermediate prognosis: AFP 1,000–10,000 ng/mL, beta-hCG 5,000–50,000 IU/L, or LDH 1.5–10× ULN
- Poor prognosis: AFP >10,000 ng/mL, beta-hCG >50,000 IU/L, or LDH >10× ULN
The half-life of AFP is 5–7 days. After orchiectomy, AFP should decline along this expected curve. If AFP falls more slowly than this half-life predicts — a "plateau" or slow decline — residual disease or occult metastases are likely. During BEP chemotherapy, serial AFP measurements every 1–2 cycles track response; a plateau or rising AFP during treatment signals chemotherapy failure and usually triggers a change to salvage regimens such as TIP or VIP.
AFP in Pediatric Cancers
Hepatoblastoma is the most common primary liver tumor of childhood, accounting for the majority of pediatric liver malignancies. AFP is elevated in approximately 90% of hepatoblastoma cases, often dramatically so — values above 100,000 ng/mL are not unusual and values in the millions have been reported. AFP is used both to confirm the diagnosis and to guide treatment: serial AFP measurements during preoperative chemotherapy (typically PLADO or SIOPEL regimens) track tumor response, and AFP normalization after surgical resection confirms complete removal. Failure of AFP to normalize after surgery is a reliable indicator of residual or metastatic disease and drives decisions about re-resection, additional chemotherapy, or transplant evaluation.
A critical caveat in pediatric oncology: AFP is physiologically extremely elevated at birth. Neonates have AFP values that can reach 100,000 ng/mL or higher, reflecting the protein's normal fetal biology. AFP declines steadily through infancy and reaches adult normal values by approximately 8–12 months of age. Applying the adult reference range (<10 ng/mL) to infants under six months will generate false-positive results. Pediatric laboratories use age-matched reference ranges — this is non-negotiable for correct interpretation.
Pediatric germ cell tumors arising at extragonadal sites — sacrococcygeal teratoma, mediastinal GCT, and intracranial GCT — behave similarly to adult testicular GCTs with respect to AFP. Yolk sac subtypes produce markedly elevated AFP, and serial measurement monitors response to chemotherapy (typically BEP) and surgical outcomes.
AFP is NOT elevated in Wilms tumor (nephroblastoma) or neuroblastoma — two other common pediatric solid tumors. This distinction is helpful in the differential diagnosis when imaging locates a large abdominal mass in a young child: an elevated AFP points toward hepatoblastoma or sacrococcygeal GCT rather than Wilms tumor or neuroblastoma, narrowing the workup significantly before tissue is obtained.
Maternal Serum AFP and Prenatal Screening
The third major clinical application of AFP is in prenatal medicine, where maternal serum AFP (MSAFP) serves as a critical screening tool for fetal neural tube defects and chromosomal abnormalities. MSAFP is measured between 15 and 20 weeks of gestation, with the optimal window at 16–18 weeks. Because AFP levels change rapidly across gestation, all results are expressed as multiples of the median (MoM) — a gestational-age–adjusted value — rather than as absolute ng/mL concentrations. The MoM is further corrected for maternal weight, race, insulin-dependent diabetes status, and number of fetuses.
Elevated MSAFP (>2.0–2.5 MoM) raises concern for several conditions:
- Open neural tube defects: In anencephaly, MSAFP is typically around 8 MoM. Open spina bifida (myelomeningocele) elevates MSAFP to approximately 3–4 MoM. The mechanism is leakage of fetal AFP from exposed neural tissue into the amniotic fluid and then across the placental membrane into maternal blood.
- Abdominal wall defects: Gastroschisis and omphalocele allow fetal AFP to leak directly into amniotic fluid, elevating MSAFP.
- Twin pregnancy: Two fetuses produce more AFP, elevating the maternal level; MoM adjustment for twin gestation is essential.
- Fetal demise or incorrect dating: Inaccurate gestational age assignment is one of the most common explanations for an apparently elevated MSAFP in a normal pregnancy; confirming dates by ultrasound before acting on the result is standard practice.
Low MSAFP (<0.75 MoM) is associated with chromosomal abnormalities:
- Down syndrome (trisomy 21): MSAFP averages approximately 0.7 MoM in affected pregnancies, reflecting the smaller-than-expected fetus and placenta.
- Trisomy 18: Very low MSAFP combined with low beta-hCG and low uE3 characterizes the trisomy 18 pattern on the triple screen.
- Molar pregnancy: Markedly elevated beta-hCG but low AFP, given the absence of a normal fetus.
MSAFP is used as part of multi-marker screening panels. The triple screen combines MSAFP, beta-hCG, and unconjugated estriol (uE3) and detects approximately 65–70% of Down syndrome cases. The quad screen adds inhibin A as a fourth marker and improves Down syndrome detection to approximately 80% at a 5% false-positive rate. An abnormal MSAFP result on its own is not diagnostic of any condition — it is a screening flag that triggers the next step, which is a detailed anatomic ultrasound and, when indicated, amniocentesis for fetal karyotyping and amniotic fluid AFP measurement.
A crucial communication point for patients: more than 90% of pregnancies with elevated MSAFP have a normal fetus. The most common causes are incorrect dates, twins, or unexplained biological variation. Parents should understand that a positive screen result means further evaluation is needed, not that something is definitely wrong.
Monitoring Treatment Response
Across all three major clinical domains, AFP functions as a dynamic biomarker — its trajectory over time is often more informative than any single value.
Hepatocellular carcinoma: AFP is measured at diagnosis to establish a baseline, then every 4–8 weeks during systemic therapy (sorafenib, lenvatinib, atezolizumab-bevacizumab, or second-line agents). A decrease of 50% or more from baseline constitutes an AFP response by modified RECIST criteria. After hepatic resection, AFP is measured at 3 and 6 months to confirm normalization — the expected half-life of AFP means that values should fall by half approximately every 5 days after complete tumor removal. Following liver transplantation for HCC, AFP surveillance continues every 6 months; a rising AFP often precedes radiological evidence of recurrence by weeks to months and permits earlier salvage intervention.
Non-seminomatous germ cell tumors: AFP (along with beta-hCG and LDH) is measured pre-operatively to establish the baseline and post-orchiectomy every 1–2 weeks during active treatment and then every 1–3 months during surveillance. During BEP chemotherapy, AFP should decline in a log-linear fashion consistent with the 5–7 day half-life. A plateau — where AFP stops declining and stabilizes at an elevated level — is a critical signal. It typically means viable tumor remains despite chemotherapy, and is one of the primary indications to consider salvage chemotherapy or residual mass resection. AFP normalization after chemotherapy and any necessary post-chemotherapy surgery is a prerequisite for declaring a complete biochemical response.
Pediatric hepatoblastoma: AFP is measured before each cycle of chemotherapy (typically PLADO: cisplatin and doxorubicin, per the SIOPEL protocol). A 1-log or greater decline in AFP per chemotherapy cycle is expected with effective treatment. The AFP level at the time of surgery is a key determinant of respectability: very high residual AFP may indicate active tumor not fully controlled by preoperative chemotherapy, warranting re-assessment before proceeding to resection. Postoperatively, AFP should reach the age-appropriate normal range within weeks to months if the resection is complete.
Interpretation Pitfalls
Normal AFP does not exclude HCC. Approximately 20–30% of hepatocellular carcinomas, including most fibrolamellar HCC cases, produce little to no AFP. Fibrolamellar HCC is a distinct variant affecting young adults without underlying cirrhosis; it is AFP-negative in the vast majority of cases and is diagnosed on imaging characteristics and histology. Surveillance ultrasound every 6 months remains mandatory for at-risk patients regardless of AFP results.
Falsely elevated AFP in benign liver disease. Active hepatitis B or C flares, liver cirrhosis, and hepatic regeneration can elevate AFP to 100–200 ng/mL without any malignancy. Distinguishing benign elevation from early HCC in a cirrhotic patient with AFP in the 50–200 ng/mL range is one of the most common and difficult interpretive challenges in clinical practice. AFP-L3 percentage, gadolinium-enhanced MRI or contrast-enhanced CT using LI-RADS criteria, and trend monitoring over serial measurements are all tools used to resolve this ambiguity.
The AFP pure-seminoma trap. As noted above, any AFP elevation in a patient with histological "pure seminoma" should be treated as a mixed NSGCT until proven otherwise. This is not a rare scenario — sampling error and histological heterogeneity in mixed tumors mean that the first biopsy may not represent all components of a mixed tumor.
Post-orchiectomy half-life check. If AFP falls more slowly than the expected 5–7 day half-life after orchiectomy, this is a marker-decline rate that warrants concern. A simple calculation: if pre-surgical AFP is 1000 ng/mL, after 7 days it should be approximately 500 ng/mL, after 14 days approximately 250 ng/mL. Values substantially above these expected levels suggest incomplete surgical resection or occult metastatic disease producing ongoing AFP.
Neonatal and infant AFP — never use adult reference ranges. AFP is physiologically in the tens of thousands of ng/mL at birth. The adult threshold of 10 ng/mL is completely inapplicable to infants under six months and meaningless in neonates. Using age-matched neonatal reference curves is essential; many laboratory information systems do not automatically flag the need for age-appropriate interpretation, so clinicians must apply this corrective step manually.
Assay differences between laboratories. AFP immunoassays are not harmonized across platforms. Values from one laboratory may not be directly comparable to values from another. When following AFP trends over time — particularly in oncology patients — testing at the same laboratory using the same platform ensures that changes reflect true biological changes rather than assay differences.
Research Papers
- Abelev GI. Production of embryonal serum alpha-globulin by hepatomas. Review of experimental and clinical data. Cancer Res. 1968. — Search PubMed
- Ruoslahti E, Seppälä M. Studies of carcino-fetal proteins. III. Development of a radioimmunoassay for alpha-fetoprotein. Int J Cancer. 1971. — Search PubMed
- Bruix J, Sherman M; Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005. — Search PubMed
- Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011. — Search PubMed
- Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased AFP concentrations (REACH-2). Lancet Oncol. 2019. — Search PubMed
- Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma (SHARP trial). N Engl J Med. 2008. — Search PubMed
- International Germ Cell Cancer Collaborative Group. International Germ Cell Consensus Classification: a prognostic factor-based staging system. J Clin Oncol. 1997. — Search PubMed
- Woodward PJ, Heidenreich A, Looijenga LH, et al. Testicular germ cell tumours: serum tumor markers. In: WHO Classification of Tumours of the Urinary System. 2002. — Search PubMed
- Wald NJ, Cuckle HS, Densem JW, et al. Maternal serum screening for Down's syndrome in early pregnancy. BMJ. 1988. — Search PubMed
- Brock DJ, Barron L, Jelen P, et al. Maternal serum alpha-fetoprotein measurements as an early indicator of low birthweight. Lancet. 1982. — Search PubMed
- Meister B, Gassner I, Streif W, et al. Alpha-fetoprotein as a tumor marker in children with hepatoblastoma. Pediatr Blood Cancer. 2012. — Search PubMed
- Vogel A, Meyer T, Sapisochin G, et al. Hepatocellular carcinoma. Lancet. 2022. — Search PubMed
Connections
- All Lab Tests
- CEA Test
- CA-125 Test
- PSA Test
- Comprehensive Metabolic Panel
- Liver Function Tests
- Liver Disease
- Hepatitis B
- Hepatitis C
- Testicular Cancer