Coriander Seeds & Heavy Metal Chelation (Honest Evidence Review)
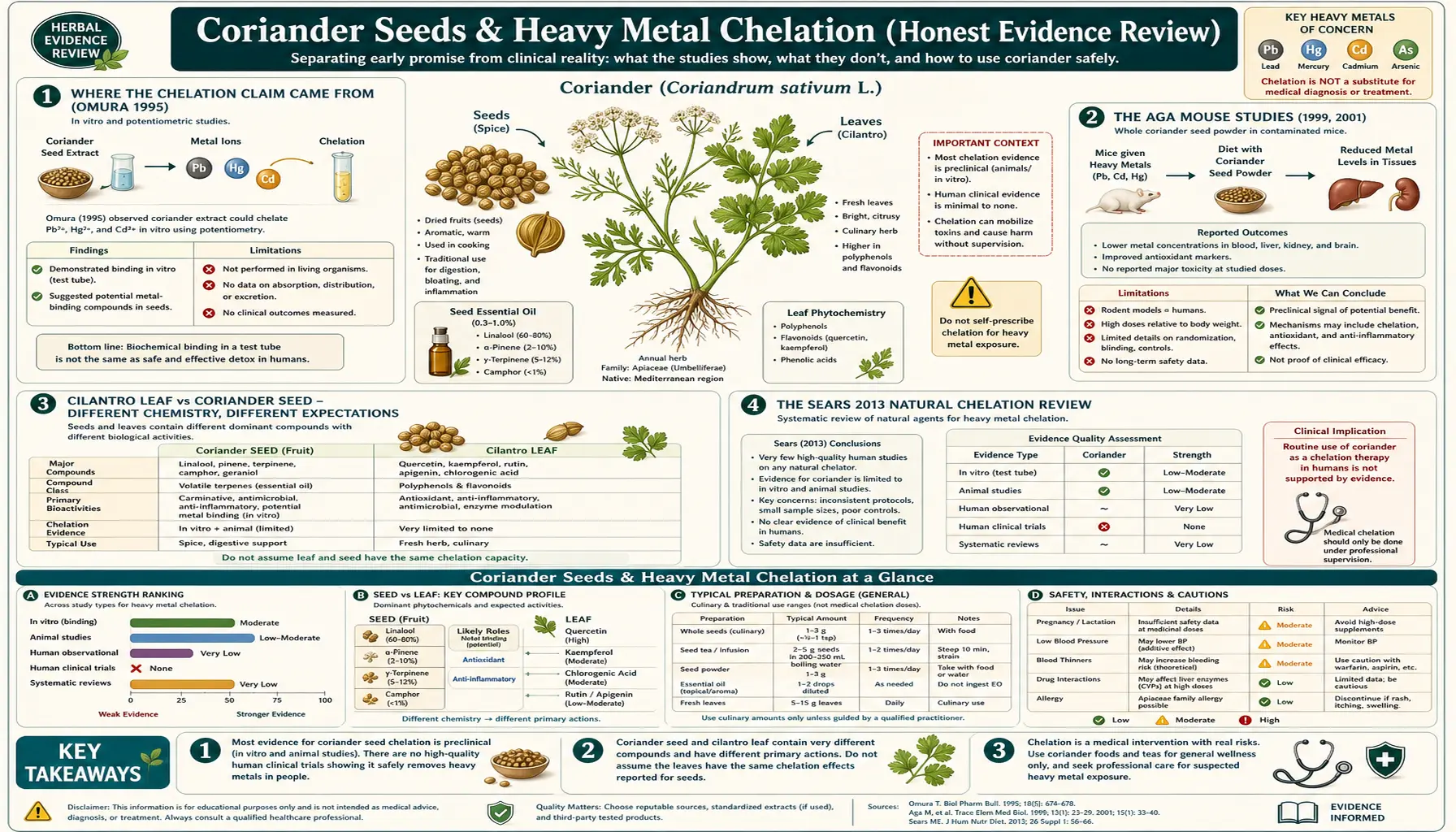
The claim that coriander (most often the leaf, sold as cilantro) chelates heavy metals — mercury, lead, aluminum, arsenic — and accelerates their excretion from the human body is one of the most widely circulated assertions in alternative medicine. It anchors many "natural detox" protocols, dental amalgam removal regimens, and post-vaccine "metal cleanses." The honest scientific reading is less dramatic. The original 1995 Omura case-series report on dental-amalgam mercury elimination is anecdotal and not properly controlled. The Aga and colleagues 1999 and 2001 mouse studies are real, peer-reviewed, and worth taking seriously — they show that pre-treatment with coriander reduces tissue deposition of lead and possibly mercury in mice. The Sears 2013 review acknowledged coriander among "natural chelation" candidates but explicitly noted the absence of any properly controlled human RCT. Three decades after Omura's paper, there is still no head-to-head clinical trial of coriander versus placebo or versus standard chelators (DMSA, DMPS, EDTA) for measured heavy-metal excretion in humans. This deep-dive lays out exactly what the literature does and does not support, why cilantro leaf chemistry differs from coriander seed chemistry, and how to think about the role (if any) of culinary coriander within a documented heavy-metal-toxicity workup.
Table of Contents
- Where the Chelation Claim Came From (Omura 1995)
- The Aga Mouse Studies (1999, 2001)
- Cilantro Leaf vs Coriander Seed — Different Chemistry
- The Sears 2013 Natural Chelation Review
- What Real Medical Chelation Actually Looks Like (DMSA, DMPS, EDTA)
- The Coriander + Chlorella Combination Claim
- The "Provoked Urine Test" Trap
- When Heavy Metal Toxicity is Actually Documented
- What Coriander Is Genuinely Good For (Not Chelation)
- Cautions and Patient Counseling
- Key Research Papers
- Connections
- Featured Videos
Where the Chelation Claim Came From (Omura 1995)
The popular claim that cilantro / coriander chelates heavy metals can be traced largely to a 1995 case series by Yoshiaki Omura published in the journal Acupuncture & Electro-Therapeutics Research. Omura, a Japanese physician practicing in New York, reported that patients undergoing removal of dental amalgam fillings showed elevated urinary mercury for several weeks, and that adding "Chinese parsley" (cilantro) to their diet appeared to accelerate the urinary mercury excretion and to clear what Omura described using his proprietary "Bi-Digital O-Ring Test" as residual mercury deposits in various organs.
The methodological problems with the Omura report are substantial. The "Bi-Digital O-Ring Test" is a form of applied kinesiology / muscle testing that has no validated reproducibility under blinded conditions and is not accepted in mainstream diagnostic medicine. The case series had no proper control group, no blinding, no pre-specified outcome measures, and a small heterogeneous patient population. Urinary mercury excretion is highly variable day to day depending on hydration, recent fish intake, and prior amalgam disturbance — the modest changes Omura reported are well within normal individual variation. The paper was not published in a major mainstream toxicology journal.
Despite these limitations, the Omura paper was widely cited in the alternative-medicine community as foundational evidence for cilantro chelation. It was integrated into the Cutler protocol for chronic mercury toxicity, into the popular Klinghardt protocol for dental amalgam removal, and into countless "natural detox" books and websites. The claim escaped into the mainstream wellness culture and is now widely repeated in social media and consumer health content with no acknowledgment that the primary evidence is a single unblinded case series using an unvalidated diagnostic method.
The Aga Mouse Studies (1999, 2001)
More credible evidence exists in two peer-reviewed mouse studies by Aga and colleagues published in Journal of Health Science in 1999 and in Journal of Ethnopharmacology in 2001. These are real laboratory experiments with proper controls, blinded measurements of tissue metal content, and published in mainstream pharmacology / toxicology venues.
The 2001 study (cited most often) examined ICR mice given lead acetate orally and then treated with either water-control, EDTA (positive-control chelator), or aqueous extract of Coriandrum sativum (Chinese parsley) leaf. The mice were sacrificed and tissue lead concentrations were measured in bone, liver, kidney, brain, and intestine. Headline findings:
- Coriander treatment reduced lead deposition in the femur (bone), brain, and kidney compared with the lead-only control group
- The magnitude of the effect was smaller than the EDTA positive control but statistically significant
- Coriander appeared to be more effective when given before the lead exposure than after, suggesting a possible role in interfering with intestinal absorption rather than removing already-deposited metal
- No obvious toxicity from coriander treatment at the doses used
The earlier 1999 study reported similar reductions in mercury deposition in mice treated with coriander, although the mercury data has been less consistently replicated. A subsequent 2004 study by Sharma and colleagues using a different mouse model found more equivocal results.
What the mouse data actually supports:
- There is some biological plausibility for coriander affecting heavy-metal kinetics in mice.
- The effect is most pronounced for lead, somewhat less consistent for mercury, and essentially untested for arsenic, cadmium, and aluminum.
- The effect appears largest when coriander is given before metal exposure (a "blocking absorption" mechanism rather than true chelation of stored metal).
- The mechanism remains unclear at the molecular level — no specific chelating compound in coriander has been isolated and characterized at the rigor seen for synthetic chelators.
- Mouse data does not reliably translate to human therapeutic dosing or clinical outcomes.
What the mouse data does not support: that consuming culinary amounts of cilantro or coriander seed in humans produces clinically meaningful reductions in stored body burden of mercury, lead, or other metals. That clinical translation requires human trials that have not been done.
Cilantro Leaf vs Coriander Seed — Different Chemistry
A point routinely conflated in popular coverage: the chelation claims in the Omura paper and the Aga studies all involved cilantro leaf (the fresh herb, also called Chinese parsley or coriander leaf), not coriander seed (the dried, ripe fruits used as a culinary spice). The chemistry of the two is substantially different.
The leaf chemistry is dominated by long-chain aliphatic aldehydes — decanal, (E)-2-decenal, (E)-2-dodecenal, and related saturated and unsaturated C8-C12 aldehydes. These compounds are responsible for the leaf's characteristic flavor (which roughly 14% of the human population finds soapy or offensive due to a polymorphism in the OR6A2 olfactory receptor gene) and have been credited with the leaf's antimicrobial activity. The proposed metal-binding mechanism in the leaf has been attributed variably to:
- Aldehyde groups that could potentially form Schiff bases with metal-bound amino acids
- Sulfur-containing volatile compounds at trace levels
- The polyphenol fraction (quercetin, kaempferol, rutin)
- Mucilage and dietary fiber that bind metal in the gut lumen and reduce reabsorption
None of these proposed mechanisms has been definitively validated. The seed chemistry, by contrast, is dominated by the monoterpene alcohol linalool, with smaller fractions of alpha-pinene, gamma-terpinene, geraniol, and camphor — a profile much closer to lavender or basil than to the leaf. The aldehydes that dominate the leaf are present at much lower concentrations in the seed.
The practical implication: the popular chelation claim, to the extent it has any animal-study support, is largely a leaf claim, not a seed claim. Products sold as coriander seed extract or coriander seed oil are unlikely to provide the leaf's aldehyde fraction in meaningful amounts. If someone wishes to attempt the experiment based on the mouse data, fresh cilantro leaf (the whole herb, not the dried seed) is the form that the Omura and Aga work actually used.
For the seed itself, the credible benefit claims center on digestive carminative use, hypoglycemic activity, and food-safety antimicrobial preservation. Heavy-metal chelation is not a credible standalone seed claim.
The Sears 2013 Natural Chelation Review
The most commonly cited modern review of natural chelation candidates is Sears (2013) in The Scientific World Journal titled "Chelation: harnessing and enhancing heavy metal detoxification — a review." Sears surveyed the published evidence for several natural agents claimed to chelate or otherwise reduce body burden of heavy metals, including coriander, chlorella, garlic, modified citrus pectin, alpha-lipoic acid, glutathione precursors (NAC), and others.
The honest summary of what Sears actually concluded:
- Coriander has biological plausibility based on the Aga mouse studies and a small number of in-vitro binding studies
- No properly controlled human RCT exists for coriander as a chelator
- The effect size, even if real, is likely modest compared with pharmaceutical chelators
- Coriander is safe enough to consume as food, so the risk-benefit calculus is reasonable for inclusion in a broader detoxification approach in an individual who wishes to do so
- It should not be used as a substitute for pharmaceutical chelation in documented clinical toxicity
The Sears review is frequently cited in popular literature as validation of cilantro chelation, but a careful reading shows it is more an inventory of candidate natural agents with biological plausibility than an endorsement of clinical efficacy. The repeated note that proper human RCTs do not exist is the central caveat.
What Real Medical Chelation Actually Looks Like (DMSA, DMPS, EDTA)
For comparison, what does properly evidence-based medical chelation look like? There are three commonly used pharmaceutical chelators in mainstream clinical toxicology:
- DMSA (meso-2,3-dimercaptosuccinic acid, brand Chemet) — oral chelator, FDA-approved for childhood lead poisoning at blood lead >45 mcg/dL. Dosed at 10 mg/kg every 8 hours for 5 days, then every 12 hours for 14 days. Pharmacokinetics, dose-response, and excretion are well-characterized. Used off-label for mercury toxicity.
- DMPS (2,3-dimercapto-1-propanesulfonic acid, brand Dimaval) — oral or IV chelator, not FDA-approved in the US but used in Europe and available via compounding pharmacies. Particularly favored for mercury, including dental amalgam mercury elimination.
- CaNa2-EDTA (calcium disodium ethylenediaminetetraacetic acid) — IV chelator, FDA-approved for severe acute lead poisoning. Dosed at 1,000-1,500 mg/m²/day for 5 days. Risk of nephrotoxicity, requires monitoring.
- BAL (British anti-Lewisite, dimercaprol) — older intramuscular chelator, used for acute arsenic, gold, mercury, and lead poisoning, particularly when oral chelation is not feasible. Painful injection, significant side-effect profile.
- Deferoxamine, deferasirox, deferiprone — iron-specific chelators for transfusion-dependent iron overload (thalassemia, sickle cell disease).
These agents have molar-equivalent metal-binding constants in the range of 10^15 to 10^25, characterized by formal stability constant measurements. They have been studied in formal pharmacokinetic, pharmacodynamic, and toxicity studies in humans. Their efficacy is measured by quantitative reduction in blood, urine, tissue, and bone metal burden using validated atomic absorption or ICP-MS analytical methods. They are administered under physician supervision with laboratory monitoring.
Coriander, even in the most optimistic reading of the Aga mouse data, does not approach this level of evidence or this level of effect size. Substituting culinary coriander for properly indicated medical chelation in a patient with documented clinically significant heavy metal toxicity is potentially dangerous because it delays effective treatment.
The Coriander + Chlorella Combination Claim
A common variation on the chelation theme is the Klinghardt-attributed protocol pairing cilantro (the proposed "mobilizer" of stored mercury) with chlorella (the proposed "binder" that supposedly prevents reabsorption from the gut). The underlying logic is that cilantro draws mercury out of intracellular storage into the bloodstream, and chlorella in the gut binds the biliary-secreted mercury before it can be reabsorbed in the enterohepatic circulation.
The evidence base for this specific combination protocol is weaker than the evidence base for either component individually. There are no peer-reviewed RCTs of the combination. Chlorella does contain peptides and cell-wall components that bind metals in vitro, and animal studies have shown reduced cadmium and lead absorption when chlorella is co-administered with the metal. The proposed clinical translation to chronic stored body burden in humans is, again, not validated.
If a patient is pursuing this protocol on their own initiative, the honest counseling points are:
- The protocol is safe as long as the cilantro is genuine fresh herb (washed; no agricultural contamination risk) and the chlorella product is from a clean-water source with third-party heavy-metal testing (some pond-grown chlorella products are themselves contaminated with the metals they purport to remove)
- Magnitude of clinical effect is unknown and likely modest if any
- If symptoms attributed to heavy metal toxicity persist, proper toxicologic workup with blood/urine metals and consideration of medical chelation is more likely to be effective
- The protocol is not a substitute for removing the ongoing exposure (amalgam fillings, contaminated drinking water, occupational exposure)
The "Provoked Urine Test" Trap
A common pattern in clinics offering chelation therapy is the "provoked urine test" — a patient is given a single dose of DMSA, DMPS, or EDTA, then provides a 6-hour or 24-hour urine sample which is sent to a lab for heavy-metal quantification. Because the chelator pulls metals into urine that would otherwise have been excreted only slowly, the provoked urine inevitably shows higher metal values than an unprovoked baseline urine.
The patient is then told that this elevated provoked urine level represents stored body burden of toxic metal that requires further chelation therapy. The problem: the reference ranges quoted by these labs are typically unprovoked reference ranges. Of course a provoked urine will exceed an unprovoked reference range. The American College of Medical Toxicology, the American Academy of Clinical Toxicology, and the CDC have all issued position statements rejecting provoked urine testing as a valid clinical tool for assessing chronic heavy-metal toxicity. The proper assessment uses whole-blood levels for lead and mercury, with consideration of hair and tissue analysis in specific clinical scenarios.
Coriander does not directly cause this diagnostic pitfall, but the broader "natural detox" framing in which the cilantro chelation claim sits often leads patients into chelation clinics that use provoked urine testing as the entry point. Patient counseling should clearly separate the in-vitro/animal evidence for coriander (interesting but inconclusive) from the misuse of provoked-urine testing (genuinely misleading and potentially harmful by driving unnecessary chelation in patients with no actual toxicity).
When Heavy Metal Toxicity is Actually Documented
Some patients do have genuine, clinically significant heavy-metal toxicity that warrants formal investigation and treatment. The common scenarios:
- Childhood lead poisoning from pre-1978 paint, contaminated soil, contaminated drinking water (Flint, Michigan), or imported folk remedies (Greta, Azarcon)
- Occupational lead exposure — battery workers, smelter workers, demolition workers, lead glaziers, stained-glass artists
- Methylmercury from large predatory fish — swordfish, tilefish, king mackerel, large tuna; particularly relevant in high-consumption populations and during pregnancy
- Elemental mercury exposure from broken thermometers, fluorescent tube breakage, dental amalgam disturbance, or rare occupational exposures
- Arsenic from contaminated well water — particularly in parts of Bangladesh, India, parts of the American Southwest, and some private well water
- Cadmium from cigarette smoking and from occupational exposure (pigment workers, battery workers)
The appropriate workup for suspected toxicity is:
- Detailed exposure history (occupational, residential, dietary, recreational, medical)
- Whole-blood lead and mercury (NOT provoked urine)
- Hair and 24-hour unprovoked urine in specific scenarios
- Tissue biopsy in rare cases (e.g. bone lead via X-ray fluorescence in chronic occupational exposure)
- Pediatric Environmental Health Specialty Unit (PEHSU) consultation for children
- Adult medical toxicology consultation for occupational or unusual exposures
- Pharmaceutical chelation if blood levels exceed treatment thresholds (e.g. blood lead >45 mcg/dL in children)
Coriander, cilantro, and other "natural chelators" are not part of the recommended workup or treatment for clinically significant toxicity. They are not harmful in food amounts and may be consumed without restriction during a proper medical chelation program if a patient finds them culturally or psychologically valuable, but they are not a substitute for evidence-based care.
What Coriander Is Genuinely Good For (Not Chelation)
The evidence base supports coriander seed for several genuine clinical applications — just not the heavy-metal one for which it is most famous in popular wellness culture. Stronger-evidence indications include:
- Carminative for IBS and functional dyspepsia — placebo-controlled trial evidence (Vejdani 2006), well-characterized mechanism through linalool calcium-channel modulation and GABA-A potentiation
- Mild hypoglycemic / glucose-lowering activity — mouse studies (Gray 1999) and small human pilots showing modest fasting glucose reduction
- Broad-spectrum antimicrobial for food-safety preservation — extensive in-vitro data against Salmonella, E. coli, Listeria, Candida
- Mild anxiolytic and sleep-supportive effect — via the linalool / GABA-A mechanism (Emamghoreishi 2005 mouse data)
- Antioxidant capacity from the flavonoid fraction (quercetin, kaempferol, rutin)
- Bioavailability enhancement of other phytochemicals when combined in traditional South Asian spice blends
The takeaway: coriander seed is genuinely useful in the herbal toolkit. It is unfortunate that its most-marketed benefit (heavy-metal chelation) is also its least-supported. Consumers and clinicians should redirect attention to the better-evidenced uses.
Cautions and Patient Counseling
- Do not delay proper toxicology workup if a patient suspects heavy-metal toxicity. The greatest risk of the cilantro-chelation narrative is not direct harm from coriander itself but rather delay of evidence-based diagnosis and treatment.
- Be wary of provoked urine tests as a basis for chelation referral. These tests overestimate body burden and drive unnecessary chelation in patients who do not have clinically significant exposure.
- Remove ongoing exposure first — no detox protocol of any kind can succeed if exposure continues. This includes evaluating drinking-water quality (lead from old pipes, arsenic from well water), occupational exposures, dietary mercury (large predatory fish), and lead-based folk remedies.
- Chlorella product quality matters — if combining with chlorella, use products with third-party heavy-metal testing from clean-water sources. Some chlorella products are themselves contaminated.
- Pregnancy — if heavy-metal exposure is suspected during pregnancy (lead, methylmercury), obstetric and toxicology consultation is required. Cilantro/coriander in culinary amounts is safe in pregnancy; supplemental extract use during documented exposure should not delay proper assessment.
- Children — if a child is suspected to have lead poisoning, immediate blood lead testing through the pediatrician or local public health department is the proper first step. Cilantro is not a substitute.
- Hypoglycemia in diabetic patients — high-dose coriander supplementation (not culinary amounts) can additively lower blood glucose in patients taking insulin or sulfonylureas.
Key Research Papers
- Aga M, Iwaki K, Ueda Y, Ushio S, Masaki N, Fukuda S, et al. (2001). Preventive effect of Coriandrum sativum (Chinese parsley) on localized lead deposition in ICR mice. Journal of Ethnopharmacology. — PubMed
- Omura Y, Beckman SL (1995). Role of mercury (Hg) in resistant infections & effective treatment of Chlamydia trachomatis and Herpes family viral infections (and potential treatment for cancer) by removing localized Hg deposits with Chinese parsley. Acupuncture & Electro-Therapeutics Research. — PubMed
- Sears ME (2013). Chelation: harnessing and enhancing heavy metal detoxification — a review. The Scientific World Journal. — PubMed
- Charlton NP, Lawrence DT, Brady WJ, Kirk MA, Holstege CP (2009). Pediatric and adult lead poisoning. American Family Physician. — PubMed
- American College of Medical Toxicology (2010). Position statement on post-chelator challenge urinary metal testing. Journal of Medical Toxicology. — PubMed
- Bjorklund G, Mutter J, Aaseth J (2017). Metal chelators and neurotoxicity: lead, mercury, and arsenic. Archives of Toxicology. — PubMed
- Andersen O, Aaseth J (2016). A review of pitfalls and progress in chelation treatment of metal poisonings. Journal of Trace Elements in Medicine and Biology. — PubMed
- Mehrandish R, Rahimian A, Shahriary A (2019). Heavy metals detoxification: a review of herbal compounds for chelation therapy in heavy metals toxicity. Journal of Herbmed Pharmacology. — PubMed
- Kaplan M, Atakan IH, Aydoğdu N, Aktoz T, Özpuyan F, Seren G, et al. (2011). The effect of Coriandrum sativum in mercury chloride-induced renal toxicity in rats. Trakya University Tip Fakultesi Dergisi. — PubMed
- Sharma V, Kansal L, Sharma A (2010). Prophylactic efficacy of Coriandrum sativum (coriander) on testis of lead-exposed mice. Biological Trace Element Research. — PubMed
- Velaga MK, Yallapragada PR, Williams D, Rajanna S, Bettaiya R (2014). Hydroalcoholic seed extract of Coriandrum sativum (coriander) alleviates lead-induced oxidative stress in different regions of rat brain. Biological Trace Element Research. — PubMed
- Howard MR, Smyth A, Watson WA (2003). Clinical practice guidelines for evaluation and treatment of children with elevated blood lead levels — CDC framework reference. Pediatrics. — PubMed
- Klaassen CD (2018). Casarett and Doull's Toxicology: The Basic Science of Poisons (9th ed.) — reference text on heavy-metal toxicology and chelation. — PubMed
- Brown MJ, Willis T, Omalu B, Leiker R (2006). Deaths resulting from hypocalcemia after administration of edetate disodium: 2003-2005. Pediatrics — cautionary tale on wrong-EDTA-formulation chelation deaths. — PubMed
PubMed Topic Searches
- PubMed: Coriander heavy metal
- PubMed: Cilantro mercury
- PubMed: DMSA / DMPS / EDTA chelation
- PubMed: Provoked urine testing critique
- PubMed: Natural chelators review
Connections
- Coriander Seeds Overview
- Coriander Benefits Hub
- Coriander for Digestive Aid
- Coriander for Blood Sugar
- Coriander Antimicrobial
- Lead Toxicity
- Mercury Toxicity
- Arsenic
- Cadmium
- Aluminum
- Detoxification
- Chlorella
- Spirulina
- Glutathione
- Cysteine (NAC)