Boswellia for Respiratory Health & Asthma
Asthma is where Boswellia's mechanism is most tantalizing and its human evidence is thinnest. The cysteinyl leukotrienes that constrict the airways in asthma are made by the very enzyme Boswellia inhibits — the same pathway targeted by prescription drugs such as zileuton and montelukast. That parallel makes a natural 5-lipoxygenase inhibitor a reasonable thing to study for asthma. But the human evidence rests largely on a single small double-blind trial from 1998, which reported symptomatic improvement and has never been replicated at scale. This page lays out the rationale, the one real trial and its limits, and the single most important safety message: Boswellia is not a rescue inhaler and cannot replace prescribed asthma controllers. Asthma can be life-threatening, and controller medications save lives.
Table of Contents
- Leukotrienes and the Asthma Rationale
- The Prescription-Drug Parallel: Zileuton and Montelukast
- The Gupta 1998 Asthma Trial
- What the Trial Showed — and Its Limitations
- Beyond Asthma: Other Airway Conditions
- The Honest Verdict on the Respiratory Evidence
- Why Boswellia Cannot Replace Asthma Controllers
- Practical, Cautious Use
- Cautions
- Key Research Papers
- External Resources
- Connections
- Featured Videos
Leukotrienes and the Asthma Rationale
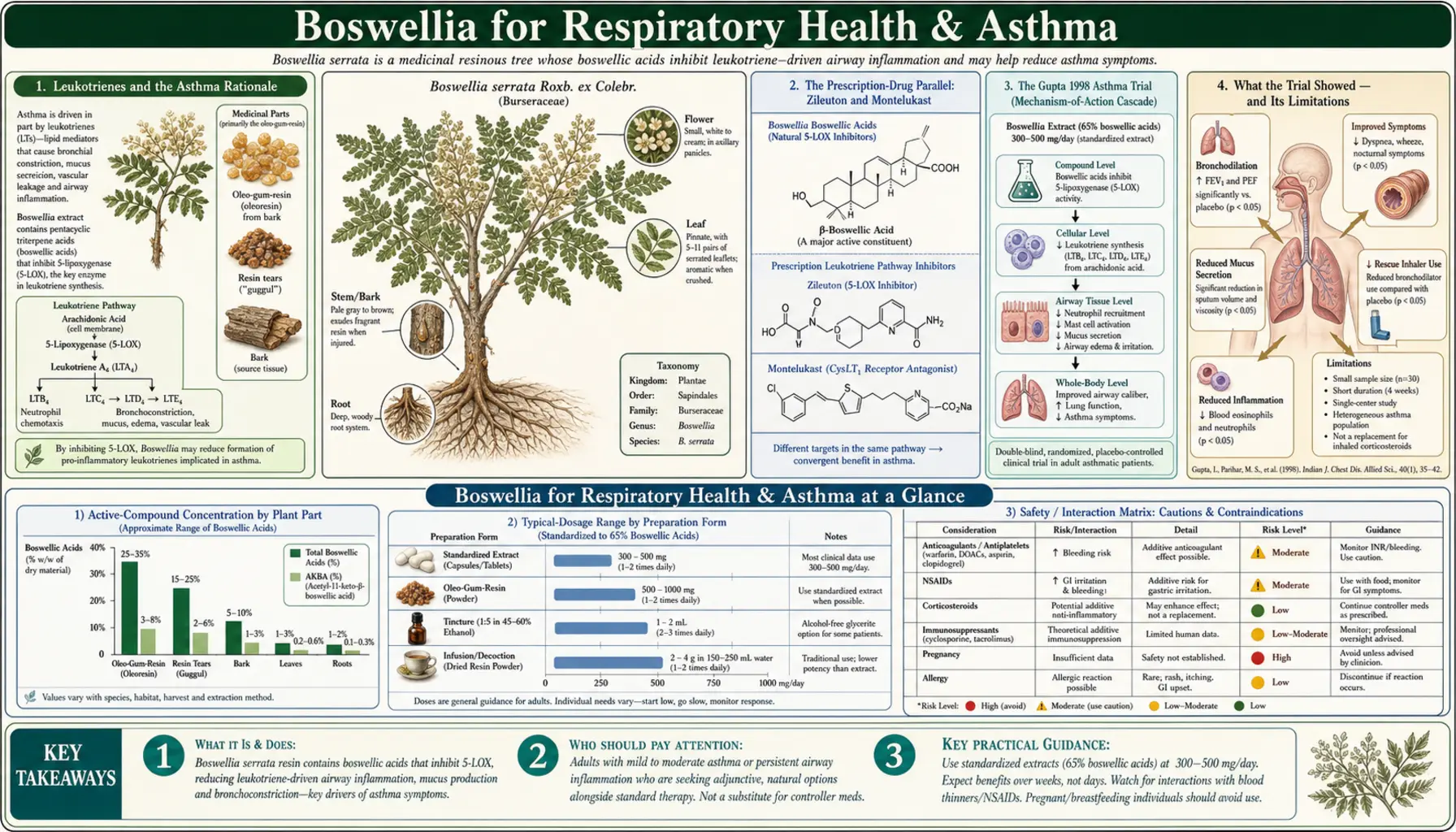
Asthma is fundamentally a disease of airway inflammation and hyperreactivity, and one family of inflammatory mediators sits close to its center: the cysteinyl leukotrienes (LTC4, LTD4, and LTE4). Historically known collectively as the “slow-reacting substance of anaphylaxis,” these molecules are among the most potent bronchoconstrictors the body produces. They tighten airway smooth muscle, increase mucus secretion, make blood vessels leaky (causing airway wall swelling), and help recruit eosinophils, the white blood cells characteristic of allergic asthma.
Crucially, cysteinyl leukotrienes are manufactured by the 5-lipoxygenase pathway — the same enzyme that Boswellia's boswellic acids inhibit, as detailed on the mechanism page. In principle, then, reducing 5-lipoxygenase activity should reduce cysteinyl leukotriene production and thereby ease bronchoconstriction and airway inflammation. This is a coherent, biologically grounded rationale — not folk speculation — which is exactly why researchers were willing to test the herb in asthma at all.
The Prescription-Drug Parallel: Zileuton and Montelukast
The strongest argument for taking Boswellia's asthma rationale seriously is that the pharmaceutical industry validated the exact same pathway with approved drugs. The class known as leukotriene modifiers includes:
- Zileuton — a direct 5-lipoxygenase inhibitor, which blocks leukotriene production at the same enzyme Boswellia targets. It is approved for asthma.
- Montelukast and zafirlukast — cysteinyl leukotriene receptor antagonists, which block the leukotrienes from acting on their receptors rather than stopping their synthesis. Montelukast in particular is widely used as an asthma controller and for allergic rhinitis.
The existence of these drugs proves that dampening the leukotriene pathway produces real clinical benefit in asthma. Boswellia sits at the same upstream position as zileuton — inhibiting synthesis rather than blocking receptors. It is important, though, not to over-read this parallel. A pharmaceutical 5-LOX inhibitor is a purified, dose-controlled molecule with proven pharmacokinetics; a botanical supplement with known absorption limitations is not automatically equivalent just because it acts on the same enzyme. The mechanism is shared; the evidence is not.
The Gupta 1998 Asthma Trial
The central piece of human evidence is a study by Gupta and colleagues published in the European Journal of Medical Research in 1998. It was a double-blind, placebo-controlled trial of Boswellia serrata gum resin in 40 patients with bronchial asthma. Patients took 300 mg three times daily (900 mg per day) for six weeks.
The reported results were positive: roughly 70% of the patients treated with Boswellia showed improvement — described as reduction or disappearance of symptoms such as shortness of breath and wheezing (rhonchi), a decrease in the number of asthma attacks, and improvements in objective measures including eosinophil count and the erythrocyte sedimentation rate (a general marker of inflammation). By comparison, only about 27% of the placebo group improved. The treatment was well tolerated over the six weeks.
On its own terms, this is an encouraging result with a plausible mechanism behind it. It is frequently cited as evidence that Boswellia “helps asthma.” The problem is not that the trial is bad — it is that a single small trial, however positive, is a starting point rather than a conclusion.
What the Trial Showed — and Its Limitations
Reading the 1998 trial responsibly means holding its encouraging result alongside its real limitations:
- Small and singular — 40 patients in one study. Modern asthma practice is built on large, multicenter trials, and no such large trial of Boswellia exists.
- Not replicated — more than two decades later, the finding has not been confirmed by rigorous, independent, adequately powered studies. In evidence-based medicine, unreplicated single trials are treated cautiously.
- Dated outcome measures — the trial predates the standardized spirometry and validated symptom-questionnaire endpoints used in contemporary asthma research, which makes its results harder to compare with modern data.
- Short duration — six weeks says nothing about long-term control, exacerbation prevention, or safety over the years a person actually lives with asthma.
None of this means the trial was wrong. It means the honest status of the evidence is “promising but unproven” — a preliminary signal awaiting the kind of confirmation that, so far, has not arrived.
Beyond Asthma: Other Airway Conditions
Boswellia is sometimes discussed for other respiratory conditions such as chronic bronchitis, chronic obstructive pulmonary disease (COPD), and allergic rhinitis, on the same anti-inflammatory logic. Here the evidence is even thinner than for asthma. Review articles on boswellic acids in chronic inflammatory disease list bronchial asthma among the conditions studied, but robust, large clinical trials in COPD or allergic rhinitis are lacking, and any benefit remains speculative.
It is fair to say that the leukotriene-and-inflammation rationale extends conceptually to these airway conditions, but it is not fair to present Boswellia as an evidence-based treatment for them. Where the trials do not exist, the honest answer is “we do not know,” not an optimistic extrapolation. Patients with COPD or chronic bronchitis should rely on established, guideline-based therapy and view Boswellia, at most, as an unproven adjunct to discuss with a clinician.
The Honest Verdict on the Respiratory Evidence
Pulling the respiratory evidence together:
- The mechanism is strong. Cysteinyl leukotrienes drive asthma, Boswellia inhibits their synthesizing enzyme, and approved drugs prove the pathway is a valid target.
- The human evidence is weak. One small 1998 trial reported benefit; it has not been replicated at scale, and there are no large modern randomized trials.
- The safety profile is reassuring but not a free pass. Boswellia is generally well tolerated, but tolerability is not the same as proven efficacy for a potentially dangerous disease.
The defensible conclusion is that Boswellia is an intriguing, mechanistically rational, but clinically unproven option for asthma — interesting enough to justify further research, not established enough to guide treatment. Compared with its osteoarthritis evidence, the respiratory case is far more preliminary.
Why Boswellia Cannot Replace Asthma Controllers
This is the most important section on the page. Asthma is a condition that can kill, and the difference between well-controlled and poorly controlled asthma is often the difference between a normal life and a fatal attack. Modern asthma treatment — inhaled corticosteroids, long-acting bronchodilators, and rescue inhalers — is one of the great success stories of chronic-disease management, backed by enormous bodies of evidence.
A supplement with a single small supporting trial cannot and must not take the place of these medications. Specifically:
- Never stop or reduce inhaled corticosteroids or other prescribed controllers to try Boswellia. Doing so can allow inflammation to rebuild silently and set the stage for a severe attack.
- Boswellia is not a rescue medication. It has no role during an acute asthma attack. A fast-acting bronchodilator (rescue inhaler) is what relieves acute bronchospasm; a slowly acting anti-inflammatory herb does nothing for an emergency.
- Any use should be additive and clinician-guided. If a person wishes to try Boswellia, it should be as an add-on to — never a substitute for — their prescribed regimen, and their asthma control should be monitored objectively.
Practical, Cautious Use
For a person with well-controlled asthma who, in partnership with their clinician, wants to try Boswellia as an adjunct, sensible guardrails apply:
- Keep every prescribed medication exactly as directed. Boswellia changes nothing about that.
- Use a studied, standardized extract with a stated boswellic-acid or AKBA content, taken with food to aid absorption.
- Monitor objectively. Peak-flow measurements, symptom diaries, and rescue-inhaler frequency reveal whether control is holding — do not rely on subjective impressions alone.
- Stop and seek care if control worsens. More frequent symptoms, more rescue-inhaler use, or nighttime waking are red flags that require medical attention, not more supplement.
- Discuss interactions with the prescriber, especially alongside leukotriene modifiers or other anti-inflammatory drugs.
Cautions
- Not a substitute for asthma medication — the single most important point on this page.
- Not for acute attacks — Boswellia has no rescue role; use a prescribed fast-acting inhaler and seek emergency care as advised.
- Evidence is preliminary — one small, dated, unreplicated trial is the core of the human data.
- Gastrointestinal side effects — nausea, reflux, and diarrhea can occur.
- Pregnancy and breastfeeding — insufficient safety data; avoid unless a clinician advises otherwise.
- Drug interactions — review with a clinician, particularly with other anti-inflammatory or immune-active medications.
Key Research Papers
- Gupta I, Gupta V, Parihar A, Gupta S, Lüdtke R, Safayhi H, Ammon HP (1998). Effects of Boswellia serrata gum resin in patients with bronchial asthma: results of a double-blind, placebo-controlled, 6-week clinical study. European Journal of Medical Research. — PubMed 9810030
- Safayhi H, Mack T, Sabieraj J, et al. (1992). Boswellic acids: novel, specific, nonredox inhibitors of 5-lipoxygenase. Journal of Pharmacology and Experimental Therapeutics. — PubMed 1602379
- Ammon HP (2006). Boswellic acids in chronic inflammatory diseases. Planta Medica. — PubMed 17024588
- Ammon HP (2016). Boswellic acids and their role in chronic inflammatory diseases. Advances in Experimental Medicine and Biology. — PubMed 27671822
- Ammon HP (2002). Boswellic acids (components of frankincense) as the active principle in the treatment of chronic inflammatory diseases. Wiener Medizinische Wochenschrift. — PubMed 12244881
- Abdel-Tawab M, Werz O, Schubert-Zsilavecz M (2011). Boswellia serrata: an overall assessment of in vitro, preclinical, pharmacokinetic and clinical data. Clinical Pharmacokinetics. — PubMed 21553931
PubMed Topic Searches
- PubMed: Boswellia serrata bronchial asthma
- PubMed: Cysteinyl leukotrienes in asthma
- PubMed: 5-lipoxygenase inhibitors (zileuton) in asthma
- PubMed: Leukotriene modifiers and airway inflammation
- PubMed: Boswellia in other airway conditions
External Resources
- LiverTox (NIH) — Boswellia serrata
- MedlinePlus — Boswellia (Indian Frankincense)
- NHLBI (NIH) — Asthma (guideline-based treatment overview)
- PubMed — Boswellia serrata asthma (all)
Connections
- Boswellia Overview
- Boswellia Benefits Hub
- Boswellia Anti-Inflammatory Mechanism
- Boswellia for Joint & Osteoarthritis
- Pulmonology
- Asthma
- COPD
- Bronchitis
- Quercetin
- Omega-3 Fatty Acids
- Ginger
- All Herbs