Ovarian Torsion
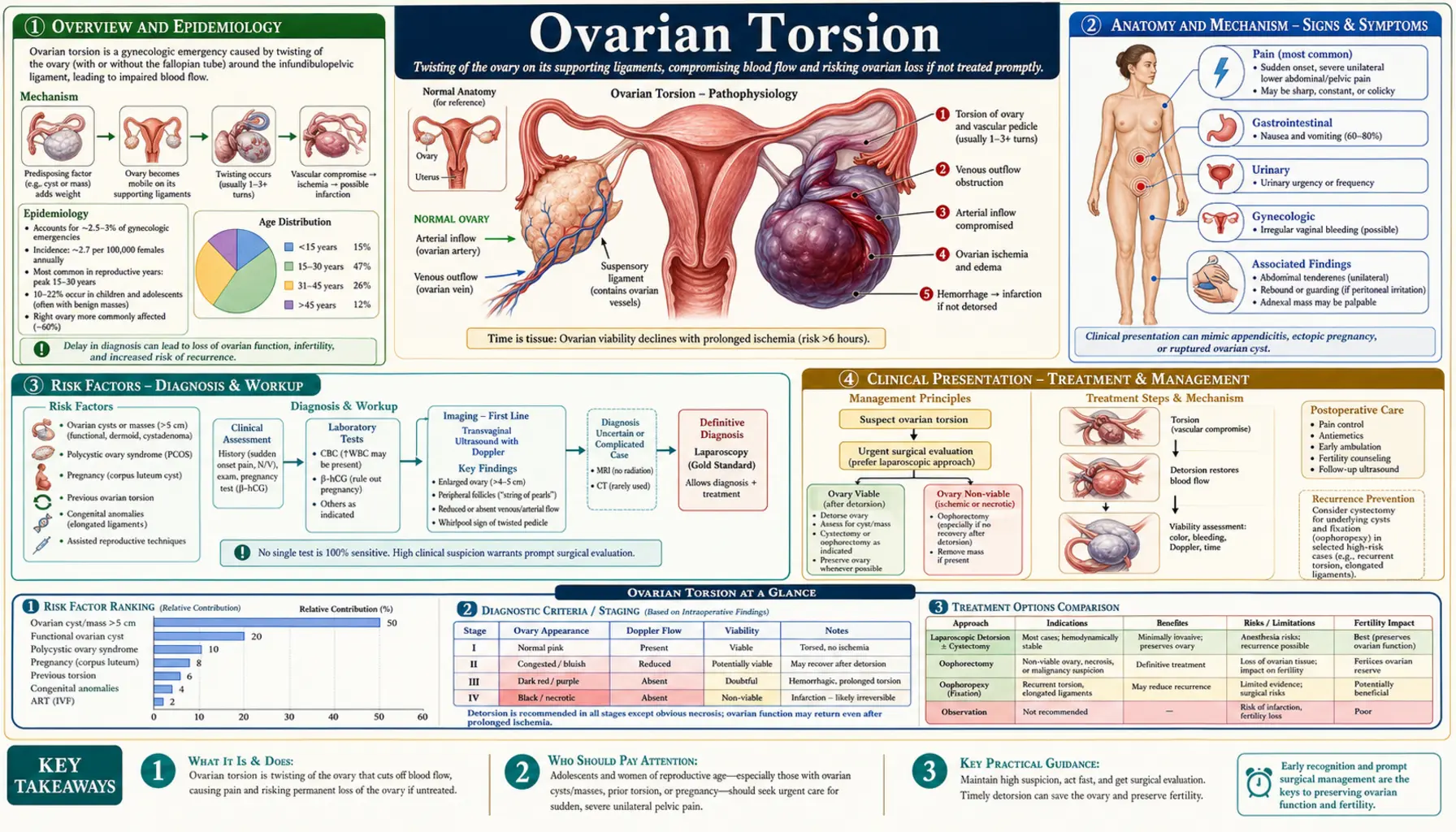
Table of Contents
- Overview and Epidemiology
- Anatomy and Mechanism
- Risk Factors
- Clinical Presentation
- Diagnosis and Imaging
- Surgical Treatment
- Fertility and Long-Term Outcomes
- Special Populations
- Recurrence and Prevention
- References and Research
- Connections
- Featured Videos
1. Overview and Epidemiology
Ovarian torsion is the partial or complete rotation of the ovary—and most often the fallopian tube—on its vascular pedicle. This twisting compresses the blood vessels that supply the ovary, cutting off first venous drainage, then arterial flow, ultimately leading to ischemia and, if untreated, irreversible infarction and permanent loss of the ovary.
Ovarian torsion accounts for roughly 2.7–7.4% of gynecological emergencies presenting to the emergency department. It is the fifth most common gynecological surgical emergency. Despite its relatively low overall incidence (approximately 5.9 per 100,000 women per year in population studies), the time-sensitive nature of the condition means that delayed recognition carries severe consequences: permanent ovarian damage or loss, affecting future fertility.
Torsion can occur at any age—from infancy through postmenopause—but peaks during the reproductive years. A second notable peak occurs in prepubertal and adolescent girls, in whom torsion of a morphologically normal ovary (without a mass) is proportionally more common than in adults. Prompt recognition and surgical management within hours of symptom onset is the decisive factor in ovarian salvage.
2. Anatomy and Mechanism
The ovary is suspended in the pelvis by three ligamentous structures: the infundibulopelvic (IP) ligament (which carries the ovarian artery and vein superiorly toward the aorta and inferior vena cava), the utero-ovarian ligament (medially to the uterine cornu), and the mesovarium (the peritoneal fold connecting ovary to broad ligament). The fallopian tube shares the utero-ovarian pedicle and therefore rotates with the ovary in most torsion events—producing the commonly described adnexal torsion.
Torsion progresses in stages:
- Venous obstruction: the lower-pressure venous system is compressed first, causing ovarian engorgement and edema—the ovary enlarges, often appearing as a large, echogenic mass on ultrasound even when the underlying pathology was a small cyst.
- Arterial compromise: as twisting tightens, arterial inflow decreases. Intermittent torsion (wrapping and spontaneously unwrapping) may cause episodic pain with temporary resolution.
- Infarction: sustained arterial occlusion leads to ischemic necrosis. The ovary turns hemorrhagic and dark blue-black at laparoscopy.
A critical anatomical asymmetry explains why the right ovary torts more frequently than the left (roughly 60% of cases). The sigmoid colon occupies the left pelvic space and physically limits leftward adnexal mobility, while the right side is adjacent to the more mobile cecum and has a longer utero-ovarian ligament on average.
3. Risk Factors
Any condition that increases ovarian mass or alters adnexal mobility raises torsion risk. The single most important risk factor is an ovarian or adnexal mass larger than 5 cm, which acts as a fulcrum around which the ovary spins.
Ovarian Masses
- Benign cystic teratoma (dermoid cyst): the most commonly associated benign tumor. Dermoids are often bilateral, which also explains bilateral torsion risk. Their dense sebaceous content gives them a characteristic ultrasound appearance (hyperechoic nodule with posterior shadowing, “tip of the iceberg” sign).
- Functional cysts: follicular and corpus luteum cysts can enlarge enough (typically >5 cm) to enable rotation. They are the most common cause in reproductive-age women because of their frequency.
- Paratubal cysts: remnants of the Wolffian duct adjacent to the tube; especially important in adolescents, where they may cause torsion without any ovarian enlargement.
- Benign serous or mucinous cystadenoma and other ovarian neoplasms.
- Malignant tumors can cause torsion, though less commonly than benign masses (malignant tumors are often fixed by adhesions to pelvic structures, paradoxically reducing mobility).
Ovulation Induction and Assisted Reproduction
Women undergoing controlled ovarian hyperstimulation for IUI or IVF develop multiple enlarged follicles, dramatically increasing the size and weight of both ovaries. The risk of torsion during and immediately after stimulation is substantially elevated compared with the general population. Ovarian hyperstimulation syndrome (OHSS) compounds the risk by causing further ovarian enlargement and ascites.
Pregnancy
The first trimester of pregnancy is a vulnerable period: the corpus luteum cyst of pregnancy can reach 6–8 cm, and the enlarging uterus displaces adnexal structures, increasing rotational leverage. Torsion complicates approximately 1 in 5,000 pregnancies.
Prior Torsion
Women with a history of unilateral torsion have a significantly elevated risk of contralateral torsion, particularly if the underlying predisposing condition (e.g., elongated infundibulopelvic ligament, dermoid) was not corrected. Recurrence risk on the same side after detorsion without oophoropexy is estimated at 10–15%.
Normal-Ovary Torsion
In prepubertal girls and adolescents, torsion frequently occurs without any identifiable ovarian pathology. An abnormally long utero-ovarian ligament is thought to be the anatomical predisposing factor, allowing the ovary to swing freely and rotate on its pedicle. This population is frequently misdiagnosed because clinicians may not consider torsion without an ovarian cyst on imaging.
4. Clinical Presentation
The hallmark symptom of ovarian torsion is sudden onset, severe, unilateral lower abdominal or pelvic pain, present in approximately 96% of confirmed cases. The pain is typically localized to one side and may radiate to the flank, groin, or inner thigh. Its abrupt onset reflects the acute vascular compromise that triggers peritoneal irritation and visceral pain.
Associated Symptoms
- Nausea and vomiting: present in up to 70% of cases—a useful distinguishing feature from many other causes of pelvic pain, though not specific to torsion.
- Low-grade fever: may develop as ischemia progresses toward infarction, releasing inflammatory mediators. Fever is a concerning sign suggesting possible necrosis or impending peritonitis.
- Palpable adnexal mass: a tender pelvic mass is detectable on exam in approximately 50% of cases; it may represent the enlarged torted ovary or the underlying cyst.
- Leukocytosis: mild elevation in white blood cell count is common but non-specific.
- Peritoneal signs: rebound tenderness and guarding suggest significant intraperitoneal irritation and may indicate advanced ischemia or rupture of an associated cyst.
Intermittent and Atypical Presentations
Partial torsion, where the adnexa wraps partially and then spontaneously unwinds, causes episodic or intermittent pain that may partially or fully resolve between episodes. Patients with intermittent torsion may present multiple times to the emergency department with “recurrent pelvic pain” before a definitive diagnosis is made. This pattern is particularly deceptive and can lead to significant diagnostic delay. The pain-free intervals occur when venous flow is transiently restored after spontaneous detorsion—but each episode causes incremental ischemic damage.
In children, the presentation can be especially misleading: nonspecific abdominal pain, periumbilical or diffuse rather than lateralized, with vomiting dominating the picture. Torsion should be high on the differential for any girl presenting with acute abdominal pain and vomiting.
5. Diagnosis and Imaging
Ovarian torsion is primarily a clinical diagnosis confirmed at surgery. No single laboratory test or imaging modality reliably rules it out, and a high index of suspicion must be maintained even when initial studies appear reassuring.
Pelvic Ultrasound with Doppler
Transvaginal (or transabdominal in children) pelvic ultrasound with Doppler flow assessment is the first-line imaging study. Findings that raise concern for torsion include:
- An enlarged, edematous ovary (often appearing as a round, uniformly echogenic mass due to diffuse stromal edema)
- A unilateral adnexal mass, commonly a dermoid or follicular cyst
- Peripheral displacement of ovarian follicles to the cortex around an edematous stroma (the “string of pearls” sign)
- Free pelvic fluid (may represent a ruptured cyst, hemorrhage from the torted ovary, or reactive fluid)
- The “whirlpool sign”: the twisted vascular pedicle seen on Doppler as a coiled, spiral-appearing vessel cluster—when identified, this finding is highly specific for torsion
The Critical Limitation of Doppler
This is the most clinically important point: the presence of normal ovarian blood flow on Doppler does NOT exclude torsion. This cannot be overemphasized. In partial torsion, the arterial supply may remain patent while venous outflow is already compromised. Studies report that Doppler is falsely reassuring in 40–60% of surgically confirmed torsion cases. A normal Doppler study should never be used to discharge a patient with a clinical picture consistent with torsion without further evaluation or surgical consultation.
CT and MRI
Computed tomography (CT) of the abdomen and pelvis is often obtained in the emergency department when the diagnosis is uncertain and appendicitis or other surgical pathologies are on the differential. CT can identify an adnexal mass, ovarian enlargement, and free fluid but lacks the sensitivity of MRI for soft-tissue characterization. MRI provides excellent visualization of the twisted vascular pedicle, the extent of ovarian ischemia, and the composition of any mass, but its use is limited by availability and time in the acute setting.
Diagnosis at Laparoscopy
When clinical suspicion is high despite inconclusive imaging, diagnostic and therapeutic laparoscopy is the appropriate next step. The definitive diagnosis is made intraoperatively when the twisted adnexa is directly visualized. Delay for additional workup is inappropriate when the clinical picture is compelling—the surgeon should proceed to the operating room promptly.
6. Surgical Treatment
Ovarian torsion is a surgical emergency. The primary goal is to restore blood flow to the ovary as quickly as possible. The overriding principle is that a dark, necrotic-appearing ovary does not necessarily mean irreversible damage—remarkable viability has been demonstrated even in grossly ischemic tissue after prompt detorsion.
Laparoscopic Detorsion
Laparoscopic untwisting (detorsion) of the adnexa is the treatment of choice and should be performed regardless of the ovary’s macroscopic appearance at surgery. Historically, surgeons would perform immediate salpingo-oophorectomy for a visually necrotic ovary out of concern for thromboembolic events from “releasing” the torted pedicle. This practice is no longer supported by evidence:
- Multiple series report that ovaries appearing black or dark blue at detorsion demonstrate normal or near-normal function (ovulation, follicular development) on follow-up ultrasound in 88–100% of cases when blood flow returns within 48 hours of onset.
- The feared thromboembolic complication from detorsion of a necrotic ovary has not been borne out in large case series.
- Ovarian tissue recovery is supported by the ovary’s capacity for collateral circulation and the dense revascularization potential of ovarian stroma.
Concurrent Cystectomy
If an ovarian cyst or mass is identified as the precipitating factor, laparoscopic cystectomy can be performed concurrently at the same operative setting or planned for a second stage once viability is confirmed. Dermoids and simple cysts are safely removed laparoscopically. Complex or suspicious masses may warrant further preoperative evaluation before cystectomy.
When Salpingo-Oophorectomy Is Indicated
Removal of the ovary and tube is reserved for situations where frank gangrene is unequivocal (tissue is friable, frankly necrotic, or fails to demonstrate any perfusion after a brief period of observation post-detorsion), the patient is postmenopausal (ovarian preservation is less critical), or tissue characteristics suggest malignancy requiring complete excision and staging.
Surgical Access: Laparoscopy vs. Laparotomy
Laparoscopy is the standard approach and carries lower morbidity, shorter recovery, and equivalent efficacy compared with open surgery. Laparotomy may be necessary in cases with extensive pelvic adhesions, hemodynamic instability, or inability to safely perform laparoscopy due to body habitus or prior surgeries.
7. Fertility and Long-Term Outcomes
Early surgical intervention is strongly associated with excellent fertility outcomes. Women who undergo prompt laparoscopic detorsion generally retain normal ovarian function and achieve future pregnancies at rates comparable to women who have not experienced torsion.
Ovarian Function After Detorsion
The majority of studies following women after laparoscopic detorsion demonstrate:
- Return of ovarian blood flow on Doppler within days to weeks in over 90% of cases
- Evidence of follicular activity (antral follicles, ovulation) on follow-up ultrasound in 88–100% of salvaged ovaries at 6–12 months
- Anti-Müllerian hormone (AMH) levels in the normal range in the majority of women followed long-term, suggesting preserved primordial follicle pool
Impact of Salpingo-Oophorectomy
Women who undergo salpingo-oophorectomy for torsion with a necrotic ovary lose the functional reserve of that ovary. In women with a normal contralateral ovary, this typically does not impair natural fertility, as the remaining ovary compensates. However, in women with diminished contralateral reserve or those who later develop contralateral torsion, the loss is clinically significant. This reinforces the case for attempting detorsion and ovarian conservation in all patients.
Timing and Outcomes
Duration of ischemia strongly predicts outcomes:
- Torsion duration under 24 hours: nearly universal ovarian salvage when detorsion is performed promptly
- 24–48 hours: majority of ovaries still viable after detorsion, though rates decline
- Greater than 48 hours: risk of irreversible necrosis increases substantially, though successful salvage is still reported
The practical implication: there is no “safe window” to delay surgery while awaiting more diagnostic certainty. If torsion is suspected, the patient should go to the operating room.
8. Special Populations
Pediatric and Adolescent Patients
Ovarian torsion in girls under 15 presents unique diagnostic challenges. The pain is often non-specific and may be diffuse or periumbilical rather than lateralized. Vomiting frequently dominates the clinical picture, leading to workups for gastrointestinal pathology (gastroenteritis, appendicitis) and delaying the correct diagnosis.
A critical point in pediatric torsion is the high prevalence of torsion occurring in morphologically normal ovaries (without a mass). Ultrasound may show an enlarged, edematous ovary without an obvious cyst or tumor. Because clinicians often associate torsion with an ovarian mass, normal-appearing ovaries on imaging are frequently dismissed, and the diagnosis is delayed. In pediatric patients with classic symptoms, the absence of an ovarian cyst should not be used to exclude torsion.
Ovarian preservation is especially important in children and adolescents, given the decades of reproductive function that remain. Aggressive surgical conservatism (detorsion even of grossly ischemic ovaries) is strongly advocated in this age group.
Pregnancy
Ovarian torsion during pregnancy is challenging to manage because concern for fetal exposure to anesthesia and surgical stress adds complexity. However, the risk of leaving torsion untreated (maternal ischemic injury, peritonitis, preterm labor from intraperitoneal inflammation) outweighs the procedural risk. Laparoscopic detorsion is safe throughout pregnancy, with the lowest risk in the second trimester. Obstetricians and gynecologic surgeons should collaborate on management. The corpus luteum (a frequent precipitant in the first trimester) can typically be preserved during cystectomy using careful hemostasis.
Postmenopausal Women
Torsion is less common after menopause because ovarian mass lesions are less frequent and the pelvic floor is less mobile. When it occurs, the differential diagnosis must include ovarian malignancy (which rises sharply in prevalence after menopause). Any adnexal torsion in a postmenopausal woman warrants complete surgical staging evaluation if the removed tissue is suspicious for malignancy on frozen section.
9. Recurrence and Prevention
The risk of recurrent ipsilateral torsion after detorsion alone (without fixation) is approximately 10–15%, though estimates vary widely across studies. Contralateral torsion is also elevated in women with prior torsion, particularly when the predisposing anatomical factor (elongated ligament, dermoid) is bilateral or when the contralateral ovary is enlarged.
Oophoropexy
Oophoropexy—surgical fixation of the ovary to the pelvic sidewall, utero-ovarian ligament, or posterior broad ligament—is performed to prevent recurrence. Indications and technique are debated:
- Strongest indication: prepubertal and adolescent girls, in whom torsion frequently involves a normal ovary (high recurrence risk without fixation) and in whom the long reproductive lifespan makes ovarian preservation critical.
- In adults: oophoropexy is generally recommended when the contralateral ovary has already been lost to torsion, or when no correctable precipitating cause (e.g., cyst) has been addressed. Some surgeons perform routine bilateral oophoropexy after detorsion in all patients; evidence is insufficient to mandate this approach universally.
- Technique: shortening the utero-ovarian ligament with non-absorbable suture (plicating), or suturing the ovary to the peritoneum of the posterior broad ligament or pelvic sidewall. Care must be taken not to compress ovarian vasculature.
Cyst Management
Addressing the underlying precipitating mass—whether dermoid, follicular cyst, or other benign tumor—reduces recurrence risk. Concurrent cystectomy during detorsion is preferred when technically feasible and safe. For dermoids, the contralateral ovary should also be evaluated at the time of surgery, given the 10–15% bilateral incidence of dermoid cysts.
10. References and Research
Key Research Papers
- Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Annals of Emergency Medicine. 2001;38(2):156–159. PMID: 11468611
- Shalev E, Bustan M, Yarom I, Peleg D. Recovery of ovarian function after laparoscopic detorsion. Human Reproduction. 1995;10(11):2965–2966 — Search PubMed
- Oelsner G, Cohen SB, Soriano D, et al. Minimal surgery for the twisted ischaemic adnexa can preserve ovarian function. Human Reproduction. 2003;18(12):2599–2602 — Search PubMed
- Cohen SB, Wattiez A, Seidman DS, et al. Laparoscopy versus laparotomy for detorsion and sparing of twisted ischemic adnexa. JSLS. 2003;7(4):295–299 — Search PubMed
- Nizar K, Deutsch M, Filmer S, et al. Doppler studies of the ovarian venous blood flow in the diagnosis of adnexal torsion. Journal of Clinical Ultrasound. 2009;37(8):436–439 — Search PubMed
- Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics. 2008;28(5):1355–1368. PMID: 18794312
- Guthrie BD, Adler MD, Powell EC. Incidence and trends of pediatric ovarian torsion hospitalizations in the United States, 2000–2006. Pediatrics. 2010;125(3):532–538 — Search PubMed
- Huchon C, Fauconnier A. Adnexal torsion: a literature review. European Journal of Obstetrics and Gynecology and Reproductive Biology. 2010;150(1):8–12 — Search PubMed
- Schmeler KM, Mayo-Smith WW, Peipert JF, et al. Adnexal masses in pregnancy: surgery compared with observation. Obstetrics and Gynecology. 2005;105(5):1098–1103. PMID: 15863550
- Spinelli C, Buti I, Pucci V, et al. Adnexal torsion in children and adolescents: new trends to conservative surgical approach — our experience and review of literature. Gynecological Endocrinology. 2013;29(1):54–58 — Search PubMed
- Mashiach R, Melamed N, Gilad N, et al. Sonographic diagnosis of ovarian torsion: accuracy and predictive factors. Journal of Ultrasound in Medicine. 2011;30(9):1205–1210 — Search PubMed
- Hibbard LT. Adnexal torsion. American Journal of Obstetrics and Gynecology. 1985;152(4):456–461 — Search PubMed
PubMed Topic Searches
- PubMed — ovarian torsion laparoscopy
- PubMed — adnexal torsion detorsion
- PubMed — ovarian torsion Doppler ultrasound
- PubMed — ovarian torsion pediatric
- PubMed — oophoropexy torsion prevention
- PubMed — ovarian torsion fertility outcomes
- PubMed — adnexal torsion pregnancy
- PubMed — ovarian torsion dermoid cyst
11. Connections
- Ovarian Cysts
- Female Infertility
- Endometriosis
- Ectopic Pregnancy
- Premature Ovarian Insufficiency
- Uterine Fibroids
- Infertility (General)
- Polycystic Ovary Syndrome (PCOS)
- PMS and PMDD
- Perimenopause
- Reproductive Medicine
- Lab Tests