Menopause and HRT: History and Discovery
Menopause is a natural life stage, not a disease — every woman who lives long enough reaches it, and the end of menstruation is a normal biological transition rather than an illness to be cured. Yet the medical history of menopause is genuinely important, because for two centuries it shaped how women were diagnosed, treated, dismissed, and sometimes harmed. The word “menopause” was coined by the French physician Charles-Pierre-Louis de Gardanne around 1812 and formalized in his 1821 book. Estrogen, the hormone at the centre of the story, was identified by Edgar Allen and Edward Doisy in 1923; conjugated estrogens (Premarin) reached the market in 1942; and decades of enthusiastic, drug-company-backed promotion of hormone “replacement” were upended by the 2002 Women’s Health Initiative results, followed by years of more careful, individualized re-evaluation. This page tells that history accurately and respectfully — honouring the women involved, naming the sexism that ran through much of it, and never inventing a discoverer, a date, or a “first.”
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →Table of Contents
- A Natural Life Stage, Not a Disease
- Naming the Change: Gardanne and the Word “Menopause”
- Medicalization and Historical Stigma
- The Discovery of Estrogen (1923–1935)
- Premarin and the Birth of Hormone Therapy (1942)
- “Feminine Forever” and the Marketing of Replacement (1966)
- The Women’s Health Initiative (2002): The Turning Point
- Aftermath and the Modern, Individualized View
- Research Papers and References
- Connections
- Featured Videos
A Natural Life Stage, Not a Disease
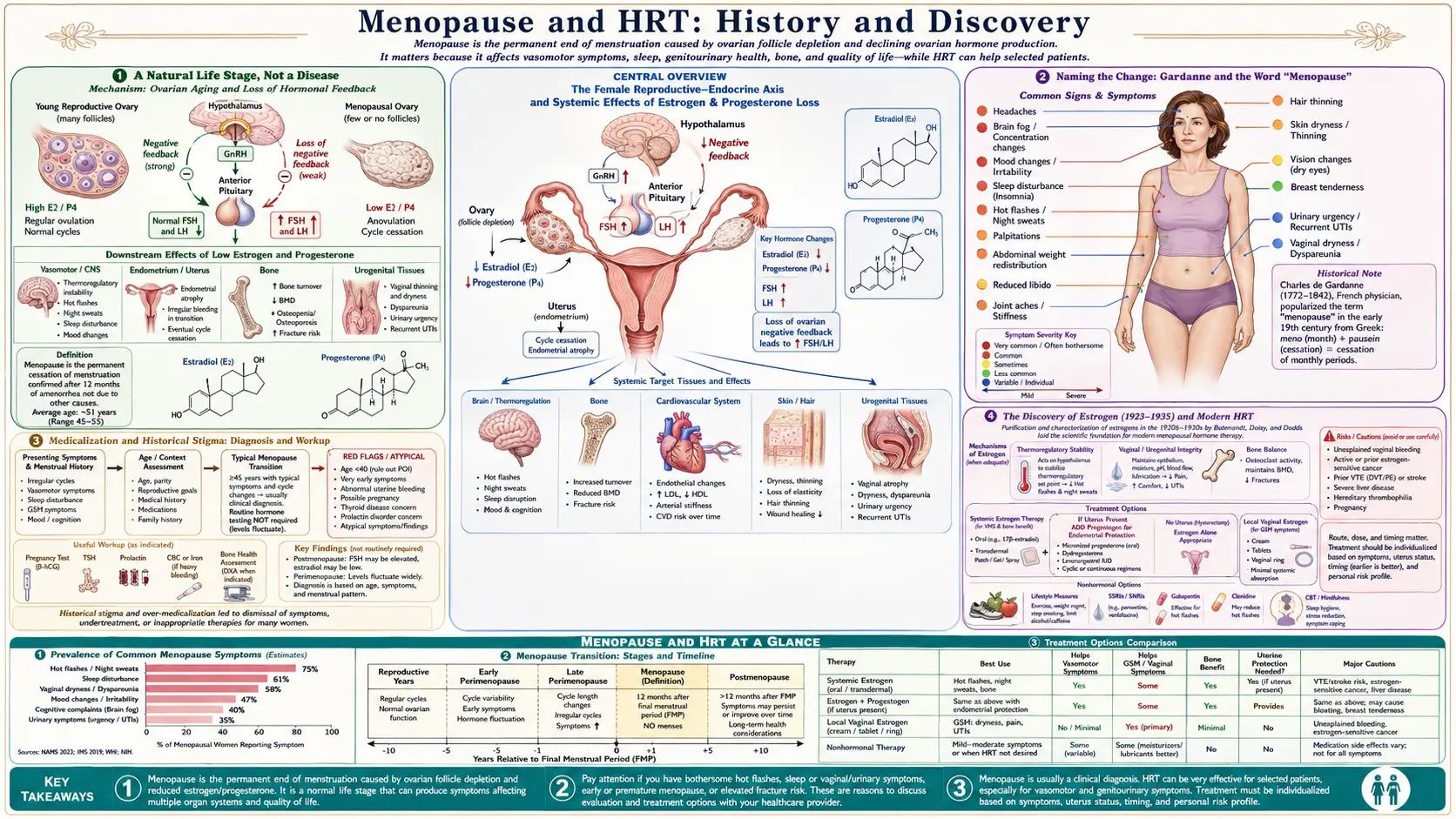
Menopause is defined, by convention, as the point twelve months after a woman’s final menstrual period — the permanent end of ovulation and monthly bleeding. In most women it occurs naturally between roughly ages 45 and 55, with an average around 51, and it is preceded by the years-long hormonal transition called perimenopause. It is a universal, expected event in the human female life course, not a pathology: it is what happens, in the ordinary run of biology, when the ovaries gradually retire from their reproductive role. Framing it first as a normal life stage is not a small point. Much of the harm in this history flowed directly from the opposite framing — the idea that a healthy midlife woman was, by virtue of her hormones, sick.
That said, the transition can bring real and sometimes disruptive symptoms — hot flashes and night sweats (vasomotor symptoms), disturbed sleep, mood changes, and vaginal and urinary changes — and the long-term drop in estrogen carries genuine health consequences, most notably accelerated bone loss and a shift in cardiovascular risk. Acknowledging both truths at once is the honest position: menopause is normal and does not need “curing,” and its symptoms and downstream effects are legitimate, treatable medical concerns that women deserve to have taken seriously. The history below is the long, uneven story of medicine trying — and frequently failing — to hold those two ideas together.
Because real people read pages like this one, a note up front: nothing here is medical advice, and the science of hormone therapy has changed substantially over time. Decisions about treating menopausal symptoms are individual, and depend on a woman’s age, time since menopause, symptoms, and personal risk profile — a conversation for a woman and her own clinician, informed by the current evidence summarized at the end of this article.
Naming the Change: Gardanne and the Word “Menopause”
People experienced menopause for as long as there have been people, and pre-modern writers — from Aristotle and the Hippocratic authors onward — noted that menstruation ceased in older women and offered an assortment of names and explanations for it. But the specific medical term we use today has a documented origin. The French physician Charles-Pierre-Louis de Gardanne coined the word ménopause, drawing on the Greek roots mēn (month) and pausis (a cessation or pause) — literally, “the stopping of the months.” Most sources date his first use of the term to about 1812; he then formalized and popularized it in his 1821 book, De la ménopause, ou de l’âge critique des femmes (“On Menopause, or the Critical Age of Women”). Historians of medicine note that his earliest writing used older variant spellings (rendered as ménépausie or ménespausie) before he settled on the cleaner form ménopause; the variant spellings are reported by secondary historical sources and the precise early orthography is treated here as historians describe it rather than asserted as a single fixed fact.
Gardanne’s stated motive, recorded in his own preface, was practical and even sympathetic: physicians and writers had been using a confusing tangle of phrases — “the critical age,” “the change of life,” and far less kind expressions — and he wanted a single, neutral, technical term to reduce confusion between doctors and their patients. Coining a precise word was, in that sense, a step toward taking the experience seriously. It is worth being clear about what Gardanne did and did not do: he named the life stage; he did not “discover” it, and he certainly did not discover the hormones behind it, which would not be identified for another century. Conflating the coinage of the word with the later biochemical discovery of estrogen is a common error, and the two are kept carefully distinct on this page.
The English word “menopause” entered medical usage over the following decades as Gardanne’s term was translated and adopted. From the beginning, then, the modern vocabulary of menopause was a French medical invention of the early nineteenth century — a fact that also helps explain why so much of the era’s framing of menopause as a “critical” or dangerous age came packaged with the name itself.
Medicalization and Historical Stigma
For much of the nineteenth and twentieth centuries, menopause was steadily medicalized — reframed from an ordinary life passage into a perilous “critical age” freighted with disease and decline. The very subtitle of Gardanne’s 1821 book, l’âge critique (“the critical age”), set the tone. Nineteenth-century medical texts routinely linked the end of menstruation to a long catalogue of supposed afflictions — nervousness, melancholy, “hysteria,” insanity, and assorted physical complaints — and some physicians treated midlife women with the harsh interventions of the day. This page names that history plainly because it was real and it did harm; it does not endorse or repeat those framings.
Running through this medical literature was a current of frank sexism. A healthy woman past her childbearing years was frequently portrayed in the sources of the time as diminished, depleted, or even useless — her value implicitly tied to fertility and youth. The expression “women’s inferno,” cited by Gardanne among the existing names for the change, captures the tenor. These attitudes were not incidental: they directly shaped how women were diagnosed and treated, encouraged the dismissal of genuine symptoms as mere “female complaints,” and, in the twentieth century, helped create a receptive market for the idea that menopause was a deficiency disease in urgent need of correction. Acknowledging this sexism is essential to telling the history honestly — and to understanding why later, drug-company-driven messaging about staying “feminine forever” found such ready purchase.
The corrective, hard-won over the past several decades, has been a return to the starting point of this article: menopause is a normal stage of life. Modern medicine increasingly distinguishes between respecting menopause as natural and treating the specific symptoms that trouble a given woman — without pathologizing the whole of midlife womanhood. That distinction is the quiet but profound shift that separates the contemporary view from the older, stigmatizing one.
The Discovery of Estrogen (1923–1935)
The biological understanding of menopause — that it is driven by the decline of ovarian hormones — rests on the discovery of estrogen, which is a twentieth-century scientific story quite separate from Gardanne’s naming of the life stage. In 1923, the American scientists Edgar Allen, an anatomist, and Edward Adelbert Doisy, a biochemist, working at Washington University in St. Louis, demonstrated that the ovarian follicle produces a hormone that controls the female reproductive cycle. They extracted this active substance from the ovaries and proved its biological effect with a bioassay in rodents that became known as the Allen–Doisy test. This 1923 work is rightly remembered as the identification of estrogen as the ovarian hormone.
Isolating the pure hormone took several more years. In 1929, Doisy in the United States and the German chemist Adolf Butenandt in Germany — working independently and at nearly the same time — succeeded in crystallizing the first estrogen, the compound now called estrone (Doisy initially named his preparation “theelin”). Doisy’s laboratory went on to isolate the related estrogens estriol (around 1930) and estradiol (the most potent natural estrogen, around 1935). It is a notable historical footnote that, although Doisy’s estrogen work was Nobel-calibre, the Nobel Prize he eventually shared in 1943 (with Henrik Dam) was awarded for an entirely different discovery — the chemistry of vitamin K, not for estrogen. Butenandt, for his part, received the 1939 Nobel Prize in Chemistry for his broader work on sex hormones.
The importance of these discoveries for menopause is direct. Once science had a purified hormone that the aging ovary stops making, it became possible to conceive of giving that hormone back — the literal idea of “hormone replacement.” The discovery of estrogen thus set the stage for everything that followed, for good and for ill: it underpinned the legitimate treatment of severe menopausal symptoms, and it equally underpinned the overreaching claim that menopause itself was simply an estrogen deficiency to be topped up indefinitely.
Premarin and the Birth of Hormone Therapy (1942)
Turning isolated estrogen into a practical medicine required a manufacturable source. In the late 1930s the pharmaceutical firm Ayerst, McKenna & Harrison (a Canadian company that, through later mergers, became part of Wyeth) developed a way to extract a mixture of estrogens from the urine of pregnant mares — a rich and renewable natural source. The product was named Premarin, a contraction of “PREgnant MARes’ urINe.” Conjugated estrogens under the Premarin brand were introduced in Canada in 1941 and approved in the United States in 1942, where the U.S. Food and Drug Administration permitted marketing for menopausal symptoms; the United Kingdom followed in 1956.
Premarin made estrogen therapy widely available for the first time, and for the genuinely severe symptoms of menopause — intense hot flashes, debilitating night sweats, distressing vaginal atrophy — it could be strikingly effective. Over the following decades it became one of the most prescribed drugs in the United States. (Worth noting alongside the medical history: the use of pregnant mares to collect urine for Premarin drew sustained criticism on animal-welfare grounds, a controversy that has accompanied the drug throughout its commercial life.)
For roughly the first thirty years, estrogen was typically given alone (“unopposed”). In the 1970s, researchers documented that unopposed estrogen markedly increased the risk of endometrial (uterine) cancer in women who still had a uterus. The response was to add a progestogen (a progesterone-like hormone) to protect the uterine lining — the origin of the distinction, still central today, between combined estrogen-plus-progestogen therapy for women with a uterus and estrogen-alone therapy for women who have had a hysterectomy. This 1970s endometrial-cancer scare was the first major signal that “more hormones for everyone” carried real risks — a warning that the marketing of the era had largely drowned out, and that the 2002 trial would amplify decisively.
“Feminine Forever” and the Marketing of Replacement (1966)
No single document did more to popularize lifelong hormone therapy — or better illustrates the era’s entanglement of medicine, sexism, and commerce — than the 1966 bestseller Feminine Forever, by the New York gynecologist Robert A. Wilson (published by M. Evans and Company). Wilson advanced the sweeping claim that menopause was an estrogen-deficiency disease, and that with estrogen women could remain youthful, attractive, and “feminine” indefinitely, avoiding what he portrayed as the decay of menopause. The book was enormously influential, sold widely, and helped drive a steep rise in estrogen prescriptions; within about a decade of its publication, Premarin had become one of the top-selling prescription drugs in the United States.
The book’s framing was both scientifically overreaching and openly sexist — it defined a woman’s worth in terms of preserved youth and femininity, and it recast a normal life stage as a dreaded disease. Crucially, what its millions of readers were not told at the time is that the project was financially compromised. It was later documented — and Wilson’s own son acknowledged in press accounts decades afterward — that the pharmaceutical manufacturer of Premarin (Wyeth-Ayerst) had funded Wilson’s book, his speaking tours, and his research foundation. In other words, a landmark of pro-estrogen patient persuasion was, in substantial part, undisclosed pharmaceutical marketing. This is presented here as the documented historical record it is: an early and consequential example of industry influence over medical messaging directed at women, and a cautionary tale that the later reassessment would vindicate.
Through the 1970s, 1980s, and 1990s, hormone “replacement” therapy (HRT) was widely prescribed not only to relieve symptoms but in the belief — based largely on observational studies — that it broadly protected women’s long-term health, including their hearts and bones. By the 1990s, millions of women were taking long-term HRT, often for years, partly in the expectation of preventing heart disease. That expectation rested on a weaker evidentiary foundation than its popularity implied, and it was precisely this question — does HRT prevent chronic disease in healthy women? — that a large randomized trial was finally designed to answer.
The Women’s Health Initiative (2002): The Turning Point
The decisive moment in this history came in 2002, with the first major results of the Women’s Health Initiative (WHI) — a large, NIH-funded set of randomized controlled trials, the gold standard of medical evidence, designed specifically to test whether long-term hormone therapy prevented chronic disease in generally healthy postmenopausal women. One arm enrolled women with a uterus and randomly assigned them to either combined conjugated equine estrogens plus the progestin medroxyprogesterone acetate (the common Prempro formulation) or to placebo. On July 8–9, 2002, this combined-therapy arm was stopped early, after an average of about 5.2 years, because the monitoring board judged that the harms outweighed the benefits; the principal results were published in JAMA on July 17, 2002.
The findings overturned decades of assumption. In this trial of combined estrogen-plus-progestin, the therapy was associated with an increased risk of invasive breast cancer (roughly a 26% relative increase), an increased risk of stroke, an increased risk of blood clots (pulmonary embolism and deep-vein thrombosis), and an increased risk of coronary heart disease events — the very opposite of the cardiac protection many had expected. There were genuine benefits, too, and the trial reported them: fewer hip fractures and fewer cases of colorectal cancer. But on the central question the trial was built to answer, the conclusion was that combined HRT should not be used to prevent chronic disease in this population, because for that purpose the overall balance of risks exceeded the benefits.
The public and clinical reaction was dramatic and swift. Widely — and sometimes alarmingly — reported in the media, the WHI results caused prescriptions for hormone therapy to fall steeply within months, in the United States and internationally, as millions of women stopped treatment and physicians grew wary of prescribing it. After more than half a century of expanding use, the trajectory reversed almost overnight. It is important to present this carefully and accurately: the 2002 result was real, important, and rigorously obtained, and it appropriately ended the era of prescribing HRT as a routine preventive tonic for healthy women — but, as the next section explains, the headline figures were also widely over-generalized in ways that the subsequent decade of analysis substantially refined.
Aftermath and the Modern, Individualized View
The years after 2002 brought a more nuanced re-evaluation of the WHI — not a reversal of its core finding, but a careful reading of which women, which hormones, and at what age the risks and benefits actually applied to. Several points reshaped the picture. First, the second WHI arm, which gave estrogen alone (conjugated equine estrogens, in women who had had a hysterectomy and so did not need a progestin), told a different story when it was stopped in 2004: it showed an increased risk of stroke, but — importantly — no increase in breast cancer, and in fact a signal toward lower breast-cancer incidence. This indicated that much of the breast-cancer risk in the 2002 arm was linked to the particular progestin used in combination, not to estrogen as such.
Second, the WHI had enrolled women with an average age in their early 60s — many of them a decade or more past menopause — rather than the typical newly-menopausal woman in her early 50s seeking symptom relief. Later analyses gave rise to the “timing hypothesis”: the idea that the cardiovascular risk–benefit balance of hormone therapy may differ by age and by time since menopause, with the picture appearing more favourable (or at least less unfavourable) for healthy women who begin therapy near the onset of menopause and for short-term symptom relief, and less favourable when therapy is started many years later. The timing hypothesis is explicitly labelled here as a hypothesis — an influential and partly supported framework that has guided major guidelines, but one that remains an area of ongoing research and debate, not settled fact.
Third, attention turned to formulation and route. Modern menopause medicine increasingly favours transdermal estrogen (patches and gels), which appears to carry a lower risk of blood clots than older oral estrogens because it bypasses first-pass metabolism in the liver, and micronized progesterone in place of older synthetic progestins for endometrial protection. These distinctions — oral versus transdermal, synthetic progestin versus micronized progesterone — were largely flattened in the original 2002 headlines but are central to current individualized prescribing.
The settled modern consensus, reflected in contemporary guidance from menopause and women’s-health societies, is therefore neither the uncritical enthusiasm of the Feminine Forever era nor the blanket fear that followed 2002. Hormone therapy is now generally regarded as an effective and reasonable option for relieving bothersome menopausal symptoms — and for protecting bone — in appropriately selected women, particularly those who are under about 60 or within roughly ten years of menopause and without specific contraindications, using the most suitable formulation, dose, and route for that individual. It is not recommended as a general preventive treatment for chronic disease in healthy women, which is the specific practice the WHI rightly ended. The throughline of this whole history — from Gardanne’s careful naming, through the over-promising of mid-century marketing, to the hard randomized evidence of the WHI and its thoughtful reinterpretation — is a long, imperfect movement toward treating menopausal women with both scientific rigour and respect: taking their symptoms seriously, being honest about risks, and individualizing care rather than imposing a one-size-fits-all story.
Research Papers and References
The references below combine the landmark peer-reviewed trial publications and historical reviews behind this article with curated PubMed topic-search links into the broader literature. Where a specific paper is cited and confirmed, a direct DOI or PMID link is given; otherwise a PubMed topic search is provided. Historical primary sources — chiefly Gardanne’s 1821 De la ménopause, ou de l’âge critique des femmes and Robert A. Wilson’s 1966 Feminine Forever — are named in the article as historical documents rather than as modern citations. Each link opens in a new tab.
- Writing Group for the Women’s Health Initiative Investigators. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results From the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321–333. — doi:10.1001/jama.288.3.321
- Women’s Health Initiative Steering Committee. Effects of Conjugated Equine Estrogen in Postmenopausal Women With Hysterectomy (the estrogen-alone arm). JAMA. 2004;291(14):1701–1712. — doi:10.1001/jama.291.14.1701
- Hersh AL, Stefanick ML, Stafford RS. National Use of Postmenopausal Hormone Therapy: Annual Trends and Response to Recent Evidence. JAMA. 2004;291(1):47–53. — doi:10.1001/jama.291.1.47
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal Hormone Therapy and Health Outcomes During the Intervention and Extended Poststopping Phases of the Women’s Health Initiative Randomized Trials. JAMA. 2013;310(13):1353–1368. — doi:10.1001/jama.2013.278040
- Allen E, Doisy EA. An Ovarian Hormone: Preliminary Report on Its Localization, Extraction and Partial Purification, and Action in Test Animals. JAMA. 1923;81(10):819–821. — doi:10.1001/jama.1923.02650100027012
- Edward A. Doisy — Nobel Prize in Physiology or Medicine 1943 (awarded for vitamin K; biographical context for his estrogen work). — NobelPrize.org: Edward A. Doisy
- The discovery and isolation of estrone, estriol, and estradiol — the work of Edward Adelbert Doisy (history of estrogen biochemistry). — PubMed: discovery of estrone and estradiol (Doisy)
- Charles de Gardanne and the coinage and history of the term “menopause.” — PubMed: history of the term menopause (Gardanne)
- Houck JA. “What Do These Women Want?”: Feminist Responses to Feminine Forever, 1963–1980. Bulletin of the History of Medicine. 2003;77(1):103–132. — PMID: 12649555
- History and controversy of Premarin (conjugated equine estrogens) and the development of hormone therapy. — PubMed: history of Premarin and conjugated estrogens
- Unopposed estrogen, endometrial cancer risk, and the rationale for adding progestogens. — PubMed: unopposed estrogen and endometrial cancer
- The “timing hypothesis”: age, time since menopause, and the cardiovascular effects of hormone therapy. — PubMed: hormone therapy timing hypothesis
- Transdermal estrogen, micronized progesterone, and venous thromboembolism risk by formulation and route. — PubMed: transdermal estrogen and clot risk
- Medicalization, stigma, and the cultural history of menopause. — PubMed: medicalization and history of menopause
External Authoritative Resources
- National Institute on Aging (NIH) — Menopause
- The Menopause Society (formerly NAMS) — evidence-based menopause guidance
- Women’s Health Initiative — official study site
Connections
- Reproductive Medicine
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Menopause — the main overview of the life stage whose medical history this page traces.
- Menopause and Hormone Replacement Therapy (HRT)
- Perimenopause: The Under-Recognized Transition
- HRT Risks: Breast Cancer, Clots, and Stroke
- Micronized Progesterone vs. Synthetic Progestins
- Osteoporosis
- Postmenopausal Osteoporosis and Hormone Therapy
- Uterine Fibroids
- All Conditions