Pulmonary Edema
Pulmonary edema is a medical emergency in which fluid floods the air sacs of the lungs, making it impossible to breathe normally. It can develop in minutes or over days, depending on the cause, and carries a real risk of death if treatment is delayed. Understanding what drives it — and the crucial difference between the two main types — is the key to rapid, life-saving care.
Table of Contents
- What Is Pulmonary Edema?
- Cardiogenic vs Non-Cardiogenic: Two Very Different Diseases
- Cardiogenic Pulmonary Edema: Heart Failure Mechanism
- Non-Cardiogenic Pulmonary Edema: ARDS and Other Causes
- Symptoms: Recognizing an Emergency
- Diagnosis: CXR, BNP, Echocardiography
- Emergency Treatment: Position, Oxygen, Diuretics
- Long-Term Management and Prevention
- Key Research Papers
- Featured Videos
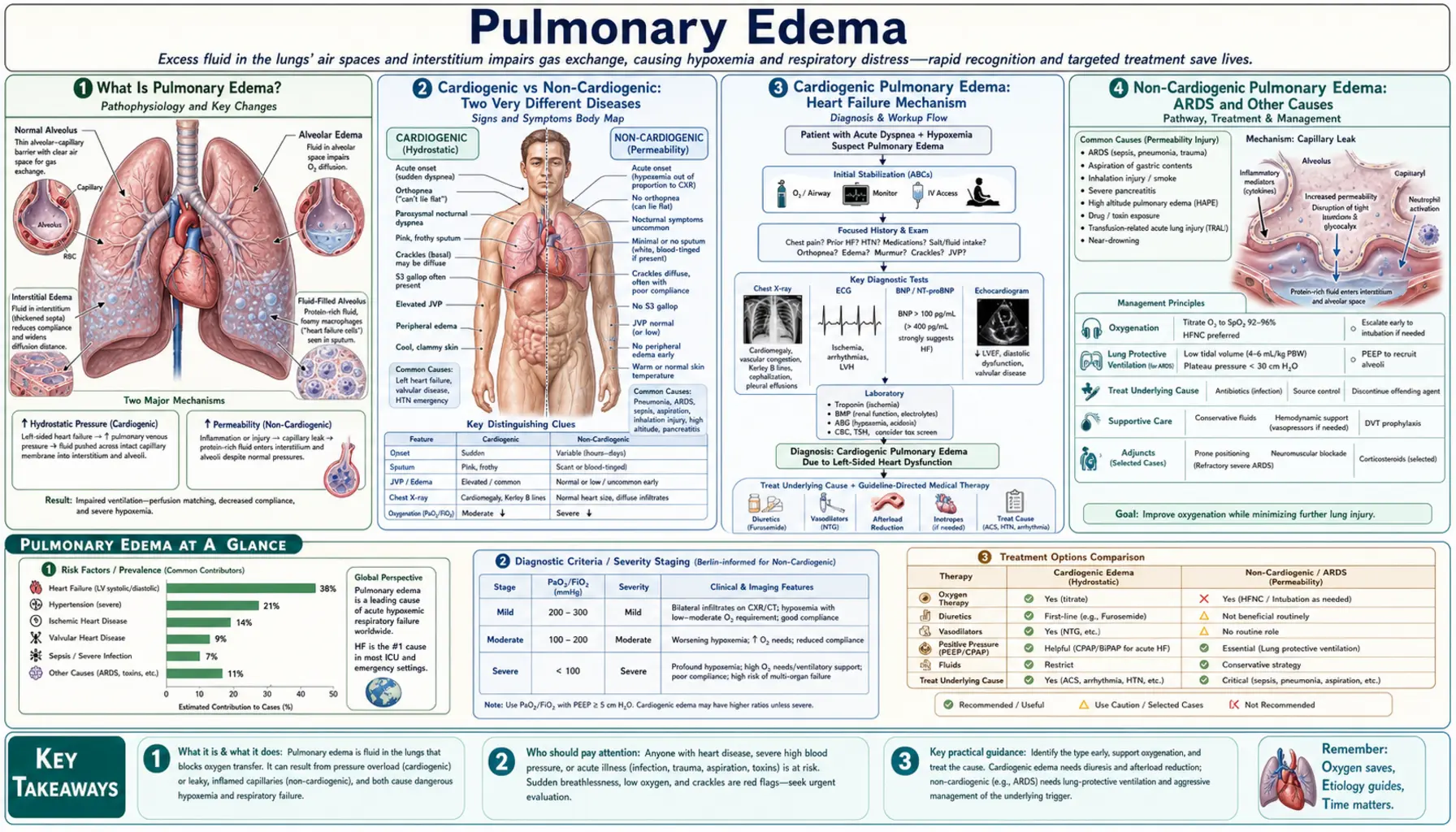
1. What Is Pulmonary Edema?
Your lungs contain roughly 300 million tiny air sacs called alveoli. Wrapped around each one is a mesh of capillaries so thin that oxygen and carbon dioxide pass directly through the walls. Pulmonary edema happens when fluid leaks out of those capillaries and accumulates first in the tissue surrounding the alveoli (the interstitium), then inside the alveoli themselves. Oxygen can no longer reach the bloodstream, and carbon dioxide can no longer escape. The result is suffocation from the inside.
This is distinct from pleural effusion, which is fluid collecting in the space around the lungs between the lung and chest wall. Pulmonary edema is fluid inside the lung tissue itself.
The progression follows a predictable two-stage pattern. In the first stage, fluid seeps into the interstitium — the scaffolding between alveoli. On a chest X-ray this shows up as Kerley B lines: short horizontal lines at the lung bases representing fluid-engorged lymphatic channels trying to drain the excess. In the second stage, the lymphatic system is overwhelmed and fluid spills into the alveoli themselves, dramatically worsening oxygen transfer.
The physics governing this process are described by the Starling equation. Fluid is pushed out of capillaries by hydrostatic pressure (the force of blood pushing outward) and pulled back in by oncotic pressure (the "suction" created by proteins dissolved in the blood). Normally these forces balance. Pulmonary edema results when hydrostatic pressure rises too high, oncotic pressure falls too low, or the capillary wall is damaged and becomes leaky regardless of pressures.
In the United States, pulmonary edema accounts for approximately 300,000 hospitalizations per year. Flash pulmonary edema — the sudden, catastrophic form — carries a mortality of 10–20% if not treated within the first hour. Even with treatment, in-hospital mortality for severe cases approaches 15%. These numbers make it one of the most time-sensitive emergencies in internal medicine.
2. Cardiogenic vs Non-Cardiogenic: Two Very Different Diseases
The most important question a clinician asks at the bedside is: is this coming from the heart or from somewhere else? The answer determines everything about treatment.
Cardiogenic pulmonary edema occurs when the left side of the heart fails to pump efficiently, causing pressure to back up into the pulmonary veins. That elevated venous pressure is transmitted forward into the pulmonary capillaries, raising hydrostatic pressure until fluid is pushed into the lung tissue. Think of it like a garden hose with a kink at the end — pressure builds upstream. The fluid that leaks out is a thin, protein-poor transudate because the capillary walls themselves are intact; only the pressure has changed.
The most common causes of cardiogenic pulmonary edema include:
- Acute decompensated heart failure (the leading cause overall)
- Acute myocardial infarction, especially when it damages the papillary muscles and causes sudden mitral regurgitation
- Hypertensive emergency (systolic blood pressure above 180 mmHg overwhelming the left ventricle)
- Severe mitral stenosis impairing outflow from the left atrium
- Cardiac tamponade or severe arrhythmias reducing cardiac output
Non-cardiogenic pulmonary edema happens when the capillary walls themselves are damaged by injury or inflammation. The heart's pressures may be completely normal. Instead, cytokines, toxins, or mechanical stress tear open the capillary endothelium, allowing a protein-rich exudate — including inflammatory cells — to flood the alveoli. This is the hallmark of ARDS.
Common causes of non-cardiogenic pulmonary edema include:
- Sepsis (the most common trigger for ARDS)
- Aspiration of stomach contents
- Near-drowning
- High-altitude pulmonary edema (HAPE) — a form of capillary stress failure at elevations above 2,500 meters
- Neurogenic pulmonary edema — seen after severe traumatic brain injury or subarachnoid hemorrhage
- Transfusion-related acute lung injury (TRALI)
- Smoke inhalation and toxic gas exposure
- Drug reactions (heroin, cocaine, salicylate overdose)
One measurable distinction separates the two: pulmonary capillary wedge pressure (PCWP), measured by a pulmonary artery catheter. In cardiogenic pulmonary edema, PCWP is above 18 mmHg because high left heart pressures are backing up. In non-cardiogenic edema, PCWP is normal or low — the heart pressures are fine, but the capillaries are leaking anyway. This distinction guided the original ARDS definition and still informs clinical decision-making today.
3. Cardiogenic Pulmonary Edema: Heart Failure Mechanism
To understand cardiogenic pulmonary edema, picture the circulatory pathway. Blood returns from the body into the right side of the heart, flows through the lungs to pick up oxygen, enters the left atrium, passes through the mitral valve into the left ventricle, and is pumped out to the body. Any failure in the left heart creates a traffic jam that backs up into the pulmonary circulation.
In left ventricular systolic failure — the most common form of heart failure — the heart muscle is weak and cannot squeeze effectively. With each beat, less blood is ejected forward, and more remains behind in the ventricle. The left ventricular end-diastolic pressure (LVEDP) climbs. This pressure is transmitted backward: left atrial pressure rises, then pulmonary venous pressure rises, and finally pulmonary capillary hydrostatic pressure exceeds the oncotic pulling force of the blood proteins. Fluid pours into the interstitium. The lymphatic channels that normally drain the lungs are overwhelmed within hours, and alveolar flooding follows.
In diastolic failure (heart failure with preserved ejection fraction, HFpEF), the ventricle squeezes normally but is stiff and cannot relax properly. During filling, it requires abnormally high pressures to accept blood — and those pressures again back up into the pulmonary veins. Diastolic failure now accounts for about half of all heart failure hospitalizations and is particularly common in older women with hypertension.
Flash pulmonary edema is the most dramatic presentation. It can develop within minutes rather than hours. The two most important triggers are:
- Acute myocardial infarction (MI): A heart attack injuring the posterior wall or the papillary muscles can cause sudden rupture of a mitral valve leaflet or chord. Acute mitral regurgitation means blood now gushes backward into the left atrium with every heartbeat. Left atrial pressure spikes, pulmonary pressures skyrocket, and the lungs fill within minutes. This is a surgical emergency.
- Hypertensive emergency: When systolic blood pressure climbs above 180 mmHg — sometimes reaching 220–240 — the left ventricle faces an acute afterload crisis. It cannot push blood out against such high resistance, LVEDP climbs, and the same cascade ensues. Blood pressure reduction of 20–25% in the first hour reverses the edema rapidly.
Mitral stenosis — typically a late complication of rheumatic fever — creates a fixed obstruction at the mitral valve. Blood cannot flow freely from the left atrium to the left ventricle. Left atrial pressure remains chronically elevated, and any additional stress (exercise, fever, atrial fibrillation with rapid rate) can precipitate acute pulmonary edema even when the left ventricle itself is entirely normal.
The common final pathway is always the same: elevated pulmonary venous pressure forces fluid through intact but pressure-overwhelmed capillary walls into the air spaces of the lungs.
4. Non-Cardiogenic Pulmonary Edema: ARDS and Other Causes
Non-cardiogenic pulmonary edema is caused by damage to the capillary endothelium — the one-cell-thick lining of the blood vessels. Once that barrier is breached, fluid and proteins pour freely into the alveoli regardless of cardiac pressures. The resulting injury pattern, when severe, is called ARDS.
Sepsis is the leading indirect cause. When bacteria, fungi, or viruses enter the bloodstream, the immune system launches a systemic inflammatory response. Cytokines like tumor necrosis factor-alpha, interleukin-1, and interleukin-6 flood the circulation. These molecules directly attack the endothelial cells of the pulmonary capillaries, opening gaps between them. Simultaneously, neutrophils migrate into the lung tissue and release enzymes that further degrade the barriers. The result is a protein-rich inflammatory exudate filling the alveoli — not the thin transudate of cardiogenic edema, but a thick sludge of proteins, immune cells, and cellular debris. Other indirect triggers include severe pancreatitis, massive blood transfusions, and major trauma.
Aspiration is the most common direct lung injury cause of non-cardiogenic edema. Stomach contents are highly acidic. When they enter the airway, the acid burns the epithelial cells lining the alveoli (type I pneumocytes) within seconds, triggering an intense inflammatory cascade. This is why aspiration during anesthesia, seizures, or altered consciousness is so dangerous.
High-altitude pulmonary edema (HAPE) is a unique and partially understood form. At high altitude, the reduced partial pressure of oxygen triggers hypoxic pulmonary vasoconstriction — a reflex that normally redirects blood from poorly ventilated regions to better-ventilated ones. But at altitude, hypoxia affects the whole lung. Vasoconstriction is uneven: some vessels constrict tightly while others remain open. The open vessels receive disproportionately high blood flow under high pressure. Eventually the walls of these high-flow capillaries fail mechanically — a process called capillary stress failure — and fluid leaks out. The edema is initially non-inflammatory but can progress to frank ARDS if not treated. HAPE develops most often on the second night after ascent above 2,500–3,000 meters and accounts for the majority of altitude-related deaths.
Neurogenic pulmonary edema follows severe brain injury — most commonly subarachnoid hemorrhage, severe traumatic brain injury, or status epilepticus. The Cushing response — the brain's emergency reflex to protect itself from herniation — generates a massive sympathetic discharge. Catecholamines surge. Alpha-adrenergic receptors in the pulmonary vasculature constrict, raising pulmonary arterial pressure dramatically. Simultaneously, the systemic vasoconstriction increases cardiac afterload, acutely impairing left ventricular function. This "blast" of high pressure combined with direct catecholamine toxicity on the endothelium opens the capillary barrier within minutes of the brain event. Neurogenic pulmonary edema is often self-limiting if the underlying neurological injury stabilizes, but it carries significant mortality in the acute phase.
TRALI (transfusion-related acute lung injury) occurs within 6 hours of blood product transfusion and is caused by donor antibodies against recipient neutrophil antigens, activating those neutrophils within the pulmonary capillaries. It is the leading cause of transfusion-associated mortality in the United States.
5. Symptoms: Recognizing an Emergency
Pulmonary edema rarely announces itself quietly. In most cases, the patient and anyone nearby know something is terribly wrong. Call 911 immediately if any of these symptoms appear — this is not a "wait and see" situation.
Sudden severe shortness of breath is the cardinal symptom. In cardiogenic pulmonary edema, it classically awakens patients from sleep between 2 and 4 in the morning. This timing is not random. During the day, gravity keeps fluid pooled in the legs and dependent tissues. When a person lies down to sleep, that fluid is redistributed — it returns to the central circulation, increases venous return to the heart, and raises pulmonary pressures. In a failing heart, this extra fluid load triggers alveolar flooding within 1–2 hours of lying down. The medical term for this pattern is paroxysmal nocturnal dyspnea (PND).
Orthopnea is the inability to breathe comfortably while lying flat. Patients learn to sleep with multiple pillows to keep their upper body elevated — gravity becomes their natural "diuretic." Clinicians actually use the number of pillows as a rough severity marker: two-pillow orthopnea is mild; sitting upright in a recliner is severe.
Pink frothy sputum is a sign of advanced alveolar flooding. As the alveoli fill with fluid, the surfactant lining (which normally keeps alveoli open) mixes with the plasma to create foam. Red blood cells leak through the damaged capillaries, tinting the foam pink. This is one of the most alarming signs in medicine — it means the patient is drowning in their own fluids.
Audible wheeze ("cardiac asthma") is common and frequently misdiagnosed as bronchial asthma. The wheeze arises not from bronchospasm in the conventional sense but from the edematous swelling of tissues surrounding the small airways — peribronchial cuffing — which narrows the airway lumen. The same bronchodilators used for asthma have limited effect here; treating the underlying cardiac pressure is what opens the airways.
Fine crackles (rales) are heard through a stethoscope, typically at the lung bases bilaterally, often extending upward as the edema worsens. They sound like the crackling of a piece of cellophane being slowly unrolled — caused by the sudden opening of fluid-collapsed alveoli with each inspiratory breath.
Additional signs of a body in crisis:
- Profuse sweating (diaphoresis) from extreme sympathetic activation
- Cyanosis — bluish discoloration of lips and fingertips from severe hypoxemia
- Extreme restlessness or panic — the body's primal response to suffocation
- The classic position: patient sitting bolt upright, leaning slightly forward, hands gripping the bed rail or knee, gasping with every breath
- Inability to speak more than two or three words between breaths
- Heart rate typically above 120 beats per minute
Any patient presenting in this posture with this constellation of signs requires immediate treatment — there is no time to wait for lab results before starting oxygen and positioning.
6. Diagnosis: CXR, BNP, Echocardiography
While emergency treatment often begins on clinical grounds alone, several tests confirm the diagnosis and guide the distinction between cardiogenic and non-cardiogenic edema.
Chest X-Ray (CXR)
The portable chest X-ray is the most immediately available diagnostic tool in the emergency room. Classic findings in pulmonary edema include:
- Bilateral alveolar opacities — the "bat wing" or "butterfly" pattern: dense white areas radiating from both hila (the central structures where major blood vessels enter the lungs), typically sparing the costophrenic angles at the bases and the outer edges of the lungs.
- Cardiomegaly — an enlarged cardiac silhouette on CXR, suggesting the underlying heart failure. The cardiothoracic ratio (heart width divided by chest width) exceeding 0.50 is abnormal.
- Kerley B lines — short, sharp horizontal lines, 1–2 cm in length, at the very bases of the lungs near the outer edges of the chest. These represent fluid-engorged interlobular lymphatic channels — the lymphatic drainage system overloaded in early pulmonary edema. They are among the earliest X-ray signs.
- Upper lobe vascular redistribution — normally, blood vessels visible in the upper lung fields are smaller than those at the bases. In elevated pulmonary venous pressure, the upper lobe vessels dilate and become more prominent than the lower lobe vessels — the vascular pattern "flips."
- Pleural effusions — small amounts of fluid collecting in the pleural space are common in cardiogenic edema because the same elevated venous pressures that cause alveolar flooding also cause fluid to weep through the visceral pleura.
- Peribronchial cuffing — fluid accumulating around the large bronchi creates a "cuff" visible on X-ray, thickening the bronchial walls.
BNP and NT-proBNP
B-type natriuretic peptide (BNP) is a hormone released by the ventricles in response to wall stress — the heart's signal to the kidneys to excrete salt and water. It is the most useful blood test for distinguishing cardiogenic from non-cardiogenic pulmonary edema:
- BNP below 100 pg/mL effectively rules out cardiogenic etiology in most patients.
- BNP above 500 pg/mL strongly suggests heart failure as the underlying cause.
- BNP 100–500 pg/mL is a gray zone requiring additional clinical context; causes include pulmonary embolism, sepsis, and renal failure, which can all modestly elevate BNP without true cardiogenic edema.
NT-proBNP (the N-terminal fragment) has different cutoffs: below 300 pg/mL rules out heart failure; above 900 pg/mL (age-stratified to 450 for under 50, 900 for 50–75, and 1800 for over 75) suggests it.
Point-of-Care Ultrasound (POCUS)
Bedside ultrasound has transformed emergency diagnosis of pulmonary edema. The BLUE protocol (Bedside Lung Ultrasound in Emergency) uses lung ultrasound findings to distinguish pulmonary edema from other causes of acute breathlessness with high accuracy.
The key finding is B-lines — vertical hyperechoic streaks arising from the pleural line and extending to the bottom of the screen without fading. More than three B-lines per lung zone, bilateral, indicates interstitial edema. A full lung ultrasound showing bilateral diffuse B-lines in a patient with shortness of breath strongly suggests cardiogenic pulmonary edema — and this finding can be obtained in under two minutes.
Cardiac ultrasound simultaneously assesses left ventricular function, wall motion abnormalities suggesting MI, valve abnormalities, and pericardial effusion — information that guides immediate treatment decisions.
Additional Tests
- Electrocardiogram (ECG): Essential to identify acute MI as the trigger. Look for ST elevation, new left bundle branch block, or signs of posterior MI.
- Troponin: Elevated in acute MI causing flash pulmonary edema. Even modest troponin elevations from myocardial stress are common in severe pulmonary edema without MI.
- Arterial blood gas (ABG): Hypoxemia (low PaO2) is universal. Early in the course, tachypnea blows off CO2, causing hypocapnia (low PaCO2) and respiratory alkalosis. Rising PaCO2 — the patient transitioning from hypocapnia to normocapnia to hypercapnia — signals impending respiratory failure and the need for ventilatory support.
- Complete metabolic panel: Assess renal function (guides diuretic dosing), electrolytes (hyponatremia common in heart failure), and liver function (hepatic congestion).
7. Emergency Treatment: Position, Oxygen, Diuretics
The emergency treatment of cardiogenic pulmonary edema follows a logical sequence targeting the underlying physiology. The goal is to reduce the pressure forcing fluid into the lungs while supporting oxygenation until the lungs can clear.
Positioning
The simplest and fastest intervention is positioning the patient upright — sitting straight up, legs dangling off the side of the bed if possible. This is not merely for comfort. The upright position allows gravity to pool blood in the legs and abdominal veins, reducing venous return to the right heart, which reduces pulmonary blood flow and pulmonary venous pressure. This "auto-preload reduction" begins within seconds and can measurably improve oxygenation before any medication is given.
Oxygen and Non-Invasive Ventilation
High-flow supplemental oxygen is given immediately to correct hypoxemia. If standard oxygen masks are insufficient — if oxygen saturation remains below 90% or the patient is tiring from the work of breathing — non-invasive positive pressure ventilation (NIV) is the next step.
Both CPAP (continuous positive airway pressure) and BiPAP (bilevel positive airway pressure) work by delivering pressurized air through a tight-fitting mask. The positive pressure "splints" the alveoli open, prevents them from collapsing with each breath, and drives fluid back across the alveolar membrane. Equally important, positive intrathoracic pressure reduces both preload and afterload on the left ventricle, directly addressing the cardiogenic mechanism.
The landmark 3CPO trial (Gray et al., 2008) demonstrated that NIV significantly reduces the need for endotracheal intubation in acute cardiogenic pulmonary edema compared to standard oxygen therapy, and meta-analyses including the Masip 2005 Lancet analysis confirmed a mortality benefit. NIV is strongly preferred over intubation when patients are conscious and cooperative, because intubation itself carries significant risks in this setting.
Furosemide (Loop Diuretics)
Intravenous furosemide (Lasix) is the cornerstone pharmacological treatment for cardiogenic pulmonary edema. It works in two phases:
- Immediate venodilation: Within 5–15 minutes of IV injection, furosemide causes dilation of the venous capacitance vessels throughout the body. Blood pools peripherally, reducing venous return to the heart and thereby reducing pulmonary pressures — before any diuresis has occurred. This early effect is the most clinically important in acute edema.
- Diuresis: Over the following 1–2 hours, furosemide acts on the kidney's loop of Henle to block sodium and water reabsorption, producing a large volume of urine. This removes the excess fluid volume that has been overloading the circulation.
Standard initial dosing in the emergency setting is 40–80 mg IV for patients not previously on diuretics, with higher doses for those with chronic kidney disease or who are already taking oral furosemide. Urine output is monitored closely to titrate the dose.
Nitrates
Nitroglycerin — given sublingually (under the tongue), as a paste on the skin, or intravenously — is a powerful vasodilator that reduces both preload and afterload. It is particularly effective in hypertensive pulmonary edema, where the underlying problem is an afterload crisis rather than volume overload. Blood pressure reduction of 20–25% in the first hour can produce dramatic resolution of symptoms.
Nitroglycerin is contraindicated if systolic blood pressure is below 90 mmHg (it will worsen hypotension) or if there is right ventricular failure (right heart failure depends on adequate preload to function).
Morphine — A Controversial Choice
Morphine was historically given in pulmonary edema for its anxiolytic effect and its mild vasodilatory properties. However, analysis of the ADHERE registry (Peacock et al., 2008) — a large real-world database of over 100,000 acute heart failure admissions — found that morphine use was independently associated with worse outcomes, including higher rates of ICU admission and mechanical ventilation, and a higher mortality signal. Most centers now avoid morphine in acute pulmonary edema and prefer benzodiazepines if anxiolysis is needed.
Treating the Underlying Cause
- Acute MI: Emergent percutaneous coronary intervention (PCI) to reopen the blocked artery is the definitive treatment. Door-to-balloon time targets apply even more urgently when MI has caused pulmonary edema.
- Hypertensive emergency: Intravenous antihypertensives (labetalol, nicardipine, clevidipine) titrated to reduce blood pressure 20–25% within one hour.
- Acute mitral regurgitation: Afterload reduction to minimize the regurgitant fraction, followed by urgent surgical consultation for valve repair or replacement.
- Cardiogenic shock (pulmonary edema plus low blood pressure): Inotropes such as dobutamine to improve cardiac contractility; vasopressors if blood pressure fails to respond; mechanical circulatory support (intra-aortic balloon pump, Impella) in refractory cases.
- HAPE: Immediate descent of at least 300–500 meters. Supplemental oxygen. Portable hyperbaric chambers if descent is impossible. Nifedipine (10 mg immediate-release followed by slow-release 30 mg twice daily) or sildenafil to reduce pulmonary artery pressure. Dexamethasone has been used adjunctively.
8. Long-Term Management and Prevention
For most patients whose pulmonary edema was caused by heart failure, surviving the acute event is only the beginning. Without addressing the underlying heart disease, the cycle of decompensation and rehospitalization continues. Roughly 25% of heart failure patients are rehospitalized within 30 days of discharge — one of the highest readmission rates in medicine.
Guideline-Directed Medical Therapy for Heart Failure
Four classes of medications have been proven in large randomized trials to reduce death and hospitalization in heart failure with reduced ejection fraction (HFrEF). Together they are called the "fantastic four" of heart failure medicine:
- ACE inhibitors or ARBs (or the newer ARNi sacubitril/valsartan — brand name Entresto): Reduce afterload and prevent cardiac remodeling. The PARADIGM-HF trial (McMurray et al., 2014) showed sacubitril/valsartan reduced cardiovascular mortality by 20% compared to enalapril alone.
- Beta-blockers (carvedilol, metoprolol succinate, bisoprolol): Slow the heart rate, reduce myocardial oxygen demand, and counteract the chronic sympathetic overdrive that worsens heart failure. Must be started when the patient is stable and dry, not during acute decompensation.
- Aldosterone antagonists (spironolactone, eplerenone): Block the harmful effects of aldosterone on the heart and kidneys, reducing fluid retention and cardiac fibrosis.
- SGLT2 inhibitors (dapagliflozin, empagliflozin): Originally developed for diabetes, these agents have emerged as transformative heart failure drugs. The DAPA-HF trial (McMurray et al., 2019) showed dapagliflozin reduced the combined risk of worsening heart failure or cardiovascular death by 26%, including in patients without diabetes. The mechanism is not fully understood but includes mild diuresis, reduction in cardiac preload and afterload, and possibly direct cardiac metabolic benefits.
Lifestyle and Self-Monitoring
- Sodium restriction: Limiting dietary sodium to less than 2 grams per day reduces fluid retention significantly. This means avoiding processed foods, canned goods, fast food, and added table salt. Even small amounts of hidden sodium (bread, condiments) can tip a compensated patient into decompensation.
- Fluid restriction: Many patients with severe heart failure are also asked to limit total fluid intake to 1.5–2 liters per day.
- Daily weight monitoring: Weighing every morning after urination, before eating, and recording the number. An increase of more than 2 pounds (roughly 1 kg) in 24 hours, or 5 pounds over a week, indicates fluid retention — the patient should call their cardiologist before symptoms develop. This simple habit has been shown to reduce emergency department visits and hospitalizations.
- Medication adherence: Most heart failure decompensations can be traced to stopping diuretics, eating salty foods, or missing other medications. Pharmacy pill-organizers, blister packs, and automated reminders substantially improve adherence.
Prevention of High-Altitude Pulmonary Edema
For individuals known to be susceptible to HAPE (defined as a prior episode), prevention strategies before planned altitude ascent include:
- Gradual ascent — no more than 300–500 meters increase in sleeping altitude per day above 2,500 meters, with a rest day every 3 days ("climb high, sleep low")
- Acetazolamide 125–250 mg twice daily starting 24 hours before ascent (stimulates breathing, reduces altitude sickness)
- Nifedipine SR 30 mg twice daily as a prophylactic pulmonary vasodilator in high-risk individuals
- Avoiding heavy exertion on the first day at a new altitude
- Immediate descent at the first sign of symptoms — never sleep at altitude if HAPE symptoms have begun
Prevention of Neurogenic Pulmonary Edema
Neurogenic pulmonary edema follows the brain injury — preventing it means preventing or rapidly treating the underlying injury (subarachnoid hemorrhage, TBI, seizures). Once it occurs, supportive care with lung-protective ventilation and treatment of the underlying neurological condition allows most cases to resolve within 24–72 hours as the catecholamine surge subsides.
9. Key Research Papers
-
Masip J, Roque M, Sanchez B, et al. Non-invasive ventilation in acute cardiogenic pulmonary oedema: systematic review and meta-analysis.
Lancet. 2005;365(9463):1025–1031 — Search PubMed.
DOI: 10.1016/S0140-6736(05)74313-0.
Meta-analysis establishing the mortality and intubation benefit of non-invasive ventilation in acute cardiogenic pulmonary edema. -
Gray A, Goodacre S, Newby DE, et al. Noninvasive Ventilation in Acute Cardiogenic Pulmonary Edema (3CPO Trial).
N Engl J Med. 2008;359(2):142–151 — Search PubMed.
DOI: 10.1056/NEJMoa0707992.
Landmark UK randomized trial showing NIV significantly reduced need for intubation versus standard oxygen therapy. -
Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid Measurement of B-Type Natriuretic Peptide in the Emergency Diagnosis of Heart Failure.
N Engl J Med. 2002;347(3):161–167 — Search PubMed.
DOI: 10.1056/NEJMoa020233.
Established the diagnostic cutoffs for BNP in distinguishing cardiac from non-cardiac causes of dyspnea in the emergency department. -
McMurray JJV, Packer M, Desai AS, et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure (PARADIGM-HF).
N Engl J Med. 2014;371(11):993–1004.
PMID: 25176015.
DOI: 10.1056/NEJMoa1409077.
Showed sacubitril/valsartan reduced cardiovascular mortality by 20% versus enalapril, changing heart failure guidelines worldwide. -
McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction (DAPA-HF).
N Engl J Med. 2019;381(21):1995–2008.
PMID: 31535829.
DOI: 10.1056/NEJMoa1911303.
Established SGLT2 inhibitors as a pillar of heart failure therapy, reducing worsening heart failure events and mortality by 26%. -
Peacock WF, Hollander JE, Diercks DB, et al. Morphine and outcomes in acute decompensated heart failure: an ADHERE analysis.
Emerg Med J. 2008;25(4):205–209.
PMID: 18356349.
DOI: 10.1136/emj.2007.050419.
Registry analysis of over 100,000 patients showing morphine use in acute heart failure associated with higher rates of mechanical ventilation and in-hospital mortality. -
Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound.
Intensive Care Med. 2012;38(4):577–591.
PMID: 22392031.
DOI: 10.1007/s00134-012-2513-4.
International consensus defining the role of lung ultrasound B-lines in the diagnosis of pulmonary edema and ARDS at the bedside. -
Bartsch P, Swenson ER. Clinical practice: Acute high-altitude illnesses.
N Engl J Med. 2013;368(24):2294–2302 — Search PubMed.
DOI: 10.1056/NEJMcp1214870.
Authoritative clinical review of HAPE pathophysiology, presentation, and evidence-based management including nifedipine and descent protocols. -
Ware LB, Matthay MA. The acute respiratory distress syndrome.
N Engl J Med. 2000;342(18):1334–1349 — Search PubMed.
DOI: 10.1056/NEJM200005043421806.
Seminal review defining the pathophysiology of non-cardiogenic pulmonary edema, capillary leak, and the ARDS spectrum. -
Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure.
J Am Coll Cardiol. 2017;70(6):776–803.
PMID: 28461007.
DOI: 10.1016/j.jacc.2017.04.025.
Official US guideline update incorporating SGLT2 inhibitors and sacubitril/valsartan into the heart failure treatment algorithm. -
Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure.
Eur Heart J. 2016;37(27):2129–2200.
PMID: 27206819.
DOI: 10.1093/eurheartj/ehw128.
Comprehensive European guidelines covering acute decompensated heart failure, pulmonary edema management, and long-term secondary prevention. -
Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension.
Eur Heart J. 2016;37(1):67–119.
PMID: 26320113.
DOI: 10.1093/eurheartj/ehv317.
Comprehensive guidelines covering the role of pulmonary hypertension in cardiogenic pulmonary edema and hemodynamic classification.
Search PubMed for More Research
- Pulmonary edema treatment
- Cardiogenic pulmonary edema
- Non-invasive ventilation acute pulmonary edema
- BNP heart failure diagnosis
- High altitude pulmonary edema
- Neurogenic pulmonary edema