Hoarding Disorder
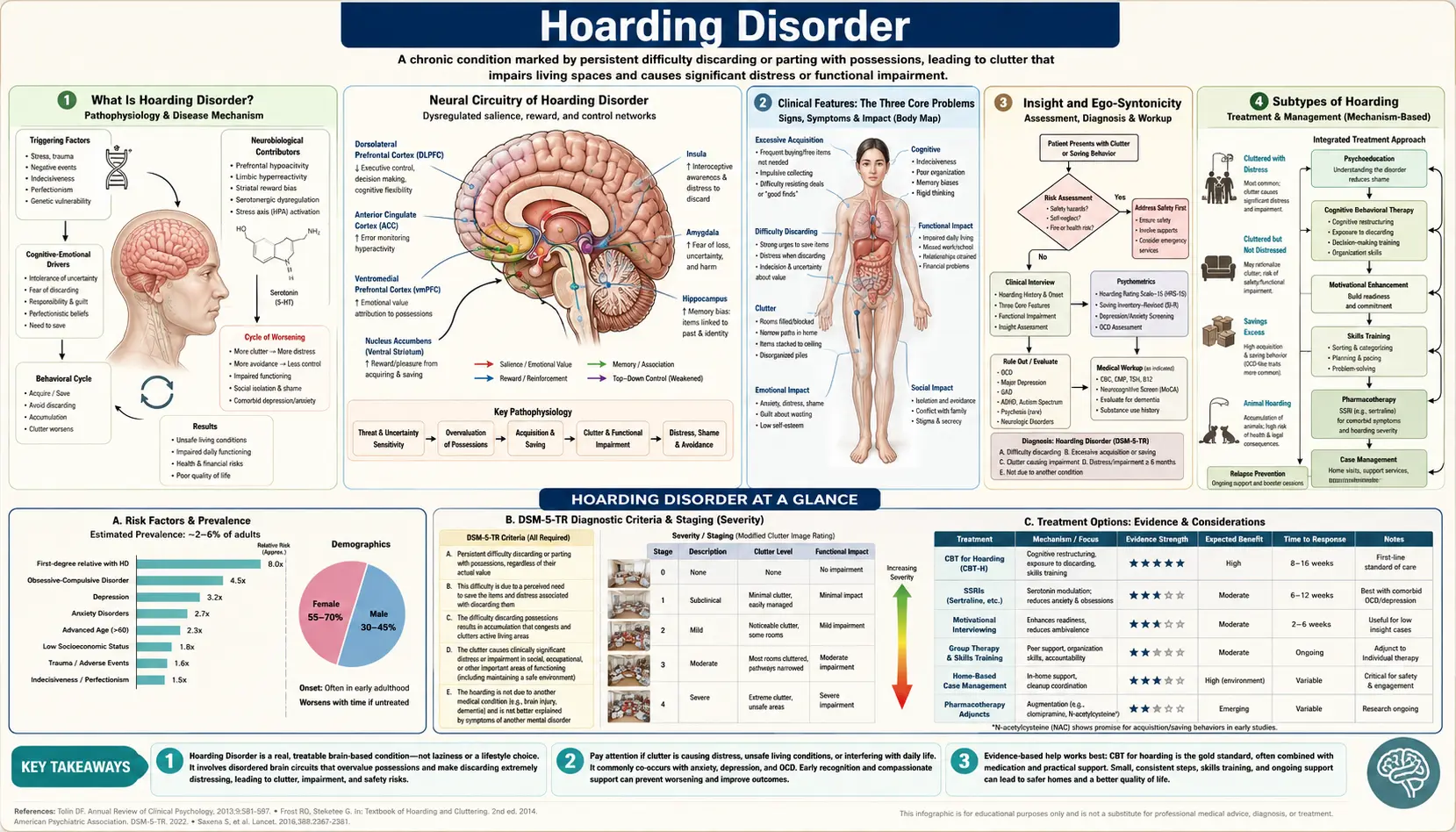
Table of Contents
- What Is Hoarding Disorder?
- The Three Core Problems
- Insight and Ego-Syntonicity
- Subtypes of Hoarding
- Brain Science of Hoarding
- Who Gets Hoarding Disorder?
- Treatment — CBT Adapted for Hoarding
- Treatment — Medications and Other Approaches
- Safety and Crisis Issues
- Living With Hoarding and Recovery
- Key Research Papers
- Connections
- Featured Videos
What Is Hoarding Disorder?
Hoarding Disorder (HD) is an officially recognized psychiatric condition listed in the DSM-5 under Obsessive-Compulsive and Related Disorders. At its core, it involves a persistent difficulty discarding or parting with possessions, regardless of their actual monetary or practical value. Over time, this difficulty leads to the accumulation of enormous quantities of items that clutter and compromise living spaces to the point where those spaces can no longer be used for their intended purpose.
This is not simply a messy house or being a pack rat. The clutter in Hoarding Disorder is severe enough to create genuine health and safety hazards — fire risks from stacked paper, fall risks from narrowed walkways, sanitation problems from rotting food or pest infestations — and it causes significant distress or impairment in daily functioning. Relationships suffer. Financial problems mount. Isolation deepens as people feel too ashamed to have anyone in their home.
It is important to understand what Hoarding Disorder is not. It is distinct from OCD in critical ways: the two conditions have different neural bases, respond differently to the same treatments, and — perhaps most importantly — differ fundamentally in how the person perceives their own behavior. In OCD, people typically recognize their obsessions as irrational and unwanted. In Hoarding Disorder, the person usually feels their saving behavior is entirely justified. HD also has different, and generally worse, treatment outcomes than OCD.
Hoarding Disorder is equally distinct from collecting. Collectors are organized and systematic; they know exactly what they have, they display their items with pride, and their collection has some recognized value to a community of others (stamps, coins, vintage records). Hoarding is chaotic, often hidden from others out of shame, and the value assigned to items is intensely personal and idiosyncratic — an empty yogurt container saved "because it might be useful someday" carries the same emotional weight as a family heirloom.
Clinical Features: The Three Core Problems
Hoarding Disorder is built on three interlocking clinical features. Understanding all three helps explain why the disorder is so persistent and why simply telling someone to clean up does not work.
Difficulty Discarding
The emotional experience of discarding a possession — even a worthless one — can feel genuinely distressing to someone with Hoarding Disorder. This is not stubbornness or laziness; it is a real psychological reaction rooted in specific beliefs about possessions. Common belief categories include:
- "I might need it someday" — a strong overestimation of future utility, combined with intolerance for the uncertainty of not having something available.
- "It's wasteful to throw it away" — a deep ethical discomfort with perceived wastefulness, even for objects that have no realistic use.
- Sentimental value — the item feels like a container of memory; discarding it feels like losing the experience itself.
- Information value — newspapers, magazines, and printouts must be kept because they contain knowledge the person might one day need.
Excessive Acquisition
Many people with Hoarding Disorder do not merely struggle to discard — they also actively acquire new items at a rate that exceeds their ability or desire to discard. Research suggests that roughly 70% of people with HD engage in compulsive buying. Others collect free items: picking up discarded objects from sidewalks, dumpster diving, or bringing home every free pamphlet, sample, or promotional item they encounter. This combination of high intake and near-zero outflow creates the relentless accumulation that defines the disorder.
Clutter That Compromises Living Spaces
The defining clinical consequence is clutter so severe that primary living areas — the kitchen, bedroom, living room, bathroom — can no longer be used for their intended purpose. A kitchen buried under boxes cannot be used for cooking. A bed covered in stacked clothing cannot be slept in. A bathroom whose floor is impassable cannot be safely used. Beyond inconvenience, this creates real physical danger: fire hazards from stacked paper near heat sources, fall hazards from navigating narrow passages, infection risks from rodent or insect infestations, and in extreme cases structural damage to the home itself. When animals are present, they too may be in danger.
Insight and Ego-Syntonicity
One of the most clinically important features of Hoarding Disorder — and one that makes treatment so challenging — is that hoarding behavior is typically ego-syntonic. This means the person experiences their saving and collecting as consistent with their own values, desires, and sense of self. It feels right. It feels reasonable. The collection feels necessary and even meaningful.
As a result, people with Hoarding Disorder almost never arrive at a therapist's office because they recognized a problem in themselves. They are far more commonly pushed toward help by outside forces: a family member who can no longer tolerate the conditions, a landlord threatening eviction, a housing authority conducting an inspection, or Adult Protective Services responding to a welfare concern. This means the very first challenge in treatment is not teaching skills — it is establishing a therapeutic alliance with someone who may not believe they need to be there.
Contrast this with OCD, where obsessions are ego-dystonic: the person knows their intrusive thoughts are irrational, unwanted, and inconsistent with who they are. That recognition of the problem, while distressing, actually makes engagement in treatment somewhat easier. A person with OCD wants the obsessions to stop. A person with Hoarding Disorder often wants to be left alone with their possessions.
Low insight also means that motivational interviewing is not just a nice add-on to treatment — it is a clinical necessity. Without carefully exploring the person's own values, goals, and the ways in which hoarding has cost them things they care about (relationships, mobility, health, self-respect), there is no foundation for change. Standard directive therapy tends to produce dropout and resentment rather than progress.
Subtypes of Hoarding
Animal Hoarding
Animal hoarding is perhaps the most severe and most widely recognized subtype. It involves keeping far more animals than a person can adequately care for, with the result that the animals suffer neglect — inadequate food, water, veterinary care, and sanitation. The living environment becomes severely contaminated with animal waste, creating serious public health hazards. Animal hoarding is also an animal welfare emergency that typically requires involvement from animal control authorities alongside mental health services.
Animal hoarders most commonly come to attention through public complaints or animal welfare inspections. They are disproportionately elderly women, though it occurs across demographics. What distinguishes animal hoarding psychologically is an intense set of attachment beliefs: the person genuinely believes that only they can provide proper care for these animals, that shelters will euthanize them, or that the animals would be lost without them. This belief system is resistant to evidence and makes intervention extremely difficult. Recovery rates for animal hoarding are among the lowest of any hoarding presentation.
Digital Hoarding
An increasingly recognized subtype, digital hoarding involves the accumulation of enormous quantities of digital files — emails in the tens of thousands, screenshots saved by the thousands, downloaded documents that are never read, photo libraries in the hundreds of gigabytes, browser bookmarks numbering in the thousands. The same psychological mechanisms are at work: difficulty discarding digital items, beliefs about future usefulness, and a sense that deleting a file means losing something irreplaceable.
Digital hoarding tends to cause less visible impairment — you cannot see a cluttered hard drive — but it creates real occupational dysfunction: inability to locate needed files, anxiety about device storage limits, hours spent "organizing" without progress, and occupational disruption when work computers or email inboxes become unmanageable. As our lives become more digital, this subtype is likely to become more clinically prominent.
Food Hoarding
Food hoarding involves the stockpiling of food far beyond what could realistically be consumed, often including expired or spoiled items that the person cannot bring themselves to discard. This creates hygiene hazards (mold, rodent attraction), health risks from consumption of spoiled food, and in severe cases a kitchen environment that has become unusable. Food hoarding sometimes occurs in the context of childhood food insecurity — the person learned early that food might disappear, and that lesson became embedded in their relationship to food even when scarcity is no longer a reality.
Brain Science of Hoarding
Research over the past two decades has revealed that Hoarding Disorder involves distinct brain-based differences in executive function, emotional processing, and decision-making — and that these differences are meaningfully different from what is seen in OCD, explaining why the two conditions respond so differently to treatment.
Executive Dysfunction and Categorization Deficits
One of the most consistent findings in hoarding research is that people with HD struggle enormously with categorization. When a person without HD looks at a piece of paper on their desk, they can quickly decide: file it, read it, recycle it. They have a mental schema into which the object fits. People with Hoarding Disorder often cannot do this — every item exists in its own unique, uncategorizable category, making every disposal decision a unique and effortful challenge. When you cannot decide where something goes, the path of least resistance is to keep it. Multiply this by every object in a house containing tens of thousands of items, and you begin to understand the scale of the problem.
Attention and ADHD Comorbidity
Between 40% and 60% of people with Hoarding Disorder also have ADHD. This is not a coincidence. ADHD involves difficulties with sustained attention, working memory, and the ability to follow through on decisions — all of which are required for the sustained, effortful work of sorting and discarding. A person with both conditions faces a double burden: they struggle to make categorization decisions (HD) and they also struggle to maintain the attention needed to work through a pile systematically (ADHD). Treating the ADHD — with medications, behavioral strategies, or both — can significantly improve a person's capacity to engage in the work of clutter reduction.
Emotional Attachment and Neural Responses
Brain imaging studies have revealed something striking about what happens when people with Hoarding Disorder are asked to consider discarding a possession. When they contemplate throwing something away, brain regions associated with pain, threat, and homeostatic disruption — particularly the insula and the anterior cingulate cortex — show heightened activation. In other words, discarding a possession activates a response that feels, neurologically, like a physical threat or a violation of the body's natural state.
This helps explain the subjective experience many people with HD describe: discarding items feels genuinely painful, almost like losing a part of themselves. Items are experienced not merely as objects but as extensions of identity, repositories of memory, and representations of a possible future self. The empty yogurt container is not just an empty yogurt container — it is the possibility of making yogurt parfaits someday, of being the kind of person who is prepared. Discarding it means discarding that future possibility.
A Different Brain Circuit Than OCD
Brain imaging studies comparing HD directly to OCD have found that the two conditions involve distinct neural circuitry. OCD is primarily associated with the frontostriatal circuit — the loop between the prefrontal cortex and the striatum that governs habitual, repetitive behaviors. Hoarding Disorder shows a different pattern, with greater involvement of the anterior cingulate cortex and left hemisphere prefrontal regions involved in decision-making and emotional significance.
Serotonin plays a role in both conditions, but the circuitry differs, which is one reason why the serotonin reuptake inhibitors (SSRIs) that work so well in OCD show only modest effects in Hoarding Disorder. The treatment approach must be tailored to the actual brain mechanisms involved — and those mechanisms are meaningfully different.
Who Gets Hoarding Disorder?
Hoarding Disorder is more common than most people realize. Community surveys suggest a prevalence of approximately 2–6% in the adult population, making it roughly as common as OCD itself. Prevalence increases significantly with age, and the disorder is most often recognized in people in their 40s and beyond — even though symptoms typically begin much earlier.
Age of Onset
Most people with Hoarding Disorder can trace their saving behavior back to adolescence, often to age 11–15. The behavior tends to worsen gradually over decades. By the time someone is in their 30s or 40s, years of accumulation have created a home environment that is visibly impaired, and the condition may finally come to outside attention. This long latency between onset and recognition means that by the time treatment is sought, hoarding behaviors are deeply ingrained and have had decades to become habitual.
Family History
Hoarding Disorder runs in families. Approximately 50% of people with HD report a first-degree relative — a parent, sibling, or child — who also had significant hoarding behaviors. Twin studies suggest a substantial genetic component, though the specific genes involved are not yet well characterized. Growing up in a hoarding household also shapes a person's relationship to objects and can normalize accumulation behaviors regardless of genetic inheritance.
Life Stressors as Triggers
While hoarding typically begins early, major life stressors often precipitate or dramatically worsen the behavior. Bereavement is a particularly common trigger — losing a loved one can intensify the emotional significance of possessions as reminders of the deceased, making discarding feel like a second loss. Divorce, serious illness, job loss, and other major transitions can similarly activate or intensify hoarding behavior. Understanding what stress precipitated a worsening episode is often clinically important in treatment.
Comorbidities
Hoarding Disorder rarely travels alone. Common co-occurring conditions include:
- ADHD (40–60%) — the most common comorbidity, and one that directly worsens hoarding-related decision-making deficits
- Major Depression (50–75%) — often secondary to the shame, isolation, and functional impairment caused by hoarding
- Anxiety Disorders (approximately 50%) — including generalized anxiety disorder and panic disorder
- Social Anxiety Disorder — the fear of having others see the home creates a self-reinforcing cycle of isolation
- OCD (15–25%) — HD can co-occur with OCD, but the two are phenomenologically very different and should be treated as separate conditions when both are present
Treatment — CBT Adapted for Hoarding
The most evidence-based treatment for Hoarding Disorder is Cognitive-Behavioral Therapy specifically adapted for HD (CBT-HD), developed primarily by Gail Steketee and Randy Frost. Standard CBT as used for depression or other anxiety disorders is not sufficient — the approach requires specific modifications to address the unique features of hoarding, particularly low insight and the need to work with actual possessions in the actual home environment.
Motivational Enhancement: The Essential First Step
Before skills-building can begin, treatment typically starts with motivational enhancement — a structured process of exploring why change matters to this specific person. The therapist helps the person identify their own values (meaningful relationships, safety, a comfortable home, financial stability) and gently explore the discrepancy between those values and the reality of their current living situation. This is done without confrontation or judgment, using a collaborative, exploratory stance. Without this foundation, the person is likely to comply superficially in sessions but not change at home — or to drop out of treatment entirely.
Skills Training
A major component of CBT-HD is building the specific cognitive skills that hoarding impairs. This includes:
- Categorization practice — learning to apply consistent decision-making rules to objects rather than treating every item as unique
- Sorting hierarchies — developing a systematic approach to working through piles ("start with the easiest items, build confidence, work toward harder ones")
- Decision-making strategies — rules like "would I buy this today if I didn't already own it?" or "do I have a specific plan for using this in the next six months?"
Exposure: Practicing Discarding
As in other anxiety-based conditions, exposure is a central treatment component. The person practices the act of discarding — starting with items that carry low emotional weight and working gradually up a hierarchy toward more meaningful possessions. Each successful discard experience provides evidence against the catastrophic belief that discarding is intolerable or irreversible. Over many sessions, the distress associated with discarding decreases.
Home Visits: Essential, Not Optional
Unlike most CBT, effective treatment for Hoarding Disorder essentially requires working in the person's actual home environment. Seeing and touching the real possessions is necessary — a clinical office cannot replicate what it feels like to stand in front of a particular pile of objects. Telehealth approaches using a video camera to view the home have been shown to be effective when in-person visits are not possible, but the home environment must be part of treatment.
Realistic Expectations
Recovery from Hoarding Disorder is typically slower and less complete than recovery from OCD. Patients and families should expect gradual improvement over months to years, not a dramatic transformation. The goal is a livable, safe home — not a perfectly organized one. Progress is real and meaningful even when it falls short of what others might consider "clean."
Treatment — Medications and Other Approaches
Serotonin Reuptake Inhibitors (SRIs)
Medications that target serotonin — including SSRIs like paroxetine and the serotonin-norepinephrine reuptake inhibitor (SNRI) venlafaxine — have been studied in Hoarding Disorder. The evidence shows modest benefit at best. These medications are far less effective in HD than they are in OCD, reflecting the different brain circuitry involved. They may help reduce anxiety around discarding, and they are useful for treating comorbid depression, but they should be understood as an adjunct to CBT — not a replacement for it.
Treating ADHD Comorbidity
When ADHD is present alongside Hoarding Disorder — which it is in roughly half of cases — treating the ADHD directly can meaningfully improve a person's capacity to engage in the hard work of decluttering. Atomoxetine (a non-stimulant ADHD medication) and stimulant medications like methylphenidate or amphetamine salts can improve decision-making, sustained attention, and the ability to follow through on sorting tasks. For someone whose hoarding is significantly driven by their inability to sustain attention long enough to make discard decisions, this intervention can be transformative.
Motivational Interviewing
Motivational Interviewing (MI) is a collaborative counseling style specifically designed to help people who are ambivalent about change. Because low insight and ambivalence are near-universal in Hoarding Disorder, MI is now considered standard pre-treatment and early-treatment practice for HD — not an optional extra. MI helps the person articulate their own reasons for change rather than being told by others that they have a problem.
Peer Support and Community Resources
Groups like Clutterers Anonymous offer regular meetings (including online) using a 12-step framework adapted for clutter and compulsive acquisition. Online communities provide mutual accountability and reduce the profound shame and isolation that hoarding generates. While peer support is not a substitute for professional treatment, it can be a powerful complement — and for many people without access to a specialized HD therapist, it may be the most accessible support available.
Harm Reduction: A Practical Middle Ground
For people who are not ready or able to engage in full CBT-HD, harm reduction is a legitimate and valuable goal. This means prioritizing safety and livability — clearing fire escape routes, addressing sanitation hazards, ensuring animals are fed and watered — even without achieving a full declutter. Harm reduction acknowledges that some improvement is better than no improvement, and that setting impossible goals leads to abandonment of any effort at all.
What Not to Do: The Coerced Cleanout
Perhaps the most important clinical caution in all of hoarding treatment: coerced cleanouts — having the home cleaned or emptied without the person's genuine consent — almost always fail. Research and clinical experience consistently show that within weeks to months, the home returns to the same level of clutter. More seriously, forced cleanouts carry real risks of psychological trauma and suicidality. The possessions are not just junk to the person with HD — they are part of their sense of self, memory, and security. Removing them by force causes genuine psychological devastation. Even when housing authorities or family members are involved, a collaborative, gradual approach is always preferable to a one-time forcible clearance.
Safety and Crisis Issues
Hoarding Disorder can create genuine emergencies that require immediate attention — not just clinical intervention. Understanding these safety dimensions is important for anyone living with a person who hoards, for family members, and for the person themselves.
Fire Risk
The most serious physical danger in a hoarding household is fire. Large quantities of paper, cardboard, and other combustible materials stacked throughout the home create ideal conditions for rapid fire spread. Blocked exits mean occupants cannot escape quickly. Overloaded electrical outlets hidden under clutter can overheat without being noticed. Fire departments in many cities have developed specialized protocols for responding to known hoarding households because the challenges they present are so different from a standard residential fire.
Fall Risk
Navigating narrow pathways through floor-to-ceiling clutter creates significant fall risk, particularly for older adults. A fall in a cluttered home may go unnoticed for hours or days. For elderly individuals with hoarding, this is a particularly dangerous combination — hoarding prevalence increases with age at the same time that fall consequences become more severe.
Sanitation and Infestation
Blocked plumbing, food waste hidden in piles, and the inability to clean surfaces create conditions for insect and rodent infestations. These are not merely unpleasant; they create genuine infectious disease risks and can compromise the structural integrity of the home through rodent damage to wiring and supports. Rotting organic material creates mold exposure risks. In severe cases, these conditions may trigger public health authority intervention.
Social Services and Legal Involvement
Hoarding Disorder frequently involves multiple agencies: Adult Protective Services (when an elderly person's safety is at risk), housing authorities (when a rental property is being damaged or other tenants are affected), animal control (when animal hoarding is present), and occasionally child protective services (when children are living in the home). Navigating these multiple agency relationships while supporting the person's mental health requires careful coordination and, ideally, a case manager who can bridge clinical and social service systems.
Suicidality During Forced Interventions
A critical safety concern that is often underappreciated: people with Hoarding Disorder can experience acute suicidal crises when facing forced loss of their possessions. When a court order, eviction, or family intervention results in the removal of their accumulated items, some individuals experience this as a profound identity loss equivalent to catastrophic bereavement. Any intervention involving coerced discarding must include mental health support and crisis planning, not just practical help with cleaning.
Children in Hoarding Households
Children growing up in severely cluttered homes face multiple risks: developmental impacts from the chaos and instability, social isolation (they cannot bring friends home), academic disruption, and in severe cases direct safety risks. Child Protective Services may become involved when living conditions fall below acceptable standards of safety. Children of hoarders often carry significant emotional burdens long into adulthood, including complex feelings of shame, anger, grief, and loyalty.
Living With Hoarding and Recovery
Recovery from Hoarding Disorder is genuinely possible, but it looks different from recovery from many other conditions. It typically involves gradual, sustained effort over months and years rather than a breakthrough moment. It requires ongoing support rather than a fixed treatment course. And it requires recalibrating expectations — both for the person with HD and for those around them.
Self-Compassion Is Essential
One of the most important reframes in hoarding recovery is understanding that hoarding is a brain-based disorder, not a character flaw. It does not reflect laziness, stupidity, or a failure of willpower. The person is not choosing to live this way out of perversity or disregard for others. The brain systems that govern decision-making, emotional regulation, and the perception of objects are working differently — and that is a medical reality, not a moral failing. Self-compassion, while difficult to build in the presence of deep shame, is a clinical necessity for sustained recovery.
For Family Members: How to Help Without Enabling
Family members of people with Hoarding Disorder face an agonizing dilemma. Watching someone they love live in dangerous, unhealthy conditions is deeply distressing. The impulse to just clean it up — to take a weekend and haul everything out — is understandable. But as discussed above, this approach backfires clinically and can damage the relationship irreparably.
More effective strategies for family members include:
- Validate their distress — acknowledge that discarding feels genuinely painful to them, even if you cannot personally understand why
- Maintain safety limits — it is appropriate to insist on clear exits, working smoke detectors, and basic sanitation, while accepting that the broader clutter may not resolve quickly
- Avoid cleaning for them — doing the sorting for the person without their active participation undermines their sense of agency and provides no lasting benefit
- Support treatment — encourage engagement with a therapist specialized in HD; offer to help locate resources; be patient with the pace of progress
- Take care of yourself — living with or being closely connected to someone with Hoarding Disorder is genuinely stressful; support groups and therapy for family members are legitimate and important
Graduated Goals and Celebrating Small Wins
A single drawer cleared. One pathway unblocked. A single grocery bag of discarded items. These feel small from the outside, but they represent real neurological and psychological work for the person with Hoarding Disorder. Celebrating these achievements — genuinely and without condescension — builds momentum and reinforces the belief that change is possible.
Resources
Several organizations provide information, therapist directories, and peer support specifically for hoarding:
- The International OCD Foundation (iocdf.org) maintains a therapist directory and extensive hoarding-specific resources
- Children of Hoarders (childrenofhoarders.com) provides support specifically for adult children navigating a parent's hoarding
- Clutterers Anonymous (clutterersanonymous.org) offers peer support meetings
Key Research Papers
- Frost RO, Hartl TL. (1996). A cognitive-behavioral model of compulsive hoarding. Behaviour Research and Therapy. PMID: 8871366. DOI: 10.1016/0005-7967(96)00010-3 — The foundational cognitive-behavioral model of hoarding; introduced the framework still used in clinical practice today.
- Mataix-Cols D, Frost RO, Pertusa A, et al. (2010). Hoarding disorder: a new diagnosis for DSM-V? Depression and Anxiety. PMID: 20336805. DOI: 10.1002/da.20693 — The consensus paper that made the case for HD as a distinct DSM-5 diagnosis separate from OCD.
- Frost RO, Steketee G, Grisham J. (2004). Measurement of compulsive hoarding: saving inventory-revised. Behaviour Research and TherapySearch PubMed. DOI: 10.1016/S0005-7967(03)00201-X — Validated the Saving Inventory-Revised (SI-R), the standard clinical measurement instrument for HD.
- Steketee G, Frost RO, Kyrios M. (2003). Cognitive aspects of compulsive hoarding. Cognitive Therapy and Research. DOI: 10.1023/A:1025428631552 — Detailed analysis of the cognitive beliefs (attachment, responsibility, memory) that maintain hoarding behavior.
- Tolin DF, Fitch KE, Frost RO, Steketee G. (2010). Family informants' perceptions of insight in compulsive hoarding. Cognitive Therapy and ResearchSearch PubMed. DOI: 10.1007/s10608-009-9261-0 — Documented the gap between patients' self-assessment of their hoarding and family members' perceptions; foundational for understanding low insight.
- Saxena S, Brody AL, Maidment KM, et al. (2004). Cerebral glucose metabolism in obsessive-compulsive hoarding. American Journal of PsychiatrySearch PubMed. DOI: 10.1176/appi.ajp.161.6.1038 — First neuroimaging study demonstrating that hoarding has distinct cerebral metabolic patterns separate from non-hoarding OCD.
- Pertusa A, Fullana MA, Singh S, Alonso P, Menchon JM, Mataix-Cols D. (2008). Compulsive hoarding: OCD symptom, distinct clinical syndrome, or both? American Journal of PsychiatrySearch PubMed. DOI: 10.1176/appi.ajp.2008.07081094 — Landmark comparative study demonstrating that most hoarding exists independently of OCD, supporting the separate diagnosis.
- Steketee G, Frost RO. (2007). Compulsive Hoarding and Acquiring: Therapist Guide. Oxford University Press. — The standard CBT-HD treatment protocol; the manual used by therapists treating hoarding worldwide.
- Tolin DF, Frost RO, Steketee G, Gray KD, Fitch KE. (2008). The economic and social burden of compulsive hoarding. Psychiatry ResearchSearch PubMed. DOI: 10.1016/j.psychres.2007.08.009 — Quantified the real-world costs of hoarding: financial burden, lost work productivity, social impairment, and housing instability.
- Frost RO, Tolin DF, Steketee G, Fitch KE, Selbo-Bruns A. (2009). Excessive acquisition in hoarding. Journal of Anxiety DisordersSearch PubMed. DOI: 10.1016/j.janxdis.2008.07.007 — Characterized the excessive acquisition component of HD, finding that ~70% of people with HD also engage in compulsive buying or collecting.
- Ayers CR, Saxena S, Golshan S, Wetherell JL. (2010). Age at onset and clinical features of late life compulsive hoarding. International Journal of Geriatric PsychiatrySearch PubMed. DOI: 10.1002/gps.2295 — Detailed the distinct presentation of hoarding in older adults, including higher prevalence and greater safety risks with age.
- Rachman S, Elliott CM, Shafran R, Radomsky AS. (2009). Separating hoarding from OCD. Behaviour Research and TherapySearch PubMed. DOI: 10.1016/j.brat.2009.03.006 — A theoretical and empirical analysis distinguishing the mechanisms, phenomenology, and treatment implications of hoarding versus OCD.
Search for more research: PubMed: Hoarding Disorder
Connections
- Psychiatry
- Obsessive-Compulsive Disorder
- Body Dysmorphic Disorder
- Trichotillomania
- ADHD
- Anxiety Disorders
- Depression
- Addiction