Dissociative Identity Disorder (DID)
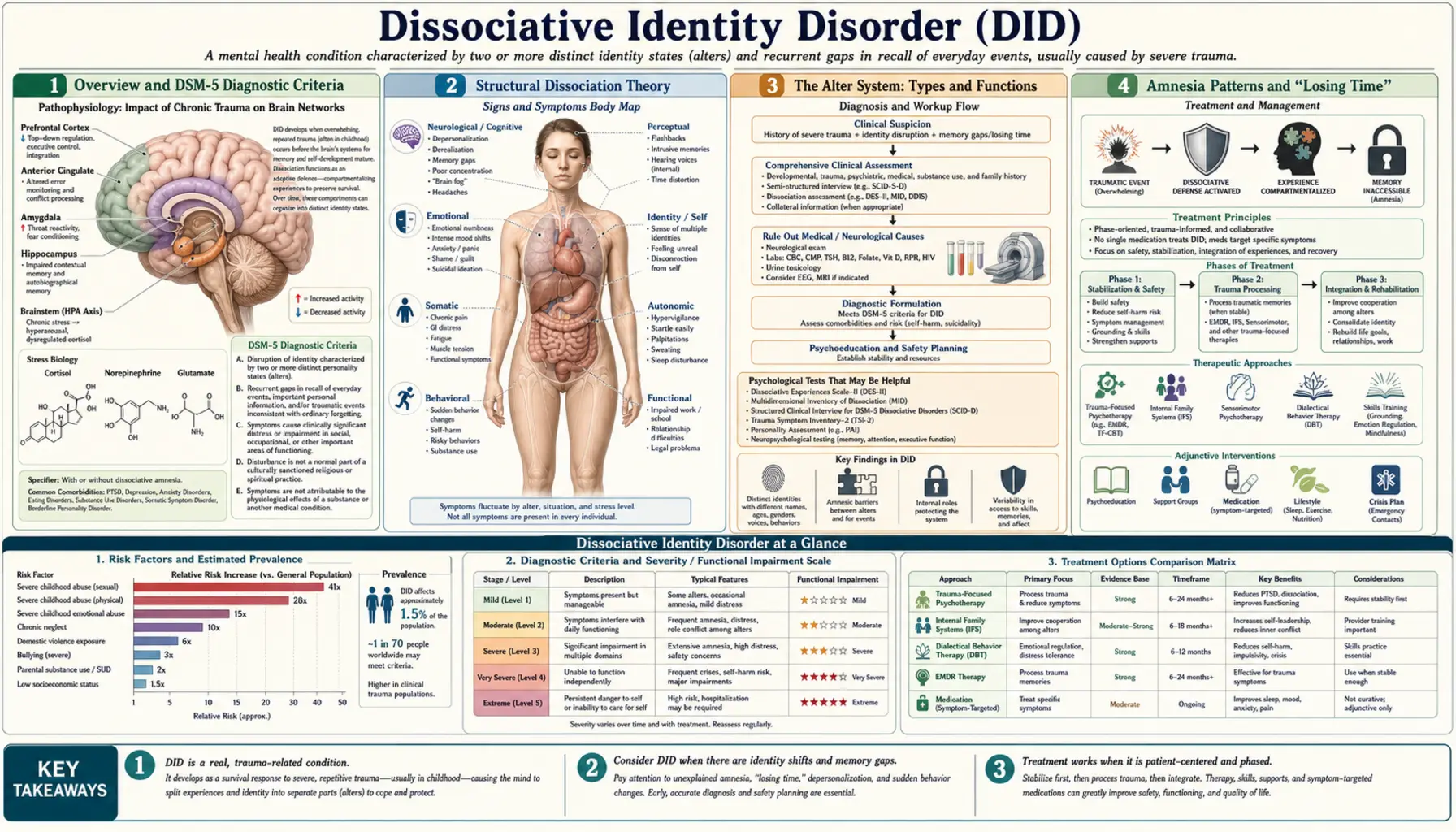
Dissociative Identity Disorder (DID), formerly called Multiple Personality Disorder (MPD) until the DSM-IV rename in 1994, is characterized by the presence of two or more distinct personality states — called "alters" — each with their own name, age, voice, mannerisms, memories, and behavioral repertoire. DID is not rare: prevalence estimates reach 1–1.5% of the general population. It is profoundly underdiagnosed, with patients averaging 6–7 years in the mental health system before a correct diagnosis is established. The overwhelming majority (approximately 90%) report severe, repeated childhood trauma — most often sexual or physical abuse — as the formative experience underlying the disorder.
- Overview and DSM-5 Diagnostic Criteria
- Structural Dissociation Theory
- The Alter System: Types and Functions
- Amnesia Patterns and "Losing Time"
- Voices and Hallucinations: DID vs. Psychosis
- Comorbidities: PTSD, Depression, and Suicide Risk
- Neurobiological Evidence
- Diagnosis: Tools and Differential Diagnosis
- Phase-Based Trauma Therapy (ISSTD Guidelines)
- Pharmacotherapy
- Controversy: Trauma Model vs. Iatrogenic Model
- Key Research Papers
Overview and DSM-5 Diagnostic Criteria
Dissociative Identity Disorder is defined in DSM-5 by five core criteria that must all be present. Criterion A requires two or more distinct personality states — characterized by marked discontinuity in sense of self, sense of agency, cognition, behavior, affect, perception, consciousness, memory, and/or sensory-motor functioning. Criterion B requires recurrent gaps in the recall of everyday events, important personal information, and/or traumatic events that are inconsistent with ordinary forgetting. Criterion C specifies that the symptoms are not the result of a substance (such as alcohol blackouts) or another medical condition (such as complex partial seizures or temporal lobe epilepsy). Criterion D requires that in children, the symptoms are not better explained by imaginary playmates or other fantasy play. Criterion E states that the symptoms cause clinically significant distress or impairment in functioning.
The rename from Multiple Personality Disorder (MPD) to Dissociative Identity Disorder in DSM-IV (1994) was deliberate and meaningful. The older name invited misunderstanding: the word "multiple" suggested discrete, separate personalities living inside one body — the Hollywood framing dramatized by films like The Three Faces of Eve (1957) and Sybil (1976). The new name emphasizes what actually breaks down: identity — the normally integrated sense of "I am one continuous person with a single perspective across time." DID is not a disorder of having too many personalities; it is a disorder of failure to integrate experience, memory, and self-concept into a coherent whole.
Epidemiologically, DID is more common than is widely appreciated. Population-based studies find prevalence of approximately 1.0–1.5%, comparable to schizophrenia. Clinical samples show a female-to-male ratio of approximately 5:1, though this likely reflects help-seeking bias: men with dissociative disorders are more often diagnosed with antisocial personality disorder, substance use disorder, or conduct disorder, and present to forensic rather than clinical settings. The average patient spends 6–7 years in the mental health system receiving incorrect diagnoses — most commonly depression, bipolar disorder, or schizophrenia — before DID is identified.
Approximately 90% of DID patients report a history of severe, repeated childhood trauma, most commonly sexual abuse, physical abuse, emotional abuse, or severe neglect beginning before age 9. The developmental period before age 9 is believed to be critical because the capacity for normal identity integration has not yet consolidated; trauma during this period disrupts the developmental process of integrating different ego states into a unified self. This is why DID is considered a developmental trauma disorder, not merely an adult-onset stress response.
- Prevalence: 1.0–1.5% general population (comparable to schizophrenia in frequency)
- Mean time to correct diagnosis: 6–7 years
- Gender ratio (clinical): approximately 5:1 female-to-male
- Trauma history: approximately 90% report severe childhood abuse or neglect
- DSM-5 criteria: A (distinct identity states) + B (amnesia) + C (not substance/medical) + D (not childhood fantasy) + E (functional impairment)
- Most common incorrect diagnoses: bipolar disorder, depression, schizophrenia, borderline personality disorder
Structural Dissociation Theory
The most influential theoretical framework for understanding DID is the Theory of Structural Dissociation of the Personality, developed by Onno van der Hart, Ellert Nijenhuis, and Kathy Steele, most fully articulated in their 2006 book The Haunted Self. The theory draws on Pierre Janet's 19th-century work on dissociation and adapts it to contemporary neuroscience. Its central claim is that dissociation is not merely a disorder of memory — it is a disorder of the entire personality system, where the biological underpinnings of personality fail to integrate under conditions of overwhelming stress.
The theory proposes that the personality divides into two primary structural components. The Apparently Normal Part (ANP) is the part of the personality responsible for managing daily life — going to work, socializing, caring for children, maintaining routines. The ANP is oriented toward present-day reality and toward action systems that promote daily functioning: attachment, caregiving, play, energy management, reproduction. Critically, the ANP is phobic of traumatic memories; it avoids trauma cues and remains amnesic for the traumatic past. When the ANP is present, the person may appear entirely functional and show no obvious signs of psychiatric disorder. The Emotional Part (EP), by contrast, is the structural component that holds traumatic memories. The EP is fixated on the trauma; it responds to trauma cues with hyperarousal, intrusion, flashbacks, and somatic re-experiencing. The EP is oriented toward survival action systems — flight, fight, freeze, collapse, submission — that were adaptive during the original trauma but are maladaptive in current daily life.
In simple dissociative disorders (such as PTSD), there is one ANP and one EP. In complex DID, the personality has fragmented further: multiple EPs exist, each holding different traumatic experiences, different developmental periods, or different aspects of the trauma response. Multiple ANPs may also exist, each managing different domains of daily functioning (one for work, one for parenting, one for intimate relationships). This layered structural fragmentation explains the clinical complexity of DID: why some alters know about others but not vice versa (asymmetric amnesia between structural layers), why different alters have dramatically different behavioral patterns and emotional responses, and why the system can appear highly organized in some cases and chaotic in others.
A key insight of the structural dissociation model is that ANP and EP states show genuinely different psychobiological response patterns to identical stimuli. When exposed to trauma-related cues, the ANP demonstrates phobic avoidance — physiological underactivation, narrowed attention, emotional numbing. The EP demonstrates approach and re-experiencing — physiological hyperactivation, intrusive memory, somatic sensation, affective flooding. These are not performed or pretended differences; they are measurable differences in autonomic nervous system activation, cortisol response, and neural activity patterns. The theory therefore predicts that alter states should show genuinely different physiological signatures — a prediction confirmed by neuroimaging research (see Neurobiology section).
- ANP (Apparently Normal Part): manages daily life; phobic of trauma; amnesic for traumatic past; oriented toward present reality
- EP (Emotional Part): holds traumatic memories; responds to trauma cues with intrusion and hyperarousal; fixed in survival mode
- Simple dissociation: 1 ANP + 1 EP (basic PTSD structure)
- Complex DID: multiple EPs + possibly multiple ANPs, each compartmentalizing different experiences
- Key prediction: different alter states show genuinely different psychobiological responses — confirmed by PET/fMRI and autonomic research
The Alter System: Types and Functions
The collection of all alter states in a DID system is called the "system." Systems vary enormously: some patients have 2–3 alters; others have 25, 50, or even reported systems of over 100. The average falls somewhere between 5 and 25. Each alter may have a distinct name, age, gender, handwriting style, clothing preferences, speech patterns, emotional tone, and memory set. Some alters are aware of each other; others have no knowledge that other alters exist. The internal organization of the system ranges from highly structured and cooperative to chaotic and conflicted.
Common alter types that clinicians encounter include the host, who is the alter present most frequently in day-to-day life and typically presents first to therapy. The host is often the least aware that the system exists and may have the most amnesia for the internal landscape. Child alters are extremely common — they are alters age-frozen at the developmental period of a specific trauma, behaving, speaking, and experiencing the world as that age. A child alter of age 4 may not know the host is an adult, may believe it is still the year the trauma occurred, and may be terrified by adult environments. Protector alters emerge to defend the system against perceived threats, internal or external. They are often experienced as angry, intimidating, or aggressive, and may present with male identity even in female-assigned systems; they serve a genuine adaptive function of keeping others safe. Persecutor alters are among the most clinically challenging: they are internally hostile, may threaten or harm other alters, and are often the mechanism through which self-harm occurs. They frequently represent an internalized version of the abuser — having taken on the abuser's voice, attitudes, and threatening behaviors as a way of anticipating and managing external threat.
Trauma holder alters exist specifically to compartmentalize particular traumatic memories, allowing other parts of the system to function without being overwhelmed by those memories. Caretaker or helper alters may emerge to tend to distressed child alters internally or to manage practical tasks externally. Opposite-gender alters are common and serve various functions — sometimes embodying aspects of identity the host is not permitted to express, sometimes modeling the gender of an abuser as a way of understanding the trauma. In rare cases, systems include non-human alters — animals, mythological figures, supernatural beings — which represent the most extreme forms of identity compartmentalization and often hold particularly overwhelming material.
Switching — the transition from one alter state to another — is a core feature of DID and can range from nearly invisible to highly dramatic. Triggers for switching include stress, trauma-related cues (smells, sounds, visual stimuli that resemble traumatic contexts), anniversaries, interpersonal conflict, or deliberate internal negotiation. A subtle switch may involve only a slight change in posture, voice tone, or eye contact. A dramatic switch may involve a period of blank staring, confusion about location or date, a complete change of behavioral style, or frank amnesia. Some systems develop varying degrees of co-consciousness — the capacity for two or more alters to be simultaneously aware and even to communicate internally in real time. Co-consciousness is often a therapeutic goal, as it reduces amnesia barriers and enables more cooperative system functioning.
- Host: most frequently presenting alter; often least aware of DID; default daily-function state
- Child alters: age-frozen at time of specific trauma; may not know current year or that host is adult
- Protector alters: defensive/aggressive; may present as male in female-assigned systems; externally or internally directed protection
- Persecutor alters: internally hostile; often internalized abuser voice; mechanism of self-harm; requires careful therapeutic engagement (not elimination)
- Trauma holder alters: compartmentalize specific traumatic memories to allow system functioning
- Caretaker/helper alters: tend to distressed parts; manage internal or external tasks
- Non-human alters: rare; represent extreme compartmentalization; often hold overwhelming material
- Switching triggers: stress, trauma cues, anniversaries, conflict, sensory reminders of trauma
- System size: typically 5–25 alters; range from 2 to over 100
Amnesia Patterns and "Losing Time"
Amnesia is the second defining criterion of DID (DSM-5 Criterion B) and is perhaps its most diagnostically distinctive feature. Unlike ordinary forgetting, the amnesia of DID is structural — it reflects genuine barriers between alter states in which one state genuinely lacks access to memories stored by another state. This is not suppression or motivated forgetting in the ordinary sense; it is a failure of the normal encoding and retrieval processes that integrate experience into a continuous autobiographical narrative. The clinician's key task is to understand which types of amnesia are present and how extensive they are.
Unilateral amnesia is among the most common patterns: the host alter is amnesic for what an alter has done, but that alter retains awareness of the host's experiences. The alter "watches" the host from inside but the host does not remember periods when the alter was present. Bilateral amnesia is more severe: neither alter state has access to the other's experiences. Co-consciousness, by contrast, represents the absence of amnesia barriers — both states are simultaneously aware and both retain memory of a shared period. In most DID systems, different pairs of alters have different amnesia arrangements; the internal memory architecture is not uniform across the system.
The clinical manifestations of DID-related amnesia that patients commonly report include: finding themselves in an unfamiliar location with no memory of having traveled there (a dissociative fugue state); discovering clothing, food, or purchased items they have no memory of selecting or buying; being told by family members or friends about behavior or conversations they have no recollection of; finding journals, artwork, or notes in a handwriting style different from their own; waking up to find tasks completed that they have no memory of starting; and being called by a name they do not recognize. These experiences are profoundly disorienting and frequently described as terrifying — patients may feel they are "going crazy," which contributes to the common years-long delay in seeking or receiving appropriate help.
Depersonalization and derealization are closely associated with the amnesia of DID and often accompany switching. Depersonalization is the experience of being detached from one's own mental processes or body — feeling like an outside observer of one's thoughts, feelings, sensations, and actions. Derealization is the experience that the external world feels unreal, dreamlike, distant, or distorted. Both are ego-dystonic in DID — that is, the patient recognizes that something is wrong and finds the experience disturbing, rather than accepting the unreality as normal. This ego-dystonic quality is an important differentiator from certain psychotic experiences, in which the patient may not recognize that their perceptions are abnormal. Patients with DID frequently describe their experience of switching as "watching a movie of my life" or "watching myself from the corner of the room" — classic depersonalization language.
- Unilateral amnesia: host amnesic for alter actions; alter aware of host — most common pattern
- Bilateral amnesia: neither alter aware of the other — most severe pattern
- Co-consciousness: simultaneous mutual awareness — often a therapeutic goal
- Common experiences: finding oneself in unknown locations; unknown purchases; unfamiliar handwriting; gaps in the day
- Depersonalization/derealization: ego-dystonic unreality; "watching myself"; often accompanies switching
- Key differential point: depersonalization is distressing and recognized as abnormal (ego-dystonic) — distinct from psychotic unreality
Voices and Hallucinations: DID vs. Psychosis
Auditory hallucinations — hearing voices — occur in approximately 80% of patients with DID and represent one of the most common reasons DID is misdiagnosed as schizophrenia. The distinction between DID-related and psychosis-related voices is clinically critical because the treatments are fundamentally different: antipsychotic medication for schizophrenia-spectrum voices, trauma therapy and alter engagement for DID-related voices. Treating DID voices primarily with antipsychotics misses the diagnosis, may impair the therapeutic engagement needed for recovery, and does not address the underlying dissociative architecture.
The most important distinguishing question a clinician can ask is: "When you hear the voice, does it seem to come from inside your head — like a thought that has a voice quality — or does it seem to come from outside, like a real person speaking in the room?" In DID, the overwhelming majority of voices (approximately 80%) are internal — they are experienced as coming from inside the head. They represent alters communicating, commenting, arguing, or issuing instructions from within the system. In schizophrenia-spectrum illness, hallucinations are more typically external — heard as coming from outside the head, often attributed to real people, machines, or supernatural sources, and experienced as unambiguously real external perceptions rather than internal mental events.
Beyond location, DID voices have characteristic features that differ from psychotic hallucinations. DID voices have distinct character — they feel like specific personalities with names, ages, attitudes, and histories. They may argue with each other or with the host. They may offer helpful guidance (protector alters) or threatening commentary (persecutor alters). Critical hostile voices are a common presentation of the persecutor alter pattern — the internalized abuser voice commenting harshly on the host's actions or worth. This is distinct from the command hallucinations of psychosis, which tend to be more alien, unfamiliar, and experienced as external impositions rather than as internal personages the patient has a relationship with. Patients with DID can often describe these voices in rich detail and can frequently engage with them cooperatively — a form of internal communication that becomes a cornerstone of DID therapy (internal self-leadership work, meeting and negotiating with alters internally). This capacity for cooperative engagement with voices would be highly atypical in schizophrenia.
Additional features that distinguish DID from schizophrenia: DID patients do not typically show formal thought disorder (loosening of associations, tangentiality, word salad, neologisms), which is a hallmark of schizophrenia. DID patients do not show the negative symptoms of schizophrenia (flat affect, poverty of speech, social withdrawal, avolition, anhedonia). DID patients typically maintain emotional relatedness and are able to form therapeutic alliances, which is often challenging in active schizophrenia. DID has a different onset trajectory — trauma in early childhood, with symptoms present from early life, rather than the adolescent/early adult new-onset pattern typical of schizophrenia. When these distinguishing features are systematically assessed, the diagnostic confusion should resolve, though in practice it frequently does not without specific training in dissociative disorders.
- Critical question: "Inside or outside your head?" — DID voices approximately 80% internal; psychotic hallucinations typically external
- DID voice character: distinct named personalities; argue with each other; feel like internal relationships rather than alien impositions
- Persecutor alter voices: critical, hostile commentary — often internalized abuser; distinct from command hallucinations
- Cooperative engagement: DID patients can negotiate with voices; unusual in schizophrenia
- No formal thought disorder: DID speech is coherent; loosening of associations absent
- No negative symptoms: DID maintains affect, relatedness, speech, motivation — schizophrenia often does not
- Onset trajectory: DID = childhood trauma onset; schizophrenia = adolescent/early adult new onset
Comorbidities: PTSD, Depression, and Suicide Risk
DID is rarely a standalone diagnosis. Because it arises from severe and repeated childhood trauma, it carries an enormous comorbidity burden. PTSD is present in over 80% of DID patients, and in many the PTSD is complex (C-PTSD) — characterized not only by the classic triad of re-experiencing, avoidance, and hyperarousal, but by additional features of pervasive emotional dysregulation, profoundly negative self-concept, chronic shame and guilt, severe interpersonal difficulties, and somatization. The distinction between PTSD, C-PTSD, and DID exists on a continuum of severity of structural dissociation; DID represents the most severe end of this continuum.
Major depressive disorder is present in over 90% of clinical DID samples. The depression in DID is often treatment-resistant to standard antidepressant monotherapy because its roots are in unprocessed trauma and ongoing internal system conflict rather than in the biological dysregulation that antidepressants primarily target. Substance use disorders are common as a form of self-medication: patients use alcohol, cannabis, opioids, or other substances to manage the distress of intrusive symptoms, internal conflict, and emotional overwhelm. A particularly complex clinical feature is that individual alters may have different relationships to substances — one alter may use substances heavily while another is abstinent — which complicates standard addiction treatment approaches. Eating disorders affect a significant subset of DID patients, often reflecting themes of control, bodily shame, self-punishment, and the complex relationship with the body that trauma creates.
Borderline Personality Disorder (BPD) co-occurs with DID in approximately 30–50% of clinical samples, and distinguishing the two is one of the most important and challenging differential diagnosis tasks in trauma psychiatry. Both involve identity disturbance, emotional dysregulation, self-harm, and attachment difficulties. The key distinctions are: BPD features identity diffusion — an unstable, shifting sense of self without discrete, distinct alter states with separate names and histories. BPD does not have the amnesia barriers characteristic of DID. Rapid mood shifts in BPD are related to interpersonal context and relational triggers, not to switching of discrete identity states. However, the two can genuinely co-occur, and some DID patients carry BPD as an additional valid diagnosis.
Self-harm and suicidality are among the most clinically urgent comorbidities. Approximately 70–80% of DID patients have a history of self-harm, most commonly self-cutting. Self-harm in DID is frequently not a simple mood-regulation strategy: it is often carried out by a persecutor alter targeting the host body — the persecutor may cut in order to punish the host, to communicate distress, or to exercise control over the shared body. This systemic dimension of self-harm in DID means that standard self-harm interventions must be adapted to engage the entire system and specifically to understand and ultimately transform the persecutor alter's function and motivations, rather than simply contracting the host not to self-harm. Lifetime suicide attempt rates in DID are among the highest of any psychiatric diagnosis — estimated at 70–80%. Individual alters may hold suicidality: the system may contain a suicidal alter while the host presents as not currently suicidal. Thorough suicide risk assessment in DID must therefore assess the suicidality of all known parts of the system, not only the presenting state.
- PTSD: over 80% comorbidity; often complex PTSD with emotional dysregulation, shame, and somatization
- Major depression: over 90% in clinical samples; often treatment-resistant without trauma processing
- Substance use: self-medication of intrusive symptoms; individual alters may have different substance use patterns
- Eating disorders: control, bodily shame, self-punishment themes
- BPD: co-occurs in 30–50%; key difference is absence of discrete named alter states and amnesia barriers in pure BPD
- Self-harm: 70–80% history; often persecutor alter targeting host body; requires system-wide engagement
- Suicide: 70–80% lifetime attempt rate; assess all alters for suicidality, not only the presenting state
- Somatic symptoms: headaches during switching; psychogenic non-epileptic seizures (PNES); fibromyalgia-pattern pain
Neurobiological Evidence
One of the most important scientific contributions to understanding DID came from a landmark positron emission tomography (PET) study by Antje Reinders and colleagues, published in Biological Psychiatry in 2003. The study measured regional cerebral blood flow (rCBF) — a proxy for neural activity — in DID patients while different alter states were active. Researchers used a trauma script procedure: participants listened to a personalized script describing traumatic events, and their brain activity was measured separately when the neutral identity state (NIS — corresponding to the ANP or host) was active and when the traumatic identity state (TIS — corresponding to trauma-holder alters or EPs) was active.
The results were striking. The NIS and TIS showed significantly different patterns of rCBF in the same individual across the same stimulus — including differences in medial prefrontal cortex activity, parietal cortex activation, and anterior cingulate response. These differences were consistent with the theoretical prediction that ANP and EP states have genuinely different psychobiological response patterns. Critically, the researchers also tested a control group of healthy non-DID participants asked to simulate or role-play these different identity states — pretending to be a trauma-holding state vs. a neutral daily-function state. The simulators showed the same brain pattern in both conditions. They could not produce the neural differentiation that the DID patients showed spontaneously. This is powerful neurobiological evidence that the identity state differences in DID are genuine rather than performance-based.
Subsequent research has extended these findings. Different alters show different cortisol responses to identical stressors — a finding that should be impossible if the differences between alter states were purely behavioral or performative, since cortisol release is controlled by the hypothalamic-pituitary-adrenal (HPA) axis and is not under voluntary control. Documented differences in pain threshold between alter states have been measured in some patients, with some alters showing markedly different pain sensitivity than others. Perhaps most strikingly, there are case reports — and some optometric case studies — of genuinely different visual acuity measured between alter states in the same individual, confirmed by repeated standardized refraction testing. These findings suggest that the psychobiological divergence between alter states may extend to peripheral sensory systems, not only central neural processing.
Neuroimaging has also identified consistent patterns of structural and functional brain differences in DID patients compared to trauma-exposed controls without DID and to healthy controls. Reduced volume and altered connectivity of the hippocampus and amygdala — structures critical for memory encoding and threat processing — are found in DID, consistent with the known effects of early chronic trauma on these structures. Altered prefrontal-limbic connectivity suggests impaired top-down regulation of emotional and survival responses. These findings parallel the neurobiological changes seen in PTSD but are typically more severe, consistent with the greater severity of structural dissociation in DID compared to PTSD without dissociation.
- Reinders 2003 PET study: different alter states show genuinely different regional cerebral blood flow patterns in the same individual
- Critical control finding: non-DID simulators cannot reproduce the neural differentiation — it is not performance
- Cortisol: different alters show different HPA axis responses to identical stressors — not under voluntary control
- Pain threshold: documented differences between alter states in some patients
- Visual acuity: case reports of different refraction measurements between alter states
- Hippocampus and amygdala: reduced volume consistent with severe early chronic trauma
- Prefrontal-limbic connectivity: impaired top-down regulation of emotion and threat response
Diagnosis: Tools and Differential Diagnosis
Diagnosing DID requires specific knowledge of dissociative symptoms and the use of validated structured assessment tools. Standard psychiatric interviews not specifically designed for dissociative disorders frequently miss DID. The most common reason is that patients with DID are often ashamed of their symptoms, have been disbelieved in the past, have been told their experiences are "just anxiety" or "just trauma," or are themselves uncertain whether their internal experiences are real. They may not volunteer information about amnesia gaps, internal voices, or switching episodes without being specifically and sensitively asked.
The Structured Clinical Interview for DSM Dissociative Disorders (SCID-D), developed by Marlene Steinberg, is the gold standard structured clinical interview for dissociative disorders. It assesses five core symptom domains: amnesia, depersonalization, derealization, identity confusion, and identity alteration. Its semi-structured format allows skilled interviewers to follow up on positive symptom reports with detailed phenomenological questions, capturing the quality and frequency of experiences rather than just their presence or absence. The SCID-D produces severity ratings for each domain and yields DSM-5 diagnoses for all dissociative disorders.
The Multidimensional Inventory of Dissociation (MID), developed by Paul Dell, is a comprehensive self-report measure of 218 items assessing 23 facets of pathological dissociation. It is among the most thoroughly validated instruments for DID diagnosis and captures the full range of dissociative phenomena including amnesia, identity alteration, and depersonalization/derealization. The Dissociative Experiences Scale (DES-II) is a widely used 28-item screening questionnaire; a score above 30 is highly predictive of a dissociative disorder and should prompt more detailed structured evaluation. The DES-II is appropriate as an initial screen but not sufficient for diagnosis.
Differential diagnosis requires careful consideration of several conditions. Bipolar disorder can mimic DID in some respects: both involve shifts in mood, energy, behavior, and self-experience. Key differences are that bipolar episodes have gradual onset and offset over days to weeks, not the rapid switching of seconds to minutes characteristic of DID; bipolar patients do not have distinct alter states with separate names and histories; and bipolar does not feature the amnesia barriers of DID. Schizophrenia is frequently confused with DID due to shared auditory hallucinations, but the differences in voice character (internal vs. external), absence of formal thought disorder and negative symptoms in DID, and different developmental trajectory allow differentiation. Temporal lobe epilepsy (TLE) must be ruled out, particularly in patients with dramatic behavioral shifts, derealization, or brief amnesic episodes; EEG is appropriate when this is clinically suspected. Malingering is a frequent concern raised by skeptical clinicians, but is rare in practice: there is generally no material gain from a DID diagnosis; patients typically conceal rather than advertise symptoms; genuine amnesia barriers can be assessed with standardized memory paradigms; and longitudinal assessment almost always reveals the genuine functional impairment of the disorder.
- SCID-D (Steinberg): gold standard structured interview; assesses 5 domains; produces DSM-5 dissociative disorder diagnoses
- MID (Dell): 218-item self-report; 23 facets of dissociation; well-validated for DID
- DES-II: 28-item screen; score over 30 highly predictive; appropriate as initial screen only
- vs. Bipolar: bipolar episodes gradual (days–weeks) not rapid (seconds–minutes); no named alters; no amnesia barriers
- vs. BPD: BPD lacks distinct named alter states and amnesia barriers; can co-occur with DID
- vs. Schizophrenia: voice location (internal vs. external); no formal thought disorder; no negative symptoms; different onset
- vs. TLE: rule out with EEG when clinically suspected
- vs. Malingering: rare; no material gain; patients conceal symptoms; genuine amnesia testable longitudinally
Phase-Based Trauma Therapy (ISSTD Guidelines)
The International Society for the Study of Trauma and Dissociation (ISSTD) published comprehensive treatment guidelines for DID in adults in 2011 (third revision), representing the clinical consensus of an international body of trauma specialists. The core of the recommended treatment is a three-phase model, adapted from Judith Herman's phases of trauma recovery. This phased approach is not a rigid sequence that every patient marches through in order; many patients cycle between phases, and Phase 1 work continues throughout treatment. The central principle is that trauma processing (Phase 2) must not be attempted until Phase 1 stability is sufficiently consolidated — premature trauma processing causes traumatic decompensation, worsening dissociation, and increased risk of hospitalization and self-harm.
Phase 1: Safety, Stabilization, and Skill-Building. This phase may last months to years and is the foundation on which all subsequent work rests. The goals of Phase 1 are: establishing external safety (ending ongoing abuse, securing housing, addressing suicidality to a workable level); providing psychoeducation about DID and dissociation (many patients find it enormously relieving to have a name and explanation for their experiences); building a therapeutic alliance that explicitly includes all parts of the system — the therapist must be willing to communicate with and respect all alters, not only the host; developing distress tolerance skills drawn from Dialectical Behavior Therapy (DBT), including TIPP (Temperature, Intense exercise, Paced breathing, Progressive relaxation), ACCEPTS (Activities, Contributing, Comparisons, Emotions, Pushing away, Thoughts, Sensations), and IMPROVE (Imagery, Meaning, Prayer, Relaxing actions, One thing in the moment, Vacation, Encouragement); developing personalized grounding techniques for dissociative episodes; establishing sleep regularity and daily structure; and beginning to establish internal communication between alters — reducing amnesia barriers and building a system in which alters can cooperate, share information, and coordinate behavior. Internal communication work is central to Phase 1 and is often accomplished through techniques like internal meeting spaces, journaling across alter states, and specific internal communication exercises.
Phase 2: Trauma Processing. Only when Phase 1 is sufficiently consolidated does trauma processing begin. The most evidence-supported approaches for DID include EMDR (Eye Movement Desensitization and Reprocessing) adapted specifically for dissociative disorders. Standard EMDR protocols must be modified for DID: processing must include alters who hold the traumatic material, not only the host; dual awareness must be carefully maintained throughout processing to prevent uncontrolled abreaction; and the therapist must be prepared to pause and stabilize if any part of the system becomes overwhelmed. EMDR for DID requires specific training beyond standard EMDR certification. Somatic Experiencing (Peter Levine) and other body-based trauma processing approaches are particularly useful for alters holding somatic trauma memories and for working with the body-level freeze and collapse responses encoded in trauma. The principle of maintaining the "window of tolerance" (Ogden) — keeping the patient within the range of arousal that is neither so low as to be dissociative nor so high as to be overwhelmed — guides all Phase 2 work. Trauma memories are processed with awareness of the full system: who holds what material, which alters may be affected by processing, and how to care for the system before and after sessions.
Phase 3: Integration and Rehabilitation. Integration does not necessarily mean that all alters merge into a single unified personality, and this is an important correction of a common misconception. Many DID patients achieve what is called functional integration — a state in which alters communicate freely, cooperate consistently, share memories, experience co-consciousness, and work harmoniously toward common life goals, without necessarily losing their distinct identities. Some patients do experience fusion — the spontaneous or deliberate merging of two or more alters into a unified state — and may achieve complete fusion of the system. Both outcomes are valid and should follow the patient's own process rather than a therapist-imposed goal of eliminating all alter distinctiveness. Phase 3 also involves future-oriented life-building: addressing developmental gaps (child alters may experientially need to "grow up" in the context of therapy), building adult life skills that have been impaired by years of dissociation, rebuilding relationships, pursuing education and employment, and constructing a meaningful life beyond the preoccupation with trauma management.
- ISSTD 2011 Guidelines: phase-based treatment; premature trauma processing causes decompensation — do not skip Phase 1
- Phase 1 goals: external safety; psychoeducation; therapeutic alliance with all alters; distress tolerance skills; internal communication between alters
- Phase 2 modalities: EMDR (adapted for DID, requires specific training); Somatic Experiencing; titrated trauma processing; maintain window of tolerance
- Phase 3 outcomes: functional integration (cooperative system) OR fusion (alters merge) — both valid; follow patient's process
- Key principle: treat the whole system, not only the host; all alters deserve therapeutic respect and engagement
- Duration: effective DID therapy typically takes many years; not a brief intervention
Pharmacotherapy
There is no FDA-approved medication for DID itself, and no pharmacological agent has been shown to directly reduce or eliminate dissociation or alter switching in controlled clinical trials. Pharmacotherapy in DID is therefore targeted at comorbid conditions — particularly the PTSD, depression, emotional dysregulation, and sleep disturbance that accompany the disorder — with the goal of reducing overall symptom burden so that trauma-focused psychotherapy can proceed more effectively.
For the PTSD and depression that affect the vast majority of DID patients, selective serotonin reuptake inhibitors (SSRIs) — particularly fluoxetine (Prozac) and sertraline (Zoloft) — and serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine (Effexor) and duloxetine (Cymbalta) are appropriate first-line agents. These medications have the strongest evidence base for PTSD and depression, may reduce hyperarousal and intrusive symptoms, and may modestly improve emotional stability — supporting the capacity to engage in psychotherapy. Prazosin, an alpha-1 adrenergic blocker, has evidence for reducing trauma-related nightmares in PTSD and may be particularly useful in DID patients troubled by nighttime intrusions. Mood stabilizers — particularly lamotrigine (Lamictal) and valproate (Depakote) — may help with emotional dysregulation, impulsivity, and rapid mood cycles, and lamotrigine has also shown some benefit in depersonalization disorder, making it potentially worth considering in DID with prominent depersonalization.
Low-dose atypical antipsychotics — such as quetiapine (Seroquel) at low doses or risperidone at low doses — may be used adjunctively for sleep disturbance, severe dissociation, or trauma-related pseudo-psychotic symptoms. They are not appropriate as primary treatment for the auditory hallucinations of DID, because doing so misattributes those hallucinations to psychosis rather than to dissociative alter-state communication. High-dose antipsychotic treatment for DID voices is strongly contraindicated: it pursues the wrong diagnosis, does not target dissociation, may impair the cognitive and emotional engagement necessary for psychotherapy, and may partially suppress symptoms without addressing the underlying structural dissociation.
Benzodiazepines are generally contraindicated or should be used with extreme caution in DID. The reasons are multiple and clinically important: benzodiazepines paradoxically increase dissociation in many patients rather than reducing it; they cause anterograde amnesia, which worsens the already-present amnesia between alter states; they carry significant dependence risk; individual alters may have different relationships to the medication (one alter may take the prescribed dose, another may take an additional dose without the first alter being aware); and some alter states may misuse benzodiazepines in ways the host alter is completely unaware of. When anxiety management is needed, non-benzodiazepine approaches (SSRIs, hydroxyzine, propranolol as-needed for physiological anxiety symptoms, DBT distress tolerance skills) are strongly preferred. Emerging research on MDMA-assisted psychotherapy and ketamine represents interesting experimental frontiers, but neither is yet standard of care for DID and both require careful infrastructure and specifically trained clinicians.
- No FDA-approved medication for DID itself: pharmacotherapy targets comorbidities
- SSRIs/SNRIs: first-line for comorbid PTSD and depression; reduce hyperarousal and intrusion
- Prazosin: evidence-based for trauma nightmares
- Mood stabilizers: lamotrigine or valproate for emotional dysregulation; lamotrigine also has depersonalization evidence
- Low-dose atypical antipsychotics: adjunctive for sleep or pseudo-psychotic symptoms; not primary treatment for voices
- High-dose antipsychotics for DID voices: contraindicated — wrong diagnosis, impairs therapy engagement
- Benzodiazepines: generally contraindicated — worsen dissociation, cause anterograde amnesia, dependence risk, inter-alter misuse
Controversy: Trauma Model vs. Iatrogenic Model
DID has been among the most contested diagnoses in modern psychiatry. The debate centers on a fundamental question: is DID a genuine disorder arising from severe childhood trauma, or is it a socially constructed clinical artifact created by therapist suggestion, cultural scripts, and media influence? The two major positions are the trauma model (endorsed by the ISSTD and the majority of dissociation researchers) and the sociocognitive or iatrogenic model (associated primarily with Nicholas Spanos and later with Harald Merckelbach and colleagues).
The trauma model holds that DID results from severe, repeated childhood trauma — particularly abuse beginning before age 9, during the developmental window in which normal personality integration is still occurring. Trauma creates genuine structural dissociation: the child's developing identity system fragments under overwhelming stress, creating compartmentalized identity states that manage different traumatic experiences and different functional demands. The model is supported by the overwhelming prevalence of severe trauma histories in DID samples (approximately 90%); the cross-cultural occurrence of DID in countries without significant media exposure to the MPD concept (documented in the Netherlands, Turkey, China, Japan); the neurobiological evidence demonstrating genuine psychobiological differences between alter states (Reinders PET data); longitudinal treatment outcome data showing that phase-based trauma therapy produces measurable improvement; and the theoretical coherence of structural dissociation theory with developmental trauma research and neuroscience.
The iatrogenic or sociocognitive model argues that DID is created through the interaction of a suggestible patient with a therapist who, often inadvertently, encourages the development and elaboration of alter states. Spanos (1994) proposed that alters are role enactments — patients adopt the role of "multiple personality" in response to therapist expectations, hypnotic suggestion, and cultural templates provided by media. Evidence cited by this model includes the dramatic increase in DID diagnoses in North America during the 1980s–1990s following the publication and TV adaptation of Sybil (1976); the concentration of diagnoses in a small number of specialist practitioners; the finding that some DID cases emerged in the context of controversial hypnotherapy and "memory recovery" techniques; and concerns about false memories, particularly involving the "satanic ritual abuse" moral panic of the 1980s, in which a number of patients came to "remember" elaborate ritual abuse scenarios that were almost certainly not real and that appeared to emerge through highly suggestive therapeutic practices.
The current scientific consensus occupies a middle position. DID is a genuine trauma-related dissociative disorder in the great majority of cases, and the neurobiological evidence makes a purely performance-based account untenable. However, the iatrogenic model identified real problems: hypnotherapy and suggestive memory-recovery techniques can elaborate or create spurious material; false memory risk is genuine and should inform therapeutic approach; the "satanic panic" cases involved genuine iatrogenic amplification of symptoms; and therapist expectations can shape symptom presentation. Current ISSTD guidelines explicitly recommend against using hypnosis for memory recovery, against leading questions about trauma content, and against techniques that encourage new alter formation. These guidelines represent the field's acknowledgment that, while DID is real, careful non-suggestive practice is essential to valid diagnosis and ethical treatment. The lesson of the controversy is not that DID does not exist, but that it must be diagnosed carefully and treated non-suggestively.
- Trauma model: DID from severe childhood trauma; genuine structural dissociation; supported by neuroimaging, cross-cultural data, treatment outcomes
- Iatrogenic model: DID created by therapist suggestion, hypnosis, media scripts; alters as role-enactment
- Evidence for trauma model: 90% trauma histories; cross-cultural occurrence; Reinders PET data; longitudinal treatment improvement
- Valid iatrogenic concerns: 1980s–90s satanic panic cases; hypnotherapy risks; false memory in suggestive recovery work
- Current consensus: DID is genuine; avoid hypnotherapy for memory recovery; avoid leading questions; non-suggestive practice is essential
- ISSTD 2011 guidelines: explicitly prohibit memory recovery hypnosis; recommend against alter proliferation encouragement
Key Research Papers
- Reinders AA, et al. One brain, two selves. NeuroImage. 2003;20(4):2119–2125 — Search PubMed — PET neuroimaging demonstrating distinct regional cerebral blood flow patterns between neutral and traumatic identity states in DID, not reproducible by healthy simulators.
- Brand BL, et al. Separating fact from fiction: An empirical examination of six myths about dissociative identity disorder. Harv Rev Psychiatry. 2016;24(4):257–270. PMID: 27384396 — Systematic empirical review rebutting six common clinical myths, including that DID is rare, iatrogenic, or feigned.
- International Society for the Study of Trauma and Dissociation. Guidelines for treating dissociative identity disorder in adults, third revision. J Trauma Dissociation. 2011;12(2):115–187 — Search PubMed — Comprehensive international clinical consensus guidelines; defines the phase-based treatment model.
- Myrick AC, et al. DID misdiagnosis as schizophrenia. J Psychiatr Pract. 2015;21(6):450–460 — Search PubMed — Literature review examining the overlap and misdiagnosis between DID and schizophrenia, with differentiation criteria.
- Loewenstein RJ. Dissociative identity disorder: an overview and clinical guide. Psychiatr Clin North Am. 2018;41(2):319–337 — Search PubMed — Comprehensive clinical review covering epidemiology, diagnosis, neurobiology, and treatment principles.
- Putnam FW, et al. The clinical phenomenology of multiple personality disorder: review of 100 recent cases. J Clin Psychiatry. 1986;47(6):285–293. PMID: 3711025 — Foundational clinical description of 100 MPD/DID cases documenting alter types, amnesia patterns, and trauma histories.
- van der Hart O, et al. The haunted self: structural dissociation and the treatment of chronic traumatization. Psychother Psychosom. 2006;75(4):195–197 — Search PubMed — Foundational exposition of the Structural Dissociation of the Personality theory underlying modern DID conceptualization.
- Sar V. The many faces of dissociation: opportunities for innovative research in psychiatry. Clin Psychopharmacol Neurosci. 2014;12(3):171–179 — Search PubMed — Overview of dissociation research landscape including epidemiology, neurobiology, and clinical implications.
- Dorahy MJ, et al. Dissociative identity disorder: an empirical overview. Aust N Z J Psychiatry. 2014;48(5):402–417 — Search PubMed — Systematic empirical overview of DID covering trauma etiology, prevalence, phenomenology, and treatment evidence.
- Bremner JD. Traumatic stress: effects on the brain. Dialogues Clin Neurosci. 2006;8(4):445–461 — Search PubMed — Review of neurobiological effects of early trauma including hippocampal and amygdala changes relevant to dissociative disorders.
- Ross CA, et al. Structured Interview for Dissociative Symptoms and PTSD in veterans. J Trauma Dissociation. 2021;22(1):114–131 — Search PubMed — Validation of structured dissociation assessment in a veteran sample, extending diagnostic research to trauma-exposed populations.
- Foote B, et al. Prevalence of dissociative disorders in psychiatric outpatients. J Nerv Ment Dis. 2006;194(12):915–920 — Search PubMed — Systematic prevalence study finding dissociative disorders in approximately 12.8% of psychiatric outpatients, demonstrating underrecognition.
PubMed Topic Searches
- Dissociative identity disorder treatment outcomes
- Structural dissociation personality disorder
- DID neuroimaging alter states
- Childhood trauma dissociation prevalence
- EMDR dissociative identity disorder
Connections
- Psychiatry
- PTSD
- Anxiety
- Depression
- Schizophrenia
- Borderline Personality Disorder
- Somatic Symptom Disorder
- Addiction
- Eating Disorders
- Insomnia
- Conversion Disorder (Functional Neurological Disorder)