Burnout: History and Discovery
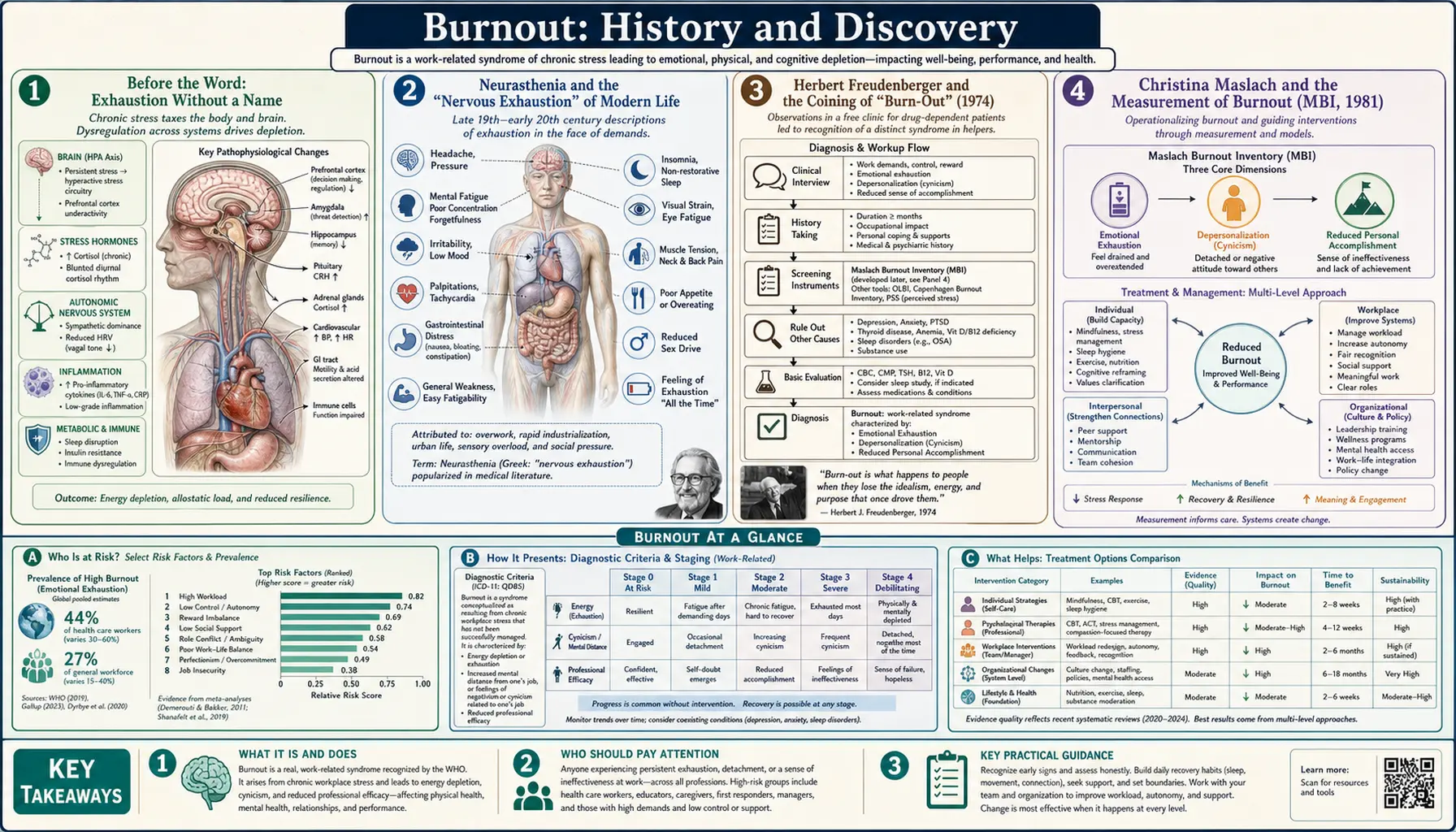
The word burnout entered the language of psychology only in the 1970s, yet the experience it names — the slow draining of energy, motivation, and feeling that comes from caring too hard for too long under too much pressure — is far older. This page traces how a colloquial term coined by a New York clinic psychologist in 1974 became a measured psychological construct, a focus of decades of workplace research, and finally an officially recognized entry in the World Health Organization's disease classification. One point deserves emphasis from the very start, because it is widely misunderstood: in the WHO's ICD-11, burnout is classified as an occupational phenomenon arising from chronic workplace stress — it is not a medical diagnosis, mental disorder, or disease. Understanding that distinction is itself part of burnout's history.
Table of Contents
- Before the Word: Exhaustion Without a Name
- Neurasthenia and the "Nervous Exhaustion" of Modern Life
- Herbert Freudenberger and the Coining of "Burn-Out" (1974)
- Christina Maslach and the Measurement of Burnout (MBI, 1981)
- Defining the Three Dimensions
- Burnout and Depression: An Unsettled Boundary
- WHO Recognition: An "Occupational Phenomenon," Not a Disease (ICD-11, 2019)
- The Modern Epidemic: Physicians, Workers, and the Pandemic Era
- Legacy: From Clinic Slang to a Global Conversation
- Research Papers and References
- Connections
- Featured Videos
Before the Word: Exhaustion Without a Name
People have always worn themselves out in the service of work and others, and the literatures of medicine, religion, and labor are full of descriptions that a modern reader recognizes instantly as burnout. Long before there was a clinical term, writers described clergy, physicians, soldiers, and caregivers collapsing into a state of depleted feeling and lost purpose after years of relentless demand. What changed in the twentieth century was not the experience but the naming of it: a shift from treating chronic exhaustion as a private moral failing or a vague nervous complaint to studying it as a measurable response to identifiable conditions.
Historians of the concept often point out that burnout, as we now understand it, is bound up with the rise of modern, bureaucratic, emotionally demanding service work — nursing, social work, teaching, medicine, policing, ministry. These are jobs in which a person is paid, in effect, to spend feeling on strangers, day after day, often with inadequate resources and limited control. The recognition that such work could produce a distinct and predictable form of depletion is the historical seed from which the modern construct grew. We cannot retroactively diagnose people in the past with a construct that did not yet exist and was not measured; what we can say is that the raw experience — emotional exhaustion, growing cynicism, and a sense of diminished effectiveness — is described again and again across centuries, which is part of why the term resonated so immediately once it was finally coined.
Neurasthenia and the "Nervous Exhaustion" of Modern Life
The most direct nineteenth-century ancestor of the burnout idea is neurasthenia, literally "weakness of the nerves." The American neurologist George Miller Beard brought the term to prominence in an 1869 article, "Neurasthenia, or Nervous Exhaustion," published in the Boston Medical and Surgical Journal (the forerunner of the New England Journal of Medicine). Beard described a syndrome of fatigue, depleted energy, headache, irritability, anxiety, and low mood, which he attributed to the exhaustion of the nervous system's finite energy reserves under the strain of modern life. (Beard popularized rather than invented the word, which had appeared earlier; the historical distinction between coining and popularizing is one this page is careful to make throughout.)
What makes neurasthenia such a striking forerunner is Beard's explanation for it. He blamed the accelerating pace of an industrializing, urbanizing society — famously naming forces such as steam power, the periodical press, the telegraph, and the sciences as drains on American nerves. He regarded the condition as so characteristically American that it acquired the nickname "Americanitis." In other words, a respected physician argued more than 150 years ago that the demands of modern work and technology could literally exhaust people into illness — an argument that echoes loudly in today's discussions of burnout, screens, and the always-on workplace.
Neurasthenia was not the same construct as burnout, and the comparison must be made carefully. Neurasthenia was framed as a medical disease of the nervous system, was applied to life in general rather than to work specifically, and eventually fell out of favor as a diagnosis in Western medicine (though related categories persisted elsewhere). Burnout, by contrast, would be defined a century later as a specifically work-related phenomenon and, crucially, would not be classified as a disease. Still, the through-line is clear: the intuition that sustained modern pressure produces a recognizable state of exhaustion did not begin in the 1970s.
Herbert Freudenberger and the Coining of "Burn-Out" (1974)
The modern psychological term was coined and popularized by Herbert J. Freudenberger (1926–1999), a German-born American psychologist who had fled Nazi Germany as a child refugee and built his career in New York. In the early 1970s Freudenberger volunteered, without pay, at a free clinic serving people with drug addiction and other needs. There he watched dedicated, idealistic volunteer staff — including himself — gradually lose their energy, enthusiasm, and commitment, becoming exhausted, irritable, cynical, and emotionally depleted after months of intense, under-resourced work with very difficult cases.
Freudenberger gave this pattern a name borrowed from colloquial speech — reportedly slang already used among drug users to describe the wasted, depleted state of chronic use — and applied it to the helping professionals he observed. His landmark paper, "Staff Burn-Out," appeared in 1974 in the Journal of Social Issues (volume 30, issue 1, pages 159–165). In it he described the physical signs (exhaustion, frequent illness, sleeplessness) and the behavioral and emotional signs (cynicism, irritability, rigidity, a loss of motivation and idealism) that he saw overtake committed staff in "alternative" care institutions.
Two things made Freudenberger's contribution historically pivotal. First, he located the problem in the interaction between a person and their working conditions, not merely in individual weakness — reframing exhaustion as something that happened to good, motivated people because of what they did and the conditions they did it under. Second, the word itself was vivid and immediately intuitive: it spread rapidly, first through the helping professions and then into general use. It is accurate to credit Freudenberger with introducing and popularizing "burnout" as a psychological term in 1974, while recognizing that he adapted an existing piece of slang rather than inventing the word from nothing.
Christina Maslach and the Measurement of Burnout (MBI, 1981)
If Freudenberger named burnout, the social psychologist Christina Maslach, of the University of California, Berkeley, did more than anyone to turn it into a researchable scientific construct. Working independently and at roughly the same time as Freudenberger, Maslach began in the early-to-mid 1970s to study how people in emotionally demanding human-services jobs coped with the strain of their work — how they managed their feelings, and what happened when those coping strategies failed. Her interviews with social workers, nurses, lawyers, and others surfaced the same recurring pattern of emotional depletion, detachment from the people they served, and a corroded sense of accomplishment.
Maslach's defining achievement was measurement. Together with Susan E. Jackson, she developed the Maslach Burnout Inventory (MBI), first published in 1981 in the paper "The measurement of experienced burnout" in the Journal of Occupational Behaviour (now the Journal of Organizational Behavior). The MBI was a self-report questionnaire that operationalized burnout as a quantifiable, three-part syndrome, allowing it to be studied systematically across occupations and populations for the first time. It rapidly became, and remains, the most widely used instrument for assessing burnout in research worldwide.
This is a crucial historical distinction to keep straight: Freudenberger supplied the coinage and the clinical observation; Maslach and Jackson supplied the operational definition and measurement. The two strands — clinical and social-psychological — developed largely in parallel before converging into the modern field. Maslach later collaborated with researchers such as Wilhelm Schaufeli and Michael Leiter to broaden the model beyond the original human-services focus toward burnout in the workplace generally, work synthesized in their influential 2001 Annual Review of Psychology article "Job Burnout."
Defining the Three Dimensions
The Maslach model defines burnout as a syndrome with three distinct dimensions, and this three-part structure has shaped essentially all subsequent thinking, including the WHO's official description. The first dimension is emotional exhaustion: the feeling of being emotionally overextended and drained of one's emotional and physical resources — the sense of having nothing left to give. This is the core stress dimension and the one most people mean when they say they are "burned out."
The second dimension is depersonalization — later often reframed as cynicism or mental distancing. It describes a negative, callous, or excessively detached response to other people, and a growing cynicism toward the work itself. In a caregiver this can look like treating patients or clients as impersonal objects rather than human beings; in other workers it appears as a hardened, disengaged, "why bother" attitude. Researchers have understood depersonalization in part as a defensive attempt to put distance between oneself and emotionally draining demands.
The third dimension is reduced personal accomplishment — later often termed reduced professional efficacy. This is a decline in one's feelings of competence and successful achievement at work, a corrosive sense that one is no longer effective or making a difference. Together, the three dimensions distinguish burnout from ordinary tiredness or simple job dissatisfaction: it is specifically the combination of being emotionally drained, growing cynically detached, and feeling ineffective. When the WHO later described burnout in the ICD-11, it used essentially these same three dimensions, a direct testament to the durability of the Maslach framework.
Burnout and Depression: An Unsettled Boundary
One of the most persistent scientific debates about burnout — and an honest history must present it as genuinely unresolved — concerns how it relates to depression. The two share substantial features: exhaustion and depleted energy, loss of interest and motivation, low mood, difficulty concentrating, and a bleak view of oneself and one's effectiveness. Because of this overlap, researchers have argued for decades about whether burnout is truly a distinct condition or whether it is, at least in part, a work-contextualized form of depression (or a state that frequently shades into one).
The scholarly literature reflects real disagreement. A frequently cited review of the burnout–depression overlap concluded that the conceptual distinction between the two is "fragile," and several researchers have warned that some people labeled as "burned out" may in fact have unrecognized, untreatable-by-vacation depressive or anxiety disorders that deserve proper clinical assessment and care. On the other side, many burnout researchers maintain that burnout is conceptually distinct — tied specifically to the work context, driven by identifiable workplace conditions, and centered on cynicism and inefficacy in ways that ordinary depression is not. The classification choice the WHO ultimately made (see below) effectively sided with treating burnout as a work-related phenomenon rather than as a mood disorder, without denying that the two can co-occur.
For a reader trying to make sense of their own experience, the practical takeaway is important and cautious: feeling burned out does not automatically mean one has clinical depression, but the symptoms overlap enough that the difference is not always obvious from the inside. Persistent low mood, hopelessness, loss of interest in everything (not just work), or any thoughts of self-harm are reasons to seek a clinical evaluation, regardless of which label fits best. This page describes a debated boundary; it is not a substitute for professional assessment.
WHO Recognition: An "Occupational Phenomenon," Not a Disease (ICD-11, 2019)
The single most consequential — and most widely misreported — event in burnout's recent history came in 2019, when the World Health Organization included burnout in the eleventh revision of the International Classification of Diseases (ICD-11). The ICD-11 was adopted by WHO member states at the 72nd World Health Assembly on 28 May 2019 and came into effect on 1 January 2022. Burnout appears under the code QD85.
The critical point, repeatedly stressed by the WHO itself, is where burnout sits in the classification. It is placed not among the mental, behavioral, or neurodevelopmental disorders, nor among diseases of any kind, but in a chapter titled "Factors influencing health status or contact with health services" — the part of the ICD that lists reasons people interact with health services that are not themselves illnesses. In the WHO's own words, burnout is "a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed," and it "is classified as an occupational phenomenon" that "is not classified as a medical condition." The WHO further specifies that the term refers specifically to phenomena in the occupational context and should not be applied to experiences in other areas of life.
The ICD-11 description characterizes burnout by three dimensions that map directly onto the Maslach model: feelings of energy depletion or exhaustion; increased mental distance from one's job, or feelings of negativism or cynicism related to one's job; and reduced professional efficacy. Because so many headlines in 2019 announced that the WHO had "recognized burnout as a disease" or a "medical condition," the organization issued clarifications, and it is important to state the fact plainly here: the WHO did not classify burnout as a medical condition or disease. It formally recognized it as an occupational phenomenon — a meaningful designation that legitimizes the experience and points to the workplace as its source, while deliberately stopping short of calling it an individual illness.
The Modern Epidemic: Physicians, Workers, and the Pandemic Era
From the 1980s onward, burnout research expanded from its original focus on human-services workers to nearly every kind of job, and by the early twenty-first century burnout had become a mainstream concern for employers, governments, and the public. Nowhere has the alarm been louder than in medicine. Large surveys have repeatedly found that a substantial share of physicians — in some reports roughly four in ten or more across many specialties — describe themselves as burned out, a finding that has driven a large body of research and a wave of institutional "wellness" initiatives. The medical profession's very public reckoning with burnout helped move the topic from academic journals into boardrooms and legislatures.
The COVID-19 pandemic that began in 2019–2020 intensified this conversation dramatically, as health-care workers, teachers, and many others faced prolonged, high-stakes stress with limited relief, and as remote and "always-on" work blurred the boundary between job and home for office workers. Burnout, already rising as a cultural preoccupation, became a defining feature of the era's discourse about work. (This page references that period only as historical context for burnout's prominence; it does not address the medical specifics of any infectious disease.)
This modern surge has also sharpened a debate about where responsibility lies. Maslach and other leading researchers have long argued that burnout is fundamentally a problem of the workplace — of excessive workload, lack of control, insufficient reward, unfairness, breakdown of community, and conflicts of values — and not merely a problem of individuals who need to be more "resilient." The WHO's decision to frame burnout as an occupational phenomenon resulting from chronic workplace stress aligns with that view, implying that the most effective remedies are organizational and structural, not only individual self-care.
Legacy: From Clinic Slang to a Global Conversation
In barely half a century, "burnout" traveled from a piece of colloquial slang adapted by one psychologist describing the volunteers at a New York free clinic, to a precisely measured three-dimensional construct, to an officially recognized entry in the world's standard health classification — and into everyday speech on every continent. Few psychological terms have spread so far, so fast. That speed is itself revealing: the word caught on because it named something a great many people already felt but had lacked the language to express.
The intellectual legacy rests on a few durable pillars. Freudenberger's 1974 coinage gave the experience a name and reframed it as something done to committed people by their conditions, not a private failing. Maslach and Jackson's 1981 inventory made it measurable and therefore scientific, and the three dimensions they defined — exhaustion, cynicism, and reduced efficacy — still organize the field. The WHO's 2019 classification gave the concept official standing while carefully defining its limits: an occupational phenomenon, rooted in the workplace, and explicitly not a disease.
For an ordinary reader, the history carries a clarifying message. If you feel emotionally drained, cynical about work you once cared about, and as though you are no longer effective, you are describing a phenomenon that has been studied for fifty years, named at the highest international level, and understood by leading researchers to arise largely from the conditions of work rather than from any weakness of your own — an understanding hard-won across the arc from neurasthenia to ICD-11.
Research Papers and References
The list below combines foundational, peer-reviewed sources on the history and definition of burnout with curated PubMed topic-search links and official WHO documentation. Real DOIs are given where they are confidently verified; otherwise links open a relevant PubMed topic search. Each link opens in a new tab.
- Freudenberger HJ. Staff Burn-Out. Journal of Social Issues. 1974;30(1):159–165. — doi:10.1111/j.1540-4560.1974.tb00706.x
- Maslach C, Jackson SE. The measurement of experienced burnout. Journal of Organizational Behavior. 1981;2(2):99–113. — doi:10.1002/job.4030020205
- Maslach C, Schaufeli WB, Leiter MP. Job Burnout. Annual Review of Psychology. 2001;52:397–422. — doi:10.1146/annurev.psych.52.1.397
- Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. 2016;15(2):103–111. — doi:10.1002/wps.20311
- Bianchi R, Schonfeld IS, Laurent E. Burnout–depression overlap: A review. Clinical Psychology Review. 2015;36:28–41. — doi:10.1016/j.cpr.2015.01.004
- Schonfeld IS, Bianchi R. Burnout and depression: two entities or one? Journal of Clinical Psychology. 2016;72(1):22–37. — doi:10.1002/jclp.22229
- World Health Organization. Burn-out an "occupational phenomenon": International Classification of Diseases (28 May 2019). — WHO news release
- Herbert J. Freudenberger and the making of burnout as a psychopathological syndrome (historical analysis). — PubMed: Freudenberger and the history of burnout
- Beard GM and the history of neurasthenia / nervous exhaustion. — PubMed: neurasthenia and George Beard, history
- History and concept of occupational burnout. — PubMed: history and concept of burnout
- Maslach Burnout Inventory: development, structure, and the three dimensions. — PubMed: Maslach Burnout Inventory dimensions
- ICD-11 burnout (QD85): meaning of the concept and prevalence. — PubMed: ICD-11 burnout as occupational phenomenon
- Physician burnout: prevalence, measurement, and workplace drivers. — PubMed: physician burnout prevalence and drivers
- Distinguishing burnout from depression: diagnostic and conceptual debate. — PubMed: burnout versus depression debate
External Authoritative Resources
- World Health Organization — Burn-out an "occupational phenomenon" (FAQ)
- ICD-11 for Mortality and Morbidity Statistics — QD85 Burn-out
- PubMed — All research on occupational burnout (history and definition)
Connections
- Psychiatry
- Burnout (Overview)
- All Conditions
- Depression
- Anxiety
- Chronic Fatigue Syndrome
- Adrenal Fatigue
- Insomnia