Metronidazole and Tinidazole for Trichomoniasis: Dosing, Safety, and Resistance
- How Nitroimidazoles Kill T. vaginalis
- CDC 2021 First-Line Dosing
- Tinidazole: The Preferred Agent
- Metronidazole: The Reliable Standard
- Side Effects and Tolerability
- The Alcohol Interaction
- Safety in Pregnancy
- Safety During Breastfeeding
- Nitroimidazole Resistance
- What Doesn't Work
- Key Research Papers
- Connections
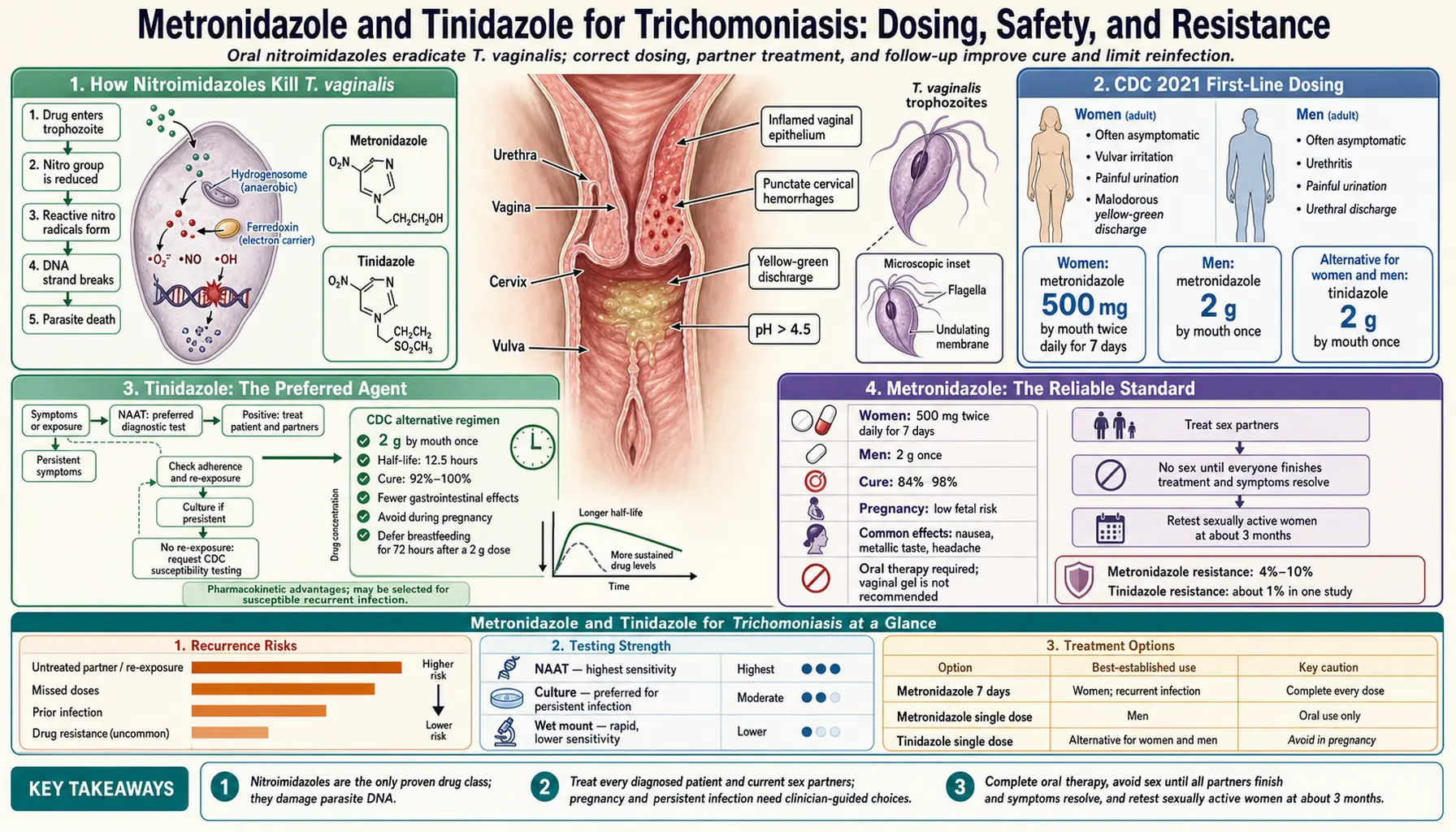
How Nitroimidazoles Kill T. vaginalis
Metronidazole and tinidazole are both 5-nitroimidazole prodrugs — meaning they are pharmacologically inactive as administered and must be metabolically activated inside the target organism to exert their lethal effect. This activation mechanism is what makes them selectively toxic to anaerobic and microaerophilic organisms like T. vaginalis while leaving most human cells unharmed.
The activation pathway works as follows: after entering the organism, the 5-nitro group of the drug molecule is reduced by ferredoxin and the enzyme pyruvate:ferredoxin oxidoreductase (PFOR), which are components of T. vaginalis's anaerobic energy metabolism. This reduction generates a highly reactive cytotoxic radical anion — a free radical species — that is the actual killing agent. The free radical attacks and fragments DNA, disrupting the helical structure, causing single- and double-strand breaks, and ultimately preventing DNA replication. The organism cannot repair this damage fast enough to survive, and cell death follows.
The reason this mechanism is selective for T. vaginalis (and other anaerobes like Bacteroides and anaerobic bacteria) rather than human cells is that the activation requires ferredoxin-dependent electron transport — a metabolic system present in hydrogenosomes (the anaerobic organelle unique to T. vaginalis) but absent from human mitochondria. Human cells do not reduce the nitroimidazole to its cytotoxic form, so the drug circulates harmlessly in systemic tissue while concentrating its destructive effect inside the parasite's own metabolic machinery. It is an elegant pharmacological trap: the organism's own survival mechanism becomes the instrument of its destruction.
Tinidazole reaches slightly higher intracellular concentrations due to its greater lipophilicity compared to metronidazole, which may partly explain its higher single-dose cure rates. Both drugs are well-absorbed orally (bioavailability >90%), widely distributed, and achieve therapeutic concentrations in the urogenital tract, urethra, Skene's glands, and bladder — all sites where T. vaginalis can colonize.
CDC 2021 First-Line Dosing
The CDC Sexually Transmitted Infections Treatment Guidelines, 2021 (MMWR 2021;70[No. RR-4]) represent the current authoritative standard. Key recommendations:
- Women — Recommended: Tinidazole 2g orally in a single dose
- Women — Alternative: Metronidazole 500mg orally twice daily for 7 days
- Men — Recommended: Metronidazole 2g orally in a single dose
- Men — Alternative: Tinidazole 2g orally in a single dose
The sex-differentiated dosing reflects anatomical and microbiological realities. In women, T. vaginalis colonizes not only the vaginal vault but also the urethra and Skene's glands (paraurethral glands adjacent to the urethral opening). These structures are harder to reach with a single-dose pulse that achieves peak-then-declining drug levels. Sustained systemic exposure — whether through tinidazole's longer half-life or metronidazole's 7-day course — more reliably eradicates organisms in these anatomical reservoirs. In men, the infection is primarily urethral and is effectively cleared by single-dose therapy; the urethral anatomy in men does not create the same reservoir problem.
All treatment courses should be taken with food to reduce nausea. Both tinidazole and metronidazole can be taken with or without food, but food consistently reduces GI side effects without affecting absorption. Patients should be instructed to avoid alcohol during and for 24 hours (metronidazole) or 72 hours (tinidazole) after completing treatment.
Tinidazole: The Preferred Agent
Tinidazole became the CDC-preferred first-line treatment for women with trichomoniasis in the 2021 guidelines, displacing the previous recommendation of metronidazole single-dose. This change was driven by compelling head-to-head trial data.
The pharmacokinetic advantages are significant. Tinidazole has a plasma half-life of 12-14 hours compared to approximately 8 hours for metronidazole. After a single 2g oral dose, tinidazole maintains therapeutic plasma concentrations for a longer period, allowing for more sustained exposure of T. vaginalis in the urogenital tract. Peak plasma concentrations are also somewhat higher with tinidazole due to greater lipophilicity and slightly better tissue penetration.
In randomized controlled trials directly comparing tinidazole 2g single dose versus metronidazole 2g single dose in women, tinidazole consistently achieves higher microbiological cure rates. A landmark 2018 Lancet Infectious Diseases study (Kissinger et al., PMID 30266571) of 623 women found that 7-day metronidazole (500mg BID) outperformed single-dose metronidazole (2g × 1), supporting the shift in guidelines. Multiple earlier trials (summarized in Schwebke 2004, PMID 15489348) showed tinidazole single dose curing approximately 92-95% of women vs 84-89% for metronidazole 2g single dose.
Tolerability is better with tinidazole: head-to-head studies consistently show less nausea with tinidazole than with metronidazole. Both cause a characteristic metallic or bitter taste that patients should be warned about in advance — this taste is not a sign of an adverse reaction but simply a side effect of the class.
The primary limitation of tinidazole is availability and cost. In some pharmacies, tinidazole is less commonly stocked than metronidazole and may be more expensive without insurance. In practice, clinicians should inquire about pharmacy availability before selecting tinidazole as the treatment, particularly for patients who need to fill a prescription that day.
Metronidazole: The Reliable Standard
Metronidazole has been the backbone of trichomoniasis treatment for over five decades and remains a valid, effective, and widely available treatment. First approved for trichomoniasis in the 1960s, it has been used in hundreds of millions of patients worldwide and has the most extensive human safety database of any agent in its class.
The two primary metronidazole regimens for women differ in cure rate and adherence demands. The 7-day course (500mg BID) achieves cure rates of 92-95% in women — comparable to tinidazole and meaningfully higher than the single-dose 2g regimen (84-89%). The 7-day course is now the preferred metronidazole regimen for women in the CDC guidelines when metronidazole is chosen. The 2g single dose is less preferred for women but remains the standard recommendation for men.
Why does the 7-day course outperform single dose in women? The sustained plasma concentrations over 7 days maintain therapeutic drug levels in the urethra and Skene's glands throughout the treatment period, allowing for more complete eradication of organisms in these anatomical sanctuaries. A single 2g pulse achieves high peak levels that then fall below therapeutic thresholds before all organisms in these sites are killed. Think of it as the difference between a single high-pressure spray versus a sustained flow: the sustained flow reaches more corners.
Metronidazole is available as a generic in both the 500mg tablet and 250mg tablet formulations, and is considerably cheaper than tinidazole at most pharmacies. For patients without prescription drug coverage, this cost difference can be clinically significant. Metronidazole is also available intravenously for patients unable to tolerate oral administration, though IV administration is rarely necessary for trichomoniasis.
Side Effects and Tolerability
Both metronidazole and tinidazole are generally well-tolerated at the doses used for trichomoniasis. The most clinically important side effects to counsel patients about are gastrointestinal.
Nausea is the most common adverse effect, occurring in approximately 10-20% of patients taking metronidazole and somewhat less frequently with tinidazole. Taking the medication with food substantially reduces nausea. For patients taking the 7-day metronidazole course who develop significant nausea, dividing the dose (250mg QID rather than 500mg BID) can sometimes improve tolerability while maintaining equivalent daily dose exposure.
Metallic or bitter taste is a characteristic effect of both agents, described by patients as a persistent bitter or metallic sensation in the mouth during and shortly after the treatment course. It typically resolves within 24-48 hours of completing treatment. Warn patients about this in advance to prevent unnecessary concern or early discontinuation.
Headache and dizziness occur in a minority of patients, are usually mild, and resolve with dose completion. Patients should be cautioned against driving or operating heavy machinery if they experience significant dizziness.
Peripheral neuropathy — tingling, numbness, or weakness in the extremities — is a rare adverse effect associated almost exclusively with prolonged high-dose use (weeks to months), not with the short courses used for trichomoniasis. Patients can be reassured that a 7-day course or single dose does not carry meaningful peripheral neuropathy risk.
Seizures have been reported rarely with very high doses in patients with CNS abnormalities. Standard trichomoniasis doses do not present significant seizure risk in otherwise healthy patients. Metronidazole does penetrate the CNS and should be used cautiously in patients with seizure disorders.
Drug interactions: Both agents may enhance the anticoagulant effect of warfarin (INR monitoring recommended in patients on warfarin). Lithium toxicity has been reported with metronidazole use; lithium levels should be monitored. Both agents can cause disulfiram-like reactions with alcohol — discussed below.
The Alcohol Interaction
The alcohol-nitroimidazole interaction is one of the most important counseling points when prescribing these medications, and it must be communicated clearly to every patient. The interaction produces a disulfiram-like reaction: both metronidazole and tinidazole inhibit aldehyde dehydrogenase, the enzyme that breaks down acetaldehyde (the first metabolic product of alcohol). When alcohol is consumed, acetaldehyde accumulates in the bloodstream, causing a toxic reaction characterized by intense flushing, nausea, vomiting, headache, and tachycardia. In severe cases, hypotension and chest pain can occur. The reaction is unpleasant and potentially dangerous, and it is entirely preventable with adequate patient education.
Metronidazole: Avoid all alcoholic beverages (including beer, wine, spirits) and any product containing significant amounts of ethanol (some mouthwashes, liquid medications) during the treatment course and for 24 hours after the last dose.
Tinidazole: Avoid alcohol during the treatment course and for 72 hours after the last dose. The extended window reflects tinidazole's longer half-life — it takes longer to be cleared from the body, and enzyme inhibition persists for a corresponding longer period.
Clinicians should not assume that a brief mention of "avoid alcohol" is sufficient. Patients need to hear the specific duration, understand why the restriction applies, and be told what the consequence of ignoring it is. A practical framing: "If you take even one drink while this medication is in your system, you will feel very sick very quickly — flushing, nausea, possibly vomiting. It's not dangerous in most cases but it's very unpleasant, and it's completely avoidable by just waiting." That level of specificity is what produces reliable adherence.
Safety in Pregnancy
Trichomoniasis during pregnancy is associated with preterm birth, premature rupture of membranes, low birthweight, and increased risk of neonatal transmission. Treatment is therefore indicated in pregnancy, and concerns about antibiotic safety should not delay treatment once the diagnosis is made.
Metronidazole in pregnancy: FDA Pregnancy Category B. Large population-based studies and multiple meta-analyses have found no increased risk of congenital malformations, miscarriage, or adverse neonatal outcomes associated with metronidazole use in any trimester, including the first. The first-trimester caution that appeared in older guidelines was based on theoretical concerns from rodent studies (where doses far exceeding human therapeutic levels were used) that have not been replicated in human observational data. The 2021 ACOG guidelines explicitly state that metronidazole is safe throughout pregnancy. The 7-day course (500mg BID) is preferred over the 2g single dose in pregnancy, as some studies suggest higher single-dose regimens may have a modest association with preterm birth when used in the second trimester (the evidence is not definitive, but precautionary dosing is reasonable).
Tinidazole in pregnancy: Data are insufficient to make a definitive safety statement. Animal studies have shown embryotoxicity at high doses. Tinidazole is generally not recommended in the first trimester. For second and third trimester use when metronidazole is not tolerated, tinidazole may be considered after discussing the limited safety evidence with the patient. Metronidazole should be used in preference when available.
Test-of-cure in pregnancy: The CDC recommends retesting at 4-6 weeks after treatment in pregnant women, rather than the 3-month window recommended for non-pregnant women. The stakes of reinfection during pregnancy — particularly in the third trimester — are high enough that earlier rescreening is warranted.
Safety During Breastfeeding
Both metronidazole and tinidazole pass into breast milk. The clinical implications depend on which agent is used and whether a single dose or multi-day course is employed.
Metronidazole 2g single dose: Drug concentrations in breast milk peak at approximately 1-2 hours after the dose and then decline. The American Academy of Pediatrics recommends withholding breastfeeding for 12-24 hours after a single 2g dose to allow for clearance. After this window, breastfeeding can be safely resumed. Mothers may wish to pump and discard breast milk during this period to maintain milk supply.
Metronidazole 500mg BID × 7 days: The lower peak concentrations with divided dosing mean that infant exposure per feeding is substantially lower than with the 2g single dose. Most clinicians and the AAP support continuing breastfeeding during the 7-day course, with monitoring for any signs of GI disturbance (diarrhea, fussiness) in the infant. The infant's exposure through breast milk represents a small fraction of an infant dose and is generally considered acceptable.
Tinidazole single dose: Due to tinidazole's longer half-life (12-14 hours) and more prolonged presence in breast milk, the recommended withholding period is longer. The AAP recommends withholding breastfeeding for 72 hours after a single 2g tinidazole dose. Mothers who find this 72-hour interruption impractical may prefer the metronidazole 7-day course for this reason alone.
Clinicians should have this conversation proactively, not as an afterthought. Knowing in advance that they can breastfeed through a 7-day course (with monitoring) may influence which regimen a breastfeeding patient prefers — a patient-centered consideration that is medically valid.
Nitroimidazole Resistance
Clinically significant nitroimidazole resistance in T. vaginalis occurs in approximately 5% of clinical isolates — a minority but a meaningful one given the volume of infections. Resistance is classified by the minimum lethal concentration (MLC) required to kill the organism under anaerobic conditions in vitro: low-level resistance (MLC 50-100 µg/mL) versus high-level resistance (MLC >100 µg/mL).
The molecular mechanisms of resistance center on impairment of the reductive activation pathway. Low-level resistance most commonly involves partial reduction in ferredoxin or PFOR activity, reducing (but not eliminating) prodrug activation. High-level resistance typically involves more complete loss of PFOR function combined with upregulation of flavin reductases that scavenge and neutralize the cytotoxic radical anions before they can damage DNA. The result is an organism that the drug reaches but cannot kill at standard doses.
Clinical recognition of resistance: when a patient presents with persistent or recurrent positive NAAT after confirmed adequate treatment AND confirmed partner treatment, resistance should be considered. However, reinfection is far more common than true resistance — the first step is always to determine whether the partner was truly treated. True resistance should only be assumed after ruling out reinfection.
In vitro susceptibility testing is available through the Centers for Disease Control and Prevention's reference laboratory. Clinicians can contact the CDC STD Treatment Hotline (1-800-CDC-INFO) to arrange testing of clinical isolates. Management of documented resistant cases: tinidazole 2g twice daily for 14 days (off-label, supported by case series data); in some cases, compounded tinidazole intravaginal gel is added to systemic therapy. Expert consultation via the CDC hotline is recommended before embarking on high-dose prolonged therapy.
What Doesn't Work
A number of commonly tried alternatives to systemic nitroimidazole therapy have no clinical evidence supporting efficacy against T. vaginalis:
Topical metronidazole vaginal gel (0.75%): This is perhaps the most common clinical error in trichomoniasis management. Vaginal gel does achieve adequate local concentrations in the vaginal vault, but not in the urethra, paraurethral glands, or bladder — all of which may harbor T. vaginalis. The CDC explicitly states that topical preparations are not effective for trichomoniasis treatment. Use of vaginal gel will typically reduce vaginal organism load (and may partially relieve symptoms) while leaving urethral reservoirs intact, leading to apparent treatment failure or rapid recurrence.
Boric acid vaginal suppositories: Effective for certain vaginal conditions (particularly recurrent yeast infections and some cases of bacterial vaginosis) but have no documented activity against T. vaginalis. Sometimes combined with metronidazole vaginal gel in compound prescriptions — the metronidazole component is ineffective for TV (see above), and the boric acid adds no benefit.
Tea tree oil, apple cider vinegar, hydrogen peroxide douches, and other OTC alternatives: No clinical evidence of efficacy against T. vaginalis. Some of these preparations disrupt normal vaginal flora, potentially worsening bacterial vaginosis (which frequently co-occurs with TV). Douching in particular is associated with worse outcomes in TV infection and should be actively discouraged.
Other antibiotic classes: T. vaginalis is resistant to the antibiotics used for bacterial STIs (azithromycin, doxycycline, cephalosporins, fluoroquinolones). Prescribing these for a TV diagnosis is not only ineffective but misses the diagnosis and allows active infection to persist. If these antibiotics are prescribed empirically for vaginal discharge before testing results return, the test result must be reviewed and nitroimidazole added if TV is found.
Key Research Papers
- Kissinger P, Muzny CA, Mena LA, et al. Single-dose versus 7-day-dose metronidazole for the treatment of trichomoniasis in women. Lancet Infect Dis. 2018;18(11):1251-1259 — Search PubMed
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187. PMID: 34292926
- Schwebke JR, Barrientes FJ. Prevalence of Trichomonas vaginalis isolates with resistance to metronidazole and tinidazole. Antimicrob Agents Chemother. 2006;50(12):4209-4210 — Search PubMed
- Cudmore SL, Delgaty KL, Hayward-McClelland SF, et al. Treatment of infections caused by metronidazole-resistant Trichomonas vaginalis. Clin Microbiol Rev. 2004;17(4):783-793 — Search PubMed
- Wendel KA, Workowski KA. Trichomoniasis: challenges to appropriate management. Clin Infect Dis. 2007;44(Suppl 3):S123-S129. PMID: 17342672
- Forna F, Gülmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev. 2003;(2):CD000218 — Search PubMed
- Schwebke JR, Burgess D. Trichomoniasis. Clin Microbiol Rev. 2004;17(4):794-803 — Search PubMed
- Kissinger P, Amedee A, Clark RA, et al. Trichomonas vaginalis treatment reduces vaginal HIV-1 shedding. Sex Transm Dis. 2009;36(1):11-16 — Search PubMed
- Helms DJ, Mosure DJ, Metcalf CA, et al. Management of Trichomonas vaginalis in women with suspected metronidazole hypersensitivity. Am J Obstet Gynecol. 2008;198(4):370.e1-7 — Search PubMed
- Lyng J, Christensen J. A double-blind study of the value of treatment with a single dose tinidazole of partners to females with trichomoniasis. Acta Obstet Gynecol Scand. 1981;60(2):199-201 — Search PubMed
Connections
- All Parasites
- Treatments Hub
- Trichomonas vaginalis — Overview
- Symptoms Hub
- Vaginal & Urethral Symptoms
- Complications & Pregnancy Risks
- Partner Treatment & Reinfection
- Prevention & Screening
- Reproductive Medicine