Trichomonas vaginalis Complications: HIV Risk and Pregnancy Outcomes
- HIV Acquisition Risk
- HIV Transmission from HIV+ Individuals
- Preterm Birth Risk
- Low Birth Weight and PPROM
- BV Co-Infection
- PID Risk
- Cervical Cancer and HPV
- Male Fertility Impact
- Prostatitis and Epididymitis
- Neonatal Infection
- Key Research Papers
- Connections
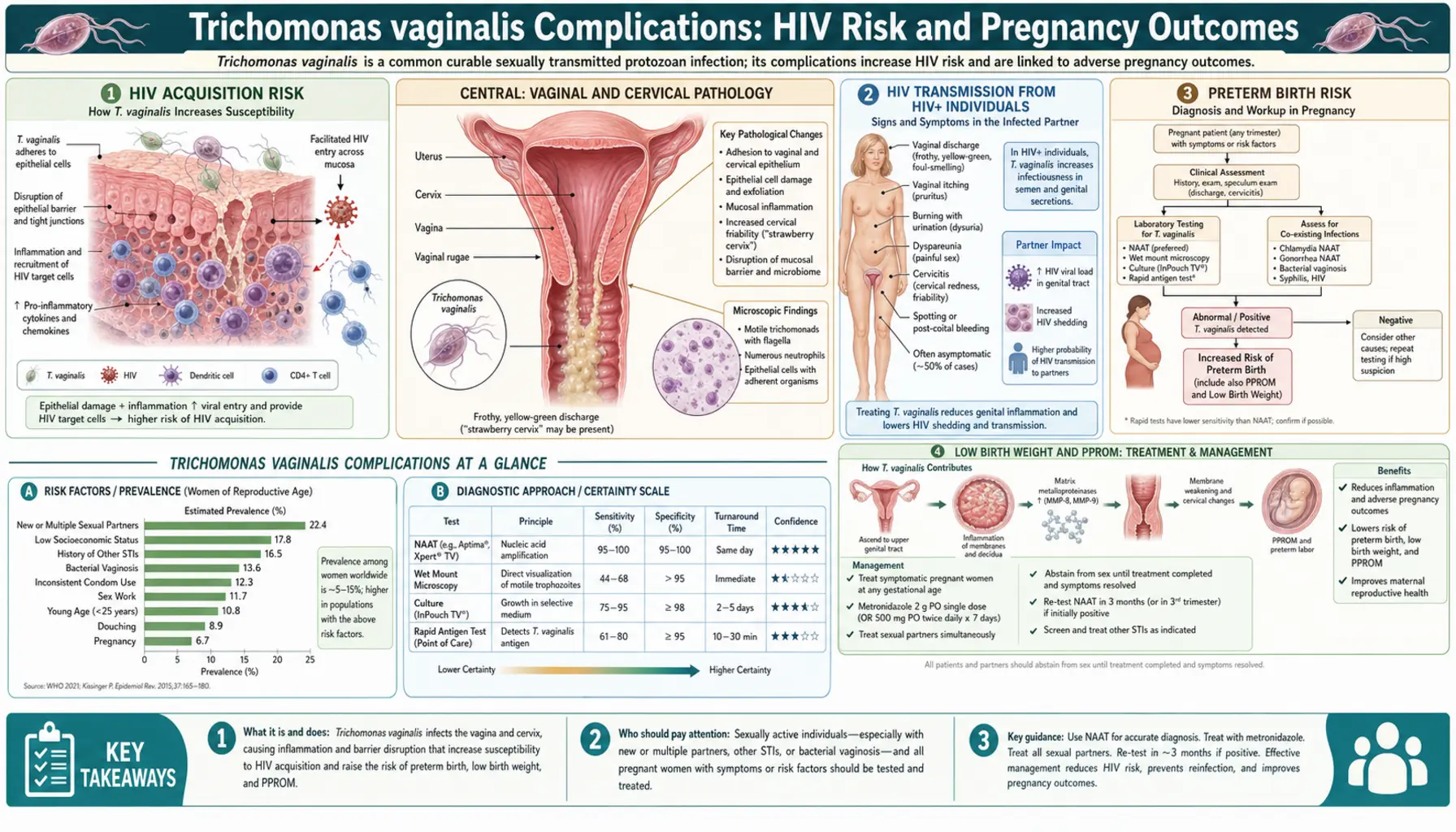
HIV Acquisition Risk
Trichomonas vaginalis infection is one of the most significant biological cofactors for HIV acquisition in women. Studies from sub-Saharan Africa, the United States, and other high-prevalence settings consistently show that women infected with T. vaginalis are 1.5–3 times more likely to acquire HIV upon exposure compared to uninfected women. This elevated risk persists after controlling for known behavioral risk factors, indicating a direct biological mechanism rather than confounding by shared risk behaviors.
The mechanism has several components. First, T. vaginalis directly disrupts the vaginal epithelial barrier through mechanical attachment (the parasite actively adheres to epithelial cells and causes cellular disruption) and enzymatic degradation of extracellular matrix proteins including fibronectin, type IV collagen, and laminin via cysteine proteases and serine proteases. This breakdown of the epithelial layer eliminates the physical barrier that normally limits HIV transcytosis across genital mucosa ( — Search PubMed).
Second, and perhaps more important, T. vaginalis triggers a robust mucosal inflammatory response. The parasite activates toll-like receptor 4 (TLR4) signaling via its lipophosphoglycan surface molecules, triggering release of pro-inflammatory cytokines including IL-1β, IL-6, IL-8, and TNF-α from vaginal epithelial cells and resident immune cells. This inflammatory milieu recruits CD4+ T lymphocytes and macrophages — the primary target cells for HIV-1 — to the genital mucosa in large numbers. HIV, if present in a male partner's ejaculate, is thus presented to a genital tissue environment dense with its own target cells and with a compromised epithelial barrier ( — Search PubMed).
Third, the elevated vaginal pH that accompanies TV infection (above 4.5) reduces the antimicrobial activity of lactic acid against HIV and other pathogens, further lowering the protective threshold at the genital surface.
The public health implication is substantial. In high TV-prevalence populations — Black women in the US, women in sub-Saharan Africa — the attributable fraction of HIV incidence due to TV co-infection is estimated to be substantial. Mathematical modeling suggests that aggressive treatment of TV in high-prevalence settings could meaningfully reduce HIV incidence, though this has been difficult to demonstrate definitively in individual randomized trials due to the complexity of measuring incident HIV.
HIV Transmission from HIV+ Individuals
The relationship between T. vaginalis and HIV is bidirectional. HIV-positive women infected with T. vaginalis have significantly higher concentrations of HIV-1 RNA in cervicovaginal secretions compared to HIV-positive women without TV. Studies have measured a 2- to 5-fold increase in cervicovaginal HIV-1 viral load associated with TV co-infection, and this increase resolves following TV treatment ( — Search PubMed).
The mechanism is parallel to the acquisition pathway: TV-driven genital inflammation recruits HIV-infected CD4+ T cells and macrophages to the mucosa, where they release virus into genital secretions. The disrupted epithelial barrier also reduces compartmentalization, allowing deeper tissue pools of HIV to contribute to surface viral load. The net result is that an HIV-positive woman co-infected with T. vaginalis is more infectious to her sexual partners than she would be without TV infection.
Similarly, HIV-positive men with TV urethritis have higher HIV-1 concentrations in seminal fluid. Treating TV in HIV-positive individuals — both to reduce infectiousness and to improve their own immune health — is therefore an important component of HIV care. Current CDC guidelines recommend annual TV screening for all HIV-positive sexually active individuals ( — Search PubMed).
Preterm Birth Risk
Multiple observational studies and meta-analyses have found associations between T. vaginalis infection in pregnancy and an increased risk of preterm birth (delivery before 37 weeks gestation). Odds ratios from the most rigorous studies range from approximately 1.3 to 1.8, meaning infected pregnant women have 30–80% higher odds of delivering preterm compared to uninfected women ( — Search PubMed).
The proposed mechanism involves the ascending spread of T. vaginalis from the vagina through the cervix into the lower uterine segment and amniotic space, where it can trigger a local inflammatory response. Prostaglandins (particularly PGE2 and PGF2α) and inflammatory cytokines (IL-1β, IL-6, IL-8) produced in response to the infection can stimulate uterine contractions and cervical ripening — processes that normally occur at term but that, when triggered prematurely, lead to preterm labor.
Additionally, TV co-infection with bacterial vaginosis (which occurs in 30–40% of TV cases) amplifies these pro-inflammatory cascades. BV-associated bacteria and their metabolic products further stimulate prostaglandin production and degrade the cervical mucus barrier, potentially allowing more organisms to ascend into the upper reproductive tract.
The important nuance here is that the evidence for association does not automatically mean that treating TV in pregnancy will prevent preterm birth. This was tested directly in a large randomized controlled trial — the results of which are described below — with disappointing results for the preterm birth prevention hypothesis.
Low Birth Weight and PPROM
Beyond preterm birth, T. vaginalis in pregnancy is associated with low birth weight (birth weight below 2,500 grams) and premature rupture of membranes (PPROM — rupture of the amniotic sac before labor begins at term, or before 37 weeks in the case of pre-term PPROM). These outcomes frequently overlap with preterm birth but represent distinct pathological pathways.
Low birth weight from TV infection may result partly from the shorter gestational age if preterm birth occurs, but also from placental inflammation that impairs nutrient transfer independent of gestational age. Studies have documented placental inflammation in women with TV infection at the time of delivery, suggesting a direct effect on fetal growth that may occur even in women who deliver at term ( — Search PubMed).
PPROM is thought to occur via a similar mechanism to preterm birth — inflammatory cytokines and prostaglandins weaken the amniotic membranes, reducing their tensile strength so that they rupture before labor is established. TV-associated BV co-infection, with its production of collagenases and mucinases by anaerobic bacteria, may directly degrade membrane integrity.
The landmark Klebanoff trial (2001), which randomized 617 asymptomatic TV-infected pregnant women to metronidazole versus placebo, found that treatment did not reduce preterm birth — and in fact, one analysis suggested a potential increase in preterm delivery in the treatment group ( — Search PubMed). This paradoxical finding may reflect the inflammatory response to dying organisms, or may indicate that the inflammatory cascade leading to preterm birth is already irreversibly initiated by the time treatment is given in the second trimester. Regardless, treatment is still recommended in symptomatic pregnant women for symptom relief and partner protection, and metronidazole is safe in all trimesters.
BV Co-Infection
The co-occurrence of T. vaginalis infection and bacterial vaginosis is documented in approximately 30–40% of TV-infected women, making it the most common clinically significant co-infection in this context. The two conditions share anatomical territory (the vaginal lumen and epithelia), share risk factors, and appear to interact bidirectionally in ways that amplify the adverse consequences of each.
T. vaginalis creates conditions favorable to BV by: consuming Lactobacillus (which are part of its diet and which provide the competitive exclusion that normally suppresses BV-associated bacteria), elevating vaginal pH (which suppresses Lactobacillus acid production and promotes anaerobe growth), and disrupting the vaginal epithelium that Lactobacillus normally adhere to and colonize. BV, in turn, may enhance TV colonization by reducing innate immune defenses and altering the local microbial ecology ( — Search PubMed).
In pregnancy, the combination is particularly dangerous. BV alone is the strongest known risk factor for preterm birth, with odds ratios of 2–6 in various studies. When co-occurring with TV, the combined pro-inflammatory and pro-contractile effects are additive or possibly synergistic, producing a substantially higher risk of adverse outcomes than either condition alone. Both conditions should be sought and treated when identified in pregnant women, using systemic metronidazole rather than topical gel (which is adequate for BV alone but may not adequately treat TV).
PID Risk
Pelvic inflammatory disease (PID) — infection and inflammation of the upper female reproductive tract including the uterus, fallopian tubes, and ovaries — is most commonly caused by Neisseria gonorrhoeae and Chlamydomonas trachomatis. Trichomonas vaginalis is an under-recognized contributor to PID but is rarely the sole causative organism.
T. vaginalis can ascend to the upper reproductive tract, particularly in conditions of altered cervical mucus (which normally acts as a barrier to ascending infection), concurrent BV (which disrupts the mucus barrier), or instrumentation (IUD insertion, hysterosalpingography). TV has been isolated from fallopian tube tissue and peritoneal fluid in women with PID, though the frequency is much lower than for gonorrhea or chlamydia.
More importantly, TV-induced lower genital tract inflammation may facilitate ascending infection by N. gonorrhoeae or C. trachomatis — the mucosal disruption and elevated local immune cell density that T. vaginalis creates may enable these pathogens to more readily penetrate the cervical barrier. Given the shared sexual transmission route and high co-infection rates with other STIs, TV testing should be included whenever PID is being evaluated ( — Search PubMed).
Cervical Cancer and HPV
An association between T. vaginalis infection and cervical cancer risk has been suggested in several epidemiological studies, though the relationship is confounded by shared risk factors with human papillomavirus (HPV), the established causal agent of cervical cancer. Higher HPV acquisition rates and persistent HPV infection have been observed in TV-infected women compared to uninfected women.
The proposed mechanism is indirect: TV-driven genital inflammation and epithelial disruption may enhance HPV acquisition and reduce the immune surveillance that normally clears HPV infections. Cervical inflammation itself is associated with impaired immune control of HPV, and women with chronic or recurrent TV infection may have a higher burden of cervical inflammatory stress over time.
Some case-control studies have found elevated TV seropositivity rates in women with cervical cancer compared to controls after adjusting for HPV exposure, but these findings have not been consistent across all studies. The current clinical guidance does not establish TV as an independent carcinogen — the recommendation is to screen for and treat TV for its established harms (HIV risk, pregnancy complications), not specifically for cervical cancer prevention ( — Search PubMed).
Male Fertility Impact
In men, T. vaginalis infection has documented adverse effects on sperm quality and function. Studies comparing sperm parameters in TV-infected versus uninfected men have found significant reductions in sperm motility (both total and progressive motility), increased rates of sperm DNA fragmentation, higher proportions of morphologically abnormal sperm, and in some studies, decreased sperm concentration and viability.
The mechanism of sperm damage is thought to involve both direct effects and oxidative stress. T. vaginalis produces a spermicidal factor — a contact-dependent cytotoxin — that directly damages sperm cell membranes at high organism concentrations. The parasite also activates complement-mediated sperm killing via its cell-surface molecules. Additionally, the seminal fluid inflammatory response to TV infection (elevated IL-6, IL-8, reactive oxygen species) causes oxidative damage to sperm DNA and membranes ( — Search PubMed).
For couples experiencing unexplained infertility, TV infection in the male partner is an underappreciated potential contributor. TV testing is not routinely part of male fertility evaluation but should be considered, particularly in men with documented leukospermia (elevated white blood cells in semen, indicating genital tract inflammation) or suboptimal sperm parameters without other identified cause. Treatment successfully clears the organism and appears to improve sperm parameters in infected men.
Prostatitis and Epididymitis
Beyond urethritis, T. vaginalis can spread to the prostate gland and epididymis in men. TV has been cultured from expressed prostatic secretions and from prostatic tissue biopsies in men with prostatitis-like symptoms, and TV DNA has been detected by PCR in prostate tissue samples in epidemiological studies.
Prostatic involvement by TV may manifest as chronic pelvic pain syndrome (Category III prostatitis in NIH classification), with symptoms of pelvic pressure, perineal discomfort, pain with ejaculation, and post-ejaculatory pain. These symptoms are common and non-specific, making TV a frequently missed contributor to chronic prostatitis that is typically attributed to other causes or treated empirically with antibiotics having no TV activity ( — Search PubMed).
Epidemiological studies have found higher TV seropositivity in men with prostate cancer compared to those without, with some meta-analyses reporting OR approximately 1.5–1.8 for prostate cancer in TV-seropositive men. The biological plausibility involves chronic prostatic inflammation as a promoter of carcinogenesis. However, these associations are observational and do not establish causation — confounding by sexual activity levels and other factors cannot be fully excluded. TV screening is not yet recommended for prostate cancer prevention, but the association reinforces the importance of treating TV in symptomatic men.
Neonatal Infection
Neonatal T. vaginalis infection is rare but documented. Infants can acquire the infection during passage through an infected birth canal during vaginal delivery. The most common manifestation in neonates is respiratory trichomoniasis — the organism colonizes the respiratory tract, which is lined by epithelium susceptible to TV, and can cause rhinitis, nasal discharge, and in some case reports, pneumonia.
Neonatal TV infection may also manifest as vaginal discharge in female neonates, representing colonization of vaginal epithelium that remains susceptible due to maternal estrogen exposure in utero. This typically resolves as maternal estrogen effects wane in the first weeks of life and the vaginal epithelium matures ( — Search PubMed).
The incidence of neonatal TV infection is not well-characterized due to limited surveillance, but it is considered uncommon. The primary motivation for identifying and treating TV in pregnant women is not prevention of neonatal infection per se, but rather the maternal complications of preterm birth, HIV risk amplification, and symptomatic disease. However, appropriate diagnosis and treatment of infected mothers before delivery will also prevent neonatal exposure.
Key Research Papers
- Kissinger P. "Trichomonas vaginalis: a review of epidemiologic, clinical and treatment issues." BMC Infect Dis. 2015;15:307 — Search PubMed
- Schwebke JR, Burgess D. "Trichomoniasis." Clin Microbiol Rev. 2004;17(4):794-803 — Search PubMed
- Sutton M, et al. "Prevalence of Trichomonas vaginalis infection among females in the United States, 2001-2004." Clin Infect Dis. 2007;45(10):1319-1326 — Search PubMed
- Dize L, et al. "Comparison of self-obtained penile-meatal swabs for detection of Trichomonas vaginalis." Sex Transm Dis. 2013 — Search PubMed
- Workowski KA, Bolan GA. "Sexually Transmitted Diseases Treatment Guidelines, 2015." MMWR Recomm Rep. 2015;64(RR-03):1-137 — Search PubMed
- Van Der Pol B, et al. "Clinical and laboratory testing for Trichomonas vaginalis infection." J Clin Microbiol. 2016;54(7):1832-1840 — Search PubMed
- Muzny CA, et al. "Trichomoniasis in women and its treatment." Best Pract Res Clin Obstet Gynaecol. 2019;55:2-9 — Search PubMed
- Klebanoff MA, et al. "Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection." N Engl J Med. 2001;345(7):487-493 — Search PubMed
- Kissinger P, et al. "Patient-delivered partner treatment for Trichomonas vaginalis infection." Sex Transm Dis. 2006;33(7):445-450 — Search PubMed
- Meites E, et al. "A review of evidence-based care of symptomatic trichomoniasis and asymptomatic Trichomonas vaginalis infections." Clin Infect Dis. 2015;61(Suppl 8):S837-S848 — Search PubMed
Connections
- All Parasites
- Trichomonas vaginalis Overview
- Symptoms Hub
- Vaginal & Urethral Symptoms
- Diagnosis: Wet Mount & NAAT
- Treatments Overview
- Reproductive Medicine
- Infectious Disease