Food Intolerance: History and Discovery
People have reacted badly to particular foods for as long as people have eaten, but the idea that there is a distinct, non-immune kind of food reaction — a food intolerance, separate from a true allergy — is surprisingly modern. It took the twentieth century to draw the line: in 1906 the Austrian physician Clemens von Pirquet coined the word allergy for an altered immune reactivity, and only later did medicine recognize that many of the most common adverse reactions to food are not immune at all but the predictable result of a missing enzyme, a pharmacologically active food chemical, or a fermentable carbohydrate. The clearest example is lactose intolerance, whose physiology was worked out in the 1960s and whose evolutionary genetics — the “lactase persistence” that lets many adults of dairying ancestry keep digesting milk — were pinned to a single DNA variant in 2002. This page traces how the concept of food intolerance was distinguished from allergy and from celiac disease, and how its individual mechanisms were discovered.
Table of Contents
- Allergy vs. Intolerance: Drawing the Line
- Lactose Intolerance: Working Out the Physiology
- Lactase Persistence and the Genetics of Milk-Drinking
- Inborn Errors: Hereditary Fructose Intolerance and Favism
- Pharmacological Reactions: Histamine and Vasoactive Amines
- Food Additives and the MSG Myth
- The FODMAP Concept and Modern IBS Diets
- A Modern, Mechanism-Based Map
- Research Papers and References
- Connections
- Featured Videos
Allergy vs. Intolerance: Drawing the Line
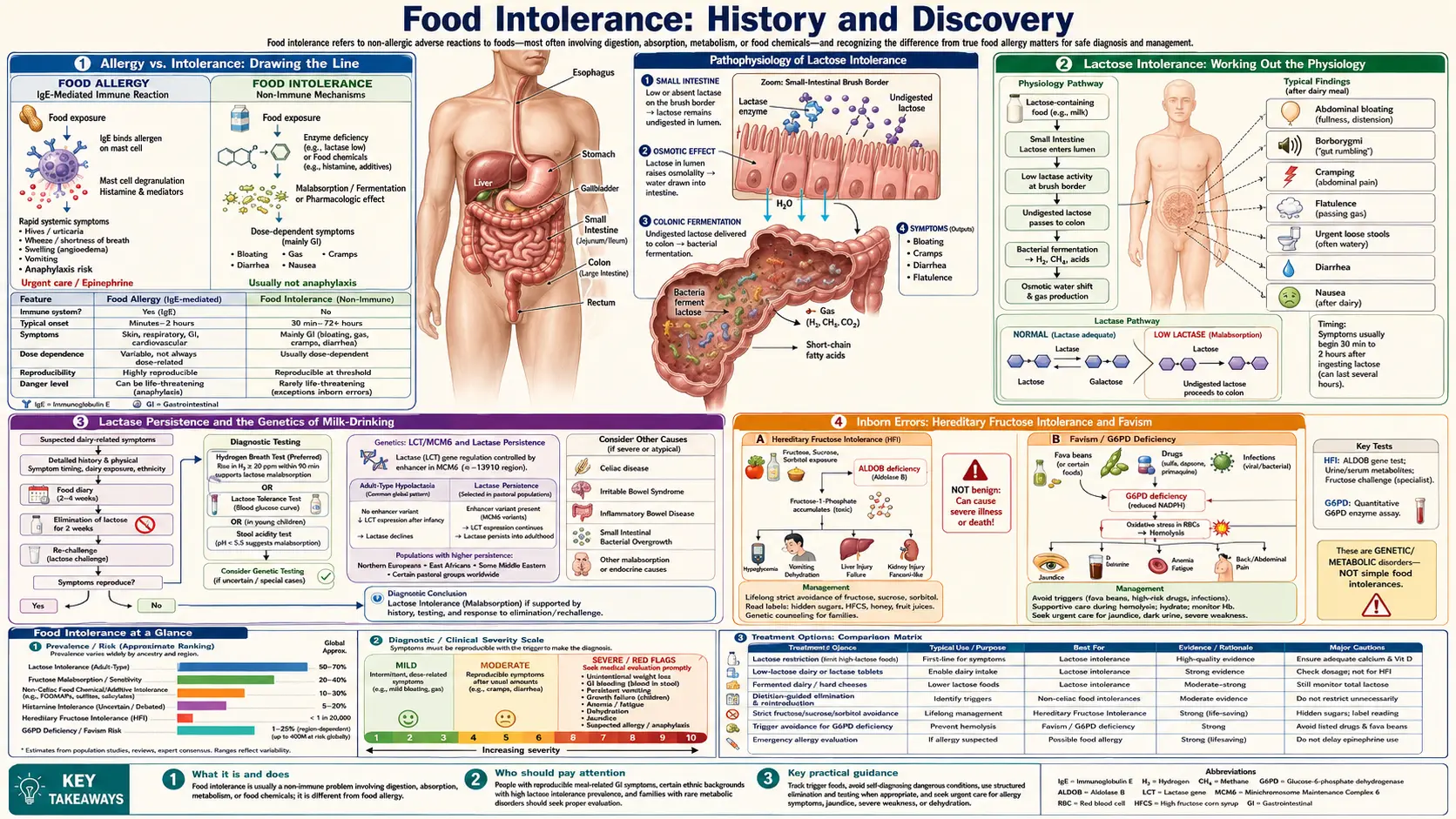
The single most important idea in the history of food intolerance is a distinction: that not every bad reaction to food involves the immune system. Today clinicians divide adverse food reactions into broad families. A true food allergy is an immune reaction — classically an IgE-antibody response — that can escalate quickly and, at worst, to life-threatening anaphylaxis. Celiac disease is a separate, autoimmune reaction to gluten that damages the small-intestinal lining. A food intolerance, by contrast, is a non-immune adverse reaction: the body cannot properly handle a food or one of its components, usually because of an enzyme deficiency, a pharmacologically active food chemical, or another non-immune mechanism. The symptoms — bloating, gas, cramping, diarrhea, headache — are real and often miserable, but the underlying machinery is digestive and biochemical, not immunological.
This vocabulary grew out of immunology. In 1906 the Viennese pediatrician Clemens von Pirquet coined the term allergy (from Greek roots meaning “altered reaction”) in the journal Münchener Medizinische Wochenschrift, building on his and Béla Schick’s study of “serum sickness” in children. It is worth noting, as historians of medicine point out, that von Pirquet’s original concept was broad — he meant any altered reactivity of the body, not only the harmful hypersensitivity reactions the word denotes today. Over the following decades the meaning narrowed to immune hypersensitivity, and that narrowing is exactly what created room for a complementary idea: reactions that look like allergy but are not immune. “Food intolerance” is, in a real sense, the non-immune counterpart that the maturing science of allergy left behind.
Why does the distinction matter so much? Because the stakes differ. A peanut allergy can kill within minutes and demands strict avoidance and emergency epinephrine; lactose intolerance, however uncomfortable, will not cause anaphylaxis, and a person may tolerate small or enzyme-assisted amounts of the food. Confusing the two leads either to dangerous complacency about real allergies or to needless, sometimes nutritionally harmful, food restriction for intolerances. Much of the modern history below is the story of medicine learning to tell these mechanisms apart — and of discovering, one by one, exactly what goes wrong in each non-immune reaction.
Lactose Intolerance: Working Out the Physiology
The textbook example of a food intolerance is the inability to digest lactose, the sugar in milk. The biochemistry is simple in outline: lactose is a disaccharide that must be split by the enzyme lactase (lactase-phlorizin hydrolase), produced in the brush border of the small intestine, into glucose and galactose before it can be absorbed. When lactase activity is low, undigested lactose passes into the colon, where gut bacteria ferment it — producing the gas, bloating, cramping, and osmotic diarrhea that define the condition. The enzyme itself was identified early: the British biochemist R. H. Plimmer is generally credited with characterizing intestinal lactase in 1906, the same year von Pirquet coined “allergy.” But understanding the enzyme was not the same as understanding the condition.
For the first half of the twentieth century, lactose intolerance was poorly understood and often misattributed. The decisive work came in the 1960s, when intestinal-biopsy techniques and new enzyme assays let researchers measure disaccharidase activity directly in living human gut tissue. In 1963, Salvatore Auricchio, Andrea Rubino, Giorgio Semenza, Andrea Prader and colleagues reported, in The Lancet, isolated lactase deficiency in adults — demonstrating that an otherwise healthy adult could simply lack lactase. Around the same time the Swedish biochemist Arne Dahlqvist developed a practical method (published 1964) for assaying intestinal disaccharidases, which made disaccharidase deficiencies measurable in routine practice. These advances reframed lactose intolerance as a definable, quantifiable enzyme deficiency rather than a vague digestive complaint.
A second conceptual shift followed: low adult lactase is the human norm, not the exception. Surveys across the 1960s and 1970s found that the majority of the world’s adults — across much of Asia, Africa, the Americas, and the Mediterranean — have lactase non-persistence (a natural decline of lactase after weaning), while continued high lactase into adulthood (lactase persistence) is concentrated in populations with a long history of dairying. That the “intolerant” majority are physiologically ordinary and the milk-drinking minority are the genetic outliers set the stage for the evolutionary genetics solved at the turn of the twenty-first century.
Lactase Persistence and the Genetics of Milk-Drinking
If most adults lose lactase, why do so many Northern Europeans, and certain African and Middle-Eastern pastoralist groups, keep it? Answering that turned lactose intolerance into one of the most celebrated case studies in human evolution. The breakthrough came in 2002, when Nabil Sahi Enattah and colleagues, working with Finnish families, published in Nature Genetics the identification of a DNA variant — designated C/T−13910, located in an intron of the neighboring MCM6 gene about 14 kilobases upstream of the lactase (LCT) gene — that associated essentially completely with lactase persistence. The “T” version acts as a regulatory switch that keeps the lactase gene switched on into adulthood; the ancestral “C” version lets it fade after weaning. For the first time, the common adult trait had a precise molecular address.
What followed showed why this discovery resonated far beyond gastroenterology. In 2004, Todd Bersaglieri and colleagues demonstrated that the lactase-persistence region bears one of the strongest signatures of recent positive natural selection anywhere in the human genome — the trait spread through certain populations with unusual speed, over roughly the last ten thousand years, a window that brackets the Neolithic domestication of dairy animals. The favored interpretation is a textbook case of gene–culture co-evolution: as people began herding and milking, those who could digest milk into adulthood gained a nutritional edge, so the persistence variant was selected for — while the availability of milk made dairying worthwhile, reinforcing the loop. Later modeling (Yuval Itan, Mark Thomas and colleagues, 2009) placed the European −13910*T variant’s rise among early Central European farmers on the order of 7,500 years ago.
Two nuances keep the story honest. First, lactase persistence evolved more than once: Sarah Tishkoff and colleagues (2007) identified different regulatory variants in East African pastoralists that independently produce the same milk-digesting trait — convergent evolution driven by the same cultural pressure. Second, the precise selective advantage (calories, fluid in arid climates, calcium and vitamin D, or avoidance of contaminated water) is still debated, and parts of the gene–culture timeline remain active research rather than settled fact. What is firmly established is the core finding: a single, identifiable regulatory variant explains most European lactase persistence, and dairying drove its spread.
Inborn Errors: Hereditary Fructose Intolerance and Favism
Lactose intolerance is common and mild; a few other food intolerances are rare, inherited, and potentially dangerous — and their discovery filled in the “enzyme deficiency” branch of the intolerance family tree. Hereditary fructose intolerance (HFI) was first described as a clinical entity in 1956 by Chambers and Pratt, who reported a young woman who became ill — nausea, abdominal pain, and low blood sugar — specifically after eating fruit or sugar, and who termed her condition an “idiosyncrasy to fructose.” A few years later (1961), Henri-Géry Hers and G. Joassin identified the underlying defect in liver tissue: a deficiency of the enzyme aldolase B, which normally processes fructose-1-phosphate. Without it, that intermediate accumulates to toxic levels, causing severe hypoglycemia and, with continued exposure, liver and kidney injury. HFI is an autosomal-recessive inborn error of metabolism — distinct from ordinary, harmless dietary fructose malabsorption — and it neatly illustrates how a single missing enzyme can make a common food poisonous to one person and harmless to everyone else.
Favism is a different and older puzzle. For centuries it was known that some people — particularly around the Mediterranean — fell acutely ill, with collapse and dark urine, after eating fava (broad) beans; the reaction is a sudden breakdown of red blood cells (hemolysis). The biochemical cause was uncovered in the 1950s. In 1956, investigators including Paul Carson in Alf Alving’s Chicago laboratory found that men who suffered hemolysis after the antimalarial drug primaquine had a deficiency of the red-cell enzyme glucose-6-phosphate dehydrogenase (G6PD). The following year (1957), Gennaro Sansone and Giuseppe Segni in Genoa showed that patients with a history of favism shared the same G6PD deficiency — tying the ancient bean reaction to the new enzyme defect. The link is oxidative stress: both fava-bean compounds and certain drugs strain red cells that, lacking G6PD, cannot defend themselves. In 1958, work by Arieh Szeinberg and colleagues helped establish that the deficiency is inherited on the X chromosome.
These “inborn” intolerances are non-immune adverse reactions to food caused by a genetic enzyme deficiency, which fits the definition of food intolerance — yet because favism produces hemolysis rather than mere digestive upset, and HFI can cause organ damage, both are far more serious than everyday lactose intolerance. Their histories matter here because they were among the first food reactions whose exact molecular mechanism was nailed down, helping establish the principle that “intolerance” is not one thing but a collection of distinct, identifiable biochemical faults.
Pharmacological Reactions: Histamine and Vasoactive Amines
A second major branch of food intolerance has nothing to do with missing digestive enzymes and everything to do with pharmacologically active chemicals naturally present in food. Certain foods contain biogenic amines — histamine, tyramine, and related compounds — that act on the body like low-dose drugs. The clearest modern concept here is histamine intolerance: the idea that some people react to histamine-rich foods (aged cheeses, cured and fermented meats, fermented vegetables, some fish, and alcohol, particularly red wine) because they cannot break dietary histamine down fast enough. Symptoms — flushing, headache, hives, nasal congestion, palpitations, digestive upset — can mimic an allergy, which is precisely why distinguishing the mechanism took careful work.
The accepted explanation centers on the enzyme diamine oxidase (DAO), produced in the intestinal lining, which normally degrades histamine arriving from food. If DAO activity is insufficient (whether from genetic factors, gut disease, or DAO-blocking drugs and alcohol), dietary histamine can build up and trigger histamine-like effects throughout the body. The concept was crystallized for the modern clinical era by a widely cited 2007 review by Laura Maintz and Natalija Novak in the American Journal of Clinical Nutrition, which framed histamine intolerance as an imbalance between histamine intake and the body’s capacity to degrade it. Related to this is tyramine sensitivity, long recognized in patients taking monoamine-oxidase-inhibitor (MAOI) antidepressants, in whom tyramine-rich aged foods can dangerously raise blood pressure — another pharmacological, non-immune food reaction.
Honesty requires a caveat the scientific literature itself stresses: histamine intolerance remains a contested, evolving concept. There is no single, universally validated diagnostic test; symptoms overlap with allergy, IBS, and other conditions; and the role of DAO measurement is still debated among specialists. It is best presented as a working hypothesis with real biochemical underpinnings — plausible, increasingly studied, and clinically useful, but not as cleanly “solved” as lactase deficiency.
Food Additives and the MSG Myth
No history of food intolerance is complete without the most famous — and most instructive — cautionary tale: monosodium glutamate (MSG) and so-called “Chinese restaurant syndrome.” The episode began with a single letter. On April 4, 1968, the New England Journal of Medicine published a short, anecdotal letter from Dr. Robert Ho Man Kwok, who described feeling numbness, weakness, and palpitations after eating at Chinese restaurants in the United States and speculated about possible causes — cooking wine, sodium, or MSG — while explicitly noting he had no scientific evidence. The journal ran it under the heading “Chinese Restaurant Syndrome,” and the label stuck for decades, fixing public suspicion on MSG and, unfairly, on a cuisine.
What makes this history valuable is the gap between the scare and the science. Despite many subsequent studies — including double-blind, placebo-controlled challenges — researchers were largely unable to reliably reproduce a consistent set of symptoms attributable to MSG in the general population at normal dietary doses. Monosodium glutamate has held “Generally Recognized As Safe” (GRAS) status with the U.S. Food and Drug Administration for decades, and major food-safety reviews have not supported the original alarm. Historians and scientists now widely regard “Chinese restaurant syndrome” as largely debunked and culturally overstated — a case where an unverified anecdote, confirmation bias, and the prejudices of the era combined to manufacture a food scare that outran the evidence. (A small minority of people may report transient, mild, self-limited symptoms after very large doses, but this is far from the sweeping syndrome originally claimed.)
Other additive reactions are better substantiated, and the contrast is instructive. Sulfites — preservatives used in some dried fruits, wine, and processed foods — can provoke genuine adverse reactions, including wheezing in a subset of people with asthma, which is why sulfite labeling above a threshold is mandated in many countries. The broader lesson of the additives chapter is methodological: the only reliable way to separate a real food intolerance from coincidence or expectation is the double-blind, placebo-controlled food challenge, in which neither patient nor observer knows whether the suspect substance or a dummy was given — a standard that emerged partly in response to the MSG controversy.
The FODMAP Concept and Modern IBS Diets
The most consequential recent chapter in food-intolerance science reframed a whole cluster of vague “sensitivities” into a single, testable idea: the FODMAP concept. FODMAP stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols — a family of short-chain carbohydrates (found in wheat, onions, garlic, legumes, certain fruits, some sweeteners, and, via lactose, dairy) that are poorly absorbed in the small intestine. Because they are osmotically active and rapidly fermented by gut bacteria, they draw water into the bowel and generate gas, producing the bloating, distension, pain, and altered bowel habits that plague many people with irritable bowel syndrome (IBS). The insight was to recognize these scattered carbohydrates as one mechanistic group and to manage them together.
The concept came from a research team at Monash University in Melbourne, Australia, led by gastroenterologist Peter Gibson with dietitian Sue (Susan) Shepherd, along with Jane Muir and colleagues. The group settled on the FODMAP term in 2004 and first published the hypothesis in 2005, proposing that collectively reducing these poorly absorbed carbohydrates would reduce the gas and water that drive IBS symptoms. Over the following years the Monash team built the evidence base — controlled trials, a systematic food-composition database measuring FODMAP content, and a structured three-phase “low-FODMAP diet” (strict restriction, methodical reintroduction, then personalization). Gibson’s own 2017 retrospective, History of the low FODMAP diet, recounts this development from the inside.
The FODMAP story matters for two reasons. First, it models how a fuzzy complaint — “something in my diet upsets my gut” — can be converted into a defined, mechanism-based, rigorously tested dietary therapy now recommended in IBS guidelines worldwide. Second, it underscores a recurring theme of this page: many food intolerances are about dose and mechanism, not all-or-nothing avoidance. The low-FODMAP approach is deliberately a temporary diagnostic-and-therapeutic tool followed by reintroduction, not a permanent ban — an evidence-based descendant of the much older, cruder observation that certain foods simply do not agree with certain people.
A Modern, Mechanism-Based Map
Seen from the present, the history of food intolerance is the gradual replacement of one vague category — “food that disagrees with you” — with a precise map of distinct mechanisms. On one side sit the immune reactions: IgE-mediated food allergy (including unusual forms such as alpha-gal syndrome, the tick-bite–triggered red-meat allergy) and the autoimmune reaction of celiac disease. On the other side sit the non-immune intolerances: enzyme deficiencies (lactose intolerance, hereditary fructose intolerance), red-cell enzyme reactions (favism/G6PD), pharmacological reactions to food chemicals (histamine, tyramine), additive reactions (sulfites; the largely debunked MSG scare), and carbohydrate malabsorption captured by the FODMAP framework, which overlaps heavily with irritable bowel syndrome.
Each branch corresponds to a real discovery: von Pirquet’s 1906 coining of “allergy” that created the immune/non-immune divide; the 1960s enzyme assays that made lactase deficiency measurable; the 2002 identification of the lactase-persistence variant and the gene–culture story behind it; the mid-century unraveling of HFI and favism; the framing of histamine intolerance in the 2000s; and the 2004–2005 birth of the FODMAP concept. Running through all of them is the same methodological backbone — controlled food challenges and biochemical testing — that lets science separate genuine intolerance from coincidence, expectation, or fashion.
For the reader, the practical takeaway of this history is also its main caution. “Food intolerance” is not a single diagnosis and not a license for sweeping elimination diets sold on the strength of unvalidated tests; it is a set of specific, identifiable conditions, each with its own mechanism, test, and sensible management. Suspected reactions deserve proper evaluation — to confirm what is real, to rule out a dangerous true allergy or celiac disease, and to avoid the nutritional harm of cutting out foods that are, for that individual, perfectly fine.
Research Papers and References
The list below combines landmark peer-reviewed papers (with real DOIs or PMIDs where attribution is firm) and curated PubMed topic-search links into the historical and mechanistic literature on food intolerance. Where a fact in this article is a working hypothesis or an area of ongoing debate — notably histamine intolerance and parts of the lactase-persistence timeline — it is presented as such in the text above. Each link opens in a new tab.
- Enattah NS, Sahi T, Savilahti E, Terwilliger JD, Peltonen L, Järvelä I. Identification of a variant associated with adult-type hypolactasia. Nature Genetics. 2002;30(2):233-237. — doi:10.1038/ng826
- Bersaglieri T, Sabeti PC, Patterson N, et al. Genetic signatures of strong recent positive selection at the lactase gene. American Journal of Human Genetics. 2004;74(6):1111-1120. — doi:10.1086/421051
- Tishkoff SA, Reed FA, Ranciaro A, et al. Convergent adaptation of human lactase persistence in Africa and Europe. Nature Genetics. 2007;39(1):31-40. — doi:10.1038/ng1946
- Itan Y, Powell A, Beaumont MA, Burger J, Thomas MG. The origins of lactase persistence in Europe. PLoS Computational Biology. 2009;5(8):e1000491. — doi:10.1371/journal.pcbi.1000491
- Maintz L, Novak N. Histamine and histamine intolerance. American Journal of Clinical Nutrition. 2007;85(5):1185-1196. — doi:10.1093/ajcn/85.5.1185
- Gibson PR. History of the low FODMAP diet. Journal of Gastroenterology and Hepatology. 2017;32(Suppl 1):5-7. — doi:10.1111/jgh.13685 ( — Search PubMed)
- Auricchio S, Rubino A, Prader A, et al. Isolated intestinal lactase deficiency in the adult (The Lancet, 1963) PubMed: isolated adult lactase deficiency (1963)
- von Pirquet C — the coining of the term “allergy” (1906) and the history of the allergy concept PubMed: von Pirquet and the history of allergy
- Chambers RA, Pratt RTC — idiosyncrasy to fructose / first description of hereditary fructose intolerance (1956), and aldolase B deficiency PubMed: hereditary fructose intolerance history
- Glucose-6-phosphate dehydrogenase (G6PD) deficiency and favism — discovery and historical perspective (Carson; Sansone & Segni) PubMed: G6PD deficiency and favism history
- “Chinese restaurant syndrome,” monosodium glutamate and the history of the MSG food scare PubMed: MSG symptom complex / Chinese restaurant syndrome
- Lactose intolerance, lactase non-persistence and lactase persistence — physiology, genetics and evolution (reviews) PubMed: lactase persistence genetics and evolution
- FODMAPs, fructose malabsorption and the low-FODMAP diet in irritable bowel syndrome PubMed: FODMAPs and irritable bowel syndrome
- Definitions and classification of adverse food reactions: food allergy vs. food intolerance vs. celiac disease PubMed: classification of adverse food reactions
External Authoritative Resources
- NIDDK (NIH) — Lactose Intolerance
- MedlinePlus — Food Allergy and Intolerance
- PubMed — Food intolerance (non-immune adverse food reactions)
Connections
- Pain & Allergy
- Food Intolerance (Overview)
- Allergies
- Alpha-Gal Syndrome
- Celiac Disease
- Irritable Bowel Syndrome
- All Conditions