Allergies: History and Discovery
The story of allergy is the story of a single, strange idea slowly coming into focus: that the very immune system meant to protect us can turn against harmless things — pollen, peanuts, cat dander — and injure or even kill the person it is supposed to defend. Ancient writers noticed odd reactions to foods and stings, but the modern science is barely two centuries old. It runs from John Bostock describing his own summer misery in 1819, through Charles Blackley proving pollen was the culprit in 1873, to Charles Richet and Paul Portier naming the deadly reaction “anaphylaxis” in 1902, to Clemens von Pirquet coining the word “allergy” itself in 1906. The molecular key — the antibody immunoglobulin E (IgE) — was not found until 1966. This page traces that arc, and is careful throughout to separate what is documented from what is merely legend.
Table of Contents
- Allergy in Antiquity: Observation and Legend
- John Bostock and the First Description of Hay Fever (1819)
- Charles Blackley Proves Pollen Is the Cause (1873)
- Richet, Portier and the Discovery of Anaphylaxis (1902)
- Clemens von Pirquet Coins the Word “Allergy” (1906)
- Histamine and the First Antihistamines
- The Discovery of IgE: The Antibody Behind Allergy (1966)
- The Modern Allergy Epidemic and the Hygiene Hypothesis
- From Discovery to Modern Care
- Research Papers and References
- Connections
- Featured Videos
Allergy in Antiquity: Observation and Legend
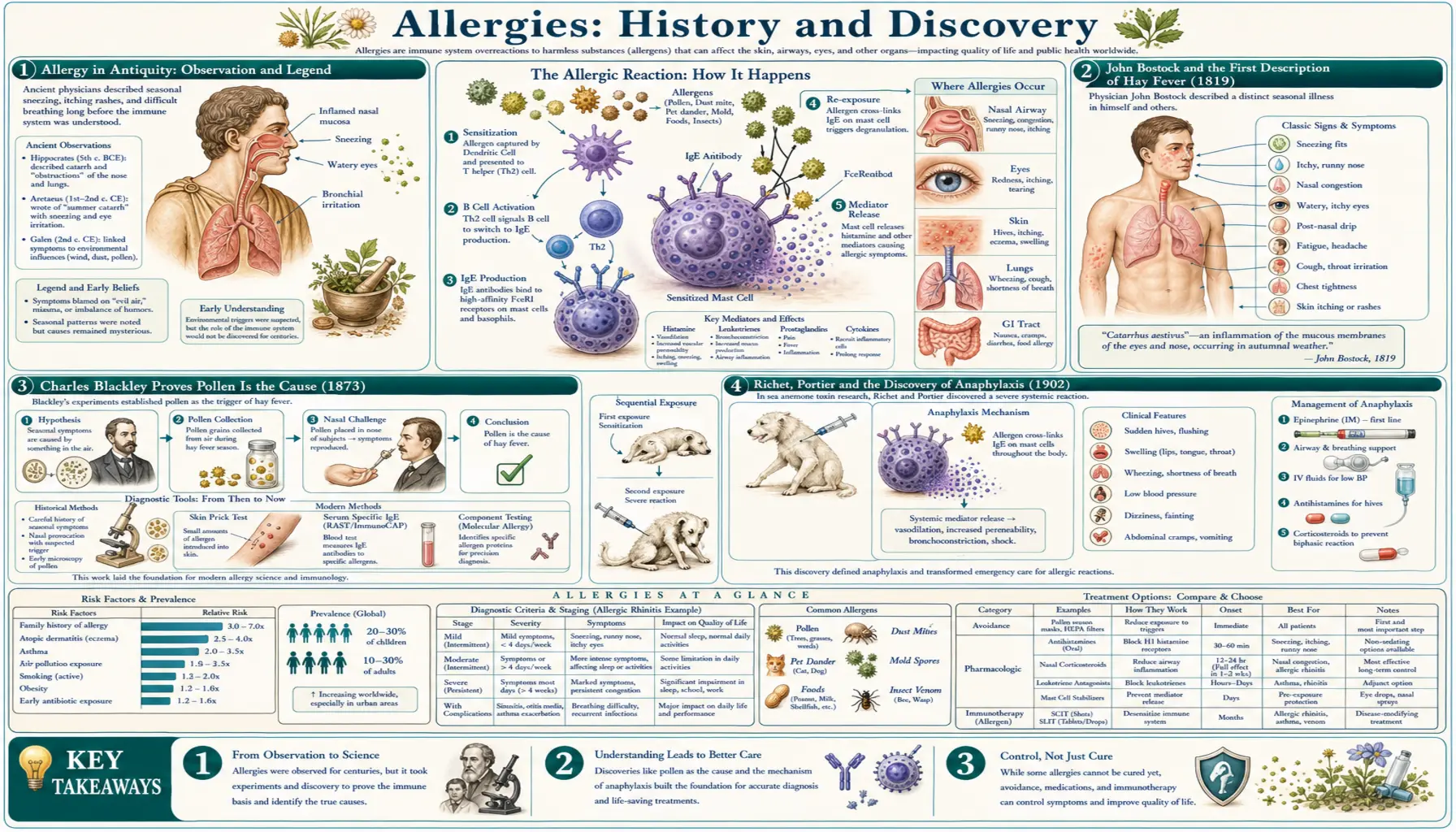
People have suffered allergic reactions for as long as there have been people, even though no one understood what was happening. Ancient Greek and Roman physicians recorded that some individuals fell ill from foods that nourished everyone else, and that certain people reacted violently to insect stings. The Roman philosopher and poet Lucretius captured the idea in a famous line usually rendered as “what is food to one may be fierce poison to others” — a striking, if accidental, glimpse of the central truth of allergy: that the danger lies not in the substance but in the individual’s reaction to it.
The most colorful ancient claim concerns Menes, traditionally counted as the first pharaoh of a unified Egypt. A widely repeated story holds that he died from the sting of a wasp or hornet, supposedly recorded on small ebony tomb plates whose hieroglyphs were read as a stinging insect — which would make it the earliest reported death from anaphylaxis. This should be treated as legend, not history. Scholars have traced the tale to a single nineteenth-century source and shown it to be essentially fiction; worse, the relevant Egyptian word for “wasp” closely resembles the word for “hippopotamus,” so the plates may not describe a sting at all. A 2004 paper in the journal Allergy bluntly called Menes’ death-by-wasp “the end of a myth.” It makes a wonderful story, but the science of allergy does not rest on it.
What antiquity genuinely contributed was observation without explanation. Physicians could see that reactions were real, sudden, and specific to particular people, but they had no framework to make sense of them. For nearly two thousand years allergy remained a collection of curious anecdotes. The scientific story proper does not begin until a London physician decided, in 1819, to describe his own annual torment in clinical detail.
John Bostock and the First Description of Hay Fever (1819)
On 16 March 1819 the English physician John Bostock stood before the Medical and Chirurgical Society of London and read a paper titled “Case of a periodical affection of the eyes and chest.” It is generally regarded as the first clear clinical description of what we now call hay fever. The patient in the report, identified only as “J.B., aged 46,” was Bostock himself. Every summer since the age of about eight he had endured fierce bouts of sneezing, streaming inflamed eyes, a running nose, and tightness of the chest — a pattern so regular it returned with the season like clockwork.
Bostock searched for the trigger and, fascinatingly, got the cause wrong while describing the disease exactly right. Because his symptoms peaked in early summer, he suspected the heat and the sun, and the popular notion of the day blamed the scent and dust of new-mown hay — which is how the enduring, if misleading, name “hay fever” arose. (The hay itself is innocent; the real culprit is grass pollen, which happens to peak at haymaking time.) Over the next nine years Bostock gathered about two dozen similar cases and, in a second paper in 1828, gave the condition the formal Latin name catarrhus aestivus — “summer catarrh.”
Two points deserve emphasis for accuracy. First, Bostock described hay fever; he did not discover its cause — that came half a century later. Second, the now-famous term catarrhus aestivus belongs to his 1828 follow-up, not the original 1819 reading. What Bostock achieved was to lift hay fever out of folklore and place it on the medical record as a distinct, repeatable, describable disease — the necessary first step before anyone could ask why it happened.
Charles Blackley Proves Pollen Is the Cause (1873)
The man who finally answered the “why” was Charles Harrison Blackley, a Manchester physician and himself a lifelong hay-fever sufferer. In his 1873 book Experimental Researches on the Causes and Nature of Catarrhus aestivus (Hay-fever or Hay-asthma) he established, through painstaking self-experimentation, that the true cause of hay fever is the inhalation of pollen — not heat, not sunlight, and not the smell of hay. It was a landmark of careful, patient science, the product of some fourteen years of work.
Blackley’s methods were ingenious and remarkably modern. To prove pollen was the agent, he deliberately applied it to his own body and watched the reaction. In one experiment he placed pollen on a small scratch on his skin and saw an itchy weal rise within about twenty minutes — an exercise now recognized as essentially the first allergy skin-prick test, the direct ancestor of the diagnostic test still used in clinics today. He confirmed that pollen applied to the eyes and nose reproduced his symptoms, while sealing pollen away relieved them. To measure how much pollen was actually in the air, he coated glass slides with a sticky surface, exposed them on timers, and even flew them on kites up to around 1,500–2,000 feet to sample pollen high in the atmosphere — pioneering the science of aerobiology and pollen counting.
The work was respected enough that Charles Darwin wrote to thank Blackley for his book. With Blackley, the chain was complete in principle: a specific, identifiable substance from the outside world (pollen) entered a susceptible person and produced a specific, reproducible illness. What was still missing was an explanation of the violent, sometimes fatal end of the spectrum — and that discovery came, unexpectedly, from an experiment that had nothing to do with hay fever at all.
Richet, Portier and the Discovery of Anaphylaxis (1902)
In 1901 the French physiologist Charles Richet and his colleague Paul Portier joined an oceanographic cruise hosted by Albert I, Prince of Monaco. Studying the venom of jellyfish and sea anemones, they set out to immunize dogs against the toxin — expecting, as the theory of the day predicted, that a small first dose would protect the animal against a later one. What they found was the opposite, and it astonished them. A dog that had survived a harmless first injection, given a tiny second dose weeks later, collapsed within minutes and died. Far from being protected, the animal had been made catastrophically, lethally over-sensitive.
Richet and Portier published this result in 1902 and gave the phenomenon a name. Reaching for the Greek, they coined “anaphylaxis” — built from ana- (against, or the reverse of) and phylaxis (protection) — literally “against protection,” the exact inverse of the immunity they had been trying to create. The word named, for the first time, the deadly end of the hypersensitivity spectrum: the whole-body allergic catastrophe that can follow a bee sting, a dose of penicillin, or a bite of peanut.
For this discovery Charles Richet was awarded the Nobel Prize in Physiology or Medicine in 1913. To be historically precise, the prize went to Richet alone; Paul Portier, his equal partner in the original experiments, was not named in the award, though by all accounts he bore no resentment and the two remained on good terms. Anaphylaxis gave clinicians a concept — and a word — for sudden, severe, systemic allergic collapse, and it set the stage for a broader term that could embrace the whole range of these altered reactions, from a sneeze to a fatal shock.
Clemens von Pirquet Coins the Word “Allergy” (1906)
That broader word was supplied in 1906 by the Viennese pediatrician Clemens von Pirquet. Working with serum therapy — treating diseases like diphtheria by injecting horse-derived antiserum — he and his colleague Béla Schick noticed something important: patients who received a second dose of horse serum or smallpox vaccine often reacted faster and more severely than to the first. The body, von Pirquet realized, was not simply “immune” or “not immune.” Prior exposure could change its reactivity in either direction — toward protection (true immunity) or toward harmful over-reaction.
To capture this neutral idea of changed reactivity, von Pirquet coined the term “allergy”, introducing it in the Münchener Medizinische Wochenschrift in 1906. He built it from two Greek roots: allos, meaning “other” or “changed,” and ergon, meaning “work,” “action,” or “reaction.” Allergy therefore meant, literally, an “altered reaction” or a “changed capacity to react.” In its original sense the word was deliberately broad, covering any altered immune responsiveness; only over the following decades did everyday usage narrow it to the harmful hypersensitivity reactions — hay fever, asthma, hives, food and drug reactions — that we mean by “allergy” today.
It is worth pausing on what von Pirquet did and did not do. He coined the word and articulated the concept of altered reactivity; he did not identify the antibody or the cellular machinery behind it, which were still sixty years from discovery. But by giving the phenomenon a single, flexible name, he created the conceptual home into which every later finding — histamine, IgE, mast cells — could be placed. The discipline of allergology, and indeed this very page, descends from that 1906 coinage.
Histamine and the First Antihistamines
Knowing that allergy existed was one thing; understanding the chemical that causes its symptoms was another. That chemical is histamine, and the central figure in its story is the British physiologist Sir Henry Dale. In the years around 1910, working with George Barger and others, Dale isolated and studied histamine and demonstrated that injecting it produced a dramatic, shock-like state strikingly similar to anaphylaxis — falling blood pressure, constricted airways, leaking blood vessels. Over the following two decades this pointed toward a powerful conclusion: histamine, released by the body’s own cells during an allergic reaction, is responsible for much of the sneezing, itching, swelling, and wheezing that sufferers feel. (Dale received the Nobel Prize in 1936, shared with Otto Loewi, for separate work on the chemical transmission of nerve impulses — an honor often mentioned alongside his name, though it was not awarded for histamine itself.)
If histamine drives the symptoms, then a drug that blocks histamine should relieve them — and that is exactly the logic the Swiss-born Italian pharmacologist Daniel Bovet pursued at the Pasteur Institute in Paris. In 1937 Bovet and his assistant Anne-Marie Staub identified the first compound that could counter histamine’s effects, a substance called piperoxan — the first antihistamine. These earliest compounds were too toxic for everyday use; the first antihistamine practical enough to give to patients, phenbenzamine, followed in 1942, opening the door to the antihistamine medicines that millions now take for hay fever and hives.
For this body of work — synthetic compounds that block the action of substances like histamine in the body — Daniel Bovet was awarded the Nobel Prize in Physiology or Medicine in 1957. The histamine story is a clean example of allergy science maturing from observation into treatment: identify the offending chemical, then design a drug to oppose it. Yet one deep question still had no answer. What, exactly, decided that this person’s immune system would release histamine at the touch of pollen while the next person’s ignored it entirely? The answer lay in an antibody no one had yet found.
The Discovery of IgE: The Antibody Behind Allergy (1966)
For decades immunologists knew that allergy could be transferred from an allergic person to a non-allergic one through the blood, implying that some specific factor in serum carried the sensitivity. They called this mysterious agent “reagin,” but no one could identify it — it did not match any of the known classes of antibody. The hunt for reagin was the great unfinished business of allergy science, and it was finished, almost simultaneously, by two teams working an ocean apart.
In 1966, the husband-and-wife immunologists Kimishige Ishizaka and Teruko Ishizaka, working at the Children’s Asthma Research Institute and Hospital in Denver, Colorado, demonstrated that the elusive reagin was in fact a previously unrecognized class of antibody. Independently and at nearly the same time, Gunnar Johansson and Hans Bennich in Uppsala, Sweden, were characterizing an unusual myeloma protein that fit none of the four known antibody classes. The two efforts converged on the same molecule, and in 1968 the World Health Organization formally recognized it as a fifth class of immunoglobulin, named immunoglobulin E (IgE); the groups published a joint paper in 1969. This was the missing piece — the actual antibody that, by coating cells called mast cells and basophils and triggering them to release histamine on contact with an allergen, makes an allergic person allergic.
The discovery of IgE transformed allergy from a description into a mechanism. It explained why allergy can be transferred in serum (the IgE travels with it), why skin tests work (injected allergen finds skin-bound IgE and fires the mast cells), and why some people are atopic while others are not (they make IgE against everyday proteins that most people tolerate). It is the foundation of modern allergy diagnosis — the blood tests that measure allergen-specific IgE — and of the newest treatments, including anti-IgE biologic drugs that mop up the antibody before it can do harm. Credit is properly shared: the Ishizakas and the Johansson–Bennich group reached the same destination by different roads, and the honest history names all four.
The Modern Allergy Epidemic and the Hygiene Hypothesis
The final chapter of the story is not a single discovery but a sweeping change in the world the immune system lives in. Across the industrialized West, rates of hay fever, asthma, eczema, and food allergy climbed steeply through the late twentieth century and into the twenty-first — far too fast to be explained by changes in our genes. Something in the modern environment was making more and more people allergic, and explaining that rise became one of the great puzzles of allergy science.
A pivotal clue arrived in 1989, when the British epidemiologist David Strachan published a short paper in the BMJ titled “Hay fever, hygiene, and household size.” Analyzing more than 17,000 British children, he found that those with more older siblings were less likely to develop hay fever and eczema. He proposed that infections passed between young siblings in early life might somehow protect against allergy, and that smaller families and cleaner homes meant fewer such exposures. This idea grew into what is now called the hygiene hypothesis — the proposal that reduced microbial exposure in early childhood leaves the immune system more prone to allergic over-reaction. (Worth noting for accuracy: Strachan’s 1989 paper did not itself use the phrase “hygiene hypothesis”; the name was attached later as the idea spread.)
It is important to be clear that the hygiene hypothesis remains a hypothesis, not settled fact. The original observation — fewer allergies in larger families — has been confirmed many times, but the explanation has been debated, refined, and partly revised. Researchers today often favor broader versions, such as the “old friends” or microbiome framework, which emphasize the diversity of the microbes we co-evolved with (in soil, on farms, in the gut) rather than simple cleanliness. Whatever the precise mechanism, the era’s central lesson is that allergy is shaped by environment and lifestyle, not genes alone — which is why the modern surge is best understood as a mismatch between an ancient immune system and a very new way of living.
From Discovery to Modern Care
Set end to end, the history of allergy is a relay across two centuries. Bostock (1819) named the disease; Blackley (1873) found the cause and invented the skin test; Richet and Portier (1902) revealed and named anaphylaxis; von Pirquet (1906) gave the whole field its word; Dale and Bovet supplied the chemistry of histamine and the first drugs to block it; the Ishizakas and Johansson and Bennich (1966) at last identified IgE, the antibody at the center of it all; and Strachan (1989) reframed the modern epidemic as a problem of environment. Each step built on the last, and each was the patient work of people who often experimented on themselves.
That long chain of discovery is exactly what stands behind today’s ordinary allergy care. The skin-prick test descends directly from Blackley’s scratch; the specific-IgE blood test descends from the Ishizakas’ antibody; over-the-counter antihistamines descend from Bovet’s piperoxan; the life-saving epinephrine auto-injector exists because Richet showed how fast anaphylaxis can kill. Even allergen immunotherapy — the allergy shots and tablets that retrain the immune system — and the newest anti-IgE biologic medicines are the direct descendants of these foundational insights, now turned into tools that genuinely change lives.
For the day-to-day reality of living with these conditions — recognizing triggers, getting tested, managing symptoms, and acting fast in an emergency — see the main Allergies page and the related condition pages linked below. History explains how we came to understand allergy; those pages explain what to do about it.
Research Papers and References
The references below trace the documented milestones in the history of allergy — Bostock’s 1819 description, Blackley’s 1873 pollen experiments, the 1902 discovery of anaphylaxis, von Pirquet’s 1906 coinage of “allergy,” the histamine and antihistamine work, the 1966 discovery of IgE, and the 1989 hygiene-hypothesis paper. Where a stable DOI or PubMed/PMC record exists it is linked directly; otherwise a curated PubMed topic search is provided. Each link opens in a new tab.
- Ring J. Allergy in Practice — historical overview of allergy from antiquity to the present. PubMed topic search — PubMed: history of allergy
- Bostock J. Case of a periodical affection of the eyes and chest (1819); “Of the catarrhus aestivus, or summer catarrh” (1828) — the first descriptions of hay fever. Historical commentary — PMC: John Bostock’s first description of hay fever
- Blackley CH. Experimental Researches on the Causes and Nature of Catarrhus aestivus (Hay-fever or Hay-asthma). London, 1873 — pollen as the cause; the first skin test. PubMed topic search — PubMed: Blackley pollen hay fever
- Cohen SG, Zelaya-Quesada M. Portier, Richet, and the discovery of anaphylaxis: a centennial. J Allergy Clin Immunol. 2002;110(2):331-336. — doi:10.1067/mai.2002.126843
- The Nobel Prize in Physiology or Medicine 1913 — Charles Richet, “in recognition of his work on anaphylaxis.” NobelPrize.org: Richet 1913
- von Pirquet C. Allergie. Münchener Medizinische Wochenschrift. 1906;53:1457-1458 — the coinage of “allergy.” Centennial commentary — PubMed: 100 years of allergy — von Pirquet
- Igea JM. The history of the idea of allergy. Allergy. 2013;68(8):966-973. — doi:10.1111/all.12174
- Krombach JW, Kampe S, Keller CA, Wright PM. Pharaoh Menes’ death after an anaphylactic reaction — the end of a myth. Allergy. 2004;59(11):1234-1235. — doi:10.1111/j.1398-9995.2004.00603.x
- Tiligada E, Ennis M. Histamine pharmacology: from Sir Henry Dale to the 21st century. Br J Pharmacol. 2020;177(3):469-489. — doi:10.1111/bph.14524
- The Nobel Prize in Physiology or Medicine 1957 — Daniel Bovet, for synthetic compounds that inhibit substances such as histamine. NobelPrize.org: Bovet 1957
- Ishizaka K, Ishizaka T. Identification of γE-antibodies as a carrier of reaginic activity (1966) — the discovery of IgE. Historical review — PubMed: discovery of IgE
- Johansson SGO, Bennich H. Immunological studies of an atypical (myeloma) immunoglobulin (1967) — independent characterization of IgE. PubMed topic search — PubMed: Johansson Bennich IgE
- Strachan DP. Hay fever, hygiene, and household size. BMJ. 1989;299(6710):1259-1260. — doi:10.1136/bmj.299.6710.1259
- Stiemsma LT, Reynolds LA, Turvey SE, Finlay BB. The hygiene hypothesis: current perspectives and future therapies. Immunotargets Ther. 2015;4:143-157. — doi:10.2147/ITT.S61528
External Authoritative Resources
- NIAID (NIH) — Allergic Diseases
- American Academy of Allergy, Asthma & Immunology (AAAAI)
- NobelPrize.org — 1913 Prize for the work on anaphylaxis