Central Retinal Artery Occlusion
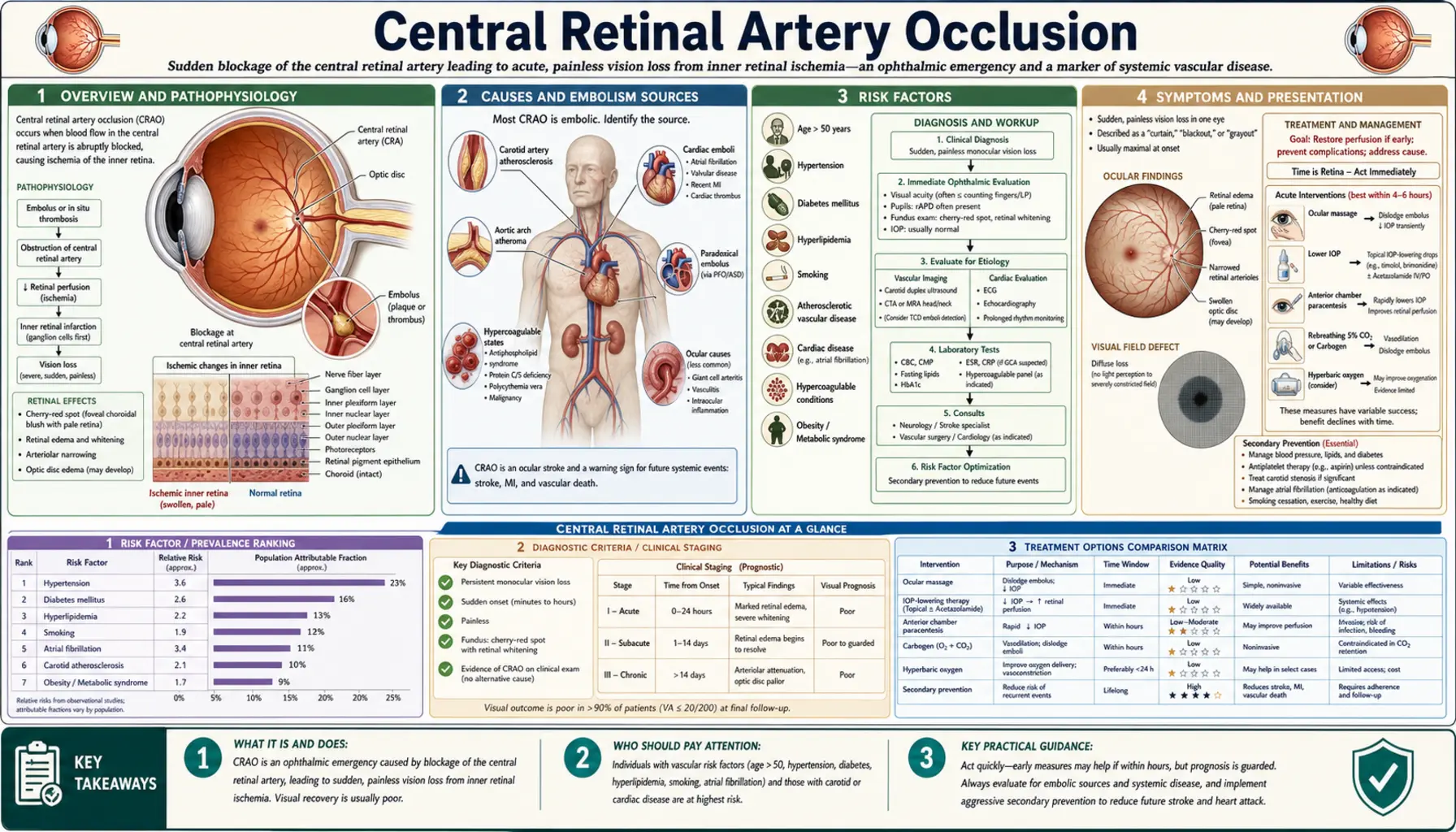
Central retinal artery occlusion (CRAO) is a sudden blockage of the central retinal artery — the main blood supply to the inner retina — causing acute, painless, and often severe monocular vision loss. It is the ocular equivalent of an ischemic stroke: rapid intervention is essential because inner retinal neurons begin dying within minutes, and most damage becomes irreversible beyond 90–100 minutes of ischemia. CRAO is also a powerful indicator of underlying systemic vascular disease; concurrent ischemic stroke occurs in up to 25–30% of patients.
Table of Contents
- Overview and Pathophysiology
- Causes and Embolism Sources
- Risk Factors
- Symptoms and Presentation
- Fundus Findings
- Diagnosis and Workup
- Emergency Treatment
- Secondary Prevention
- Prognosis and Outcomes
- Special Populations
- Key Research Papers
- Connections
- Featured Videos
Overview and Pathophysiology
The central retinal artery is a branch of the ophthalmic artery, itself a branch of the internal carotid artery. It enters the eye at the optic disc and divides into superior and inferior branches, each with nasal and temporal sub-branches, supplying the inner two-thirds of the retina — the ganglion cell layer, nerve fiber layer, inner plexiform layer, inner nuclear layer, and inner portion of the outer plexiform layer. The outer retina (photoreceptors) receives oxygen and nutrients from the choroidal circulation through diffusion across the retinal pigment epithelium.
When the central retinal artery is blocked, inner retinal ischemia begins immediately. Experimental primate data established the timeline that guides clinical management: retinal ischemia of 97 minutes or less can be reversible; beyond that threshold, damage becomes permanent. In practice, the critical treatment window is generally considered to be within 4–6 hours of symptom onset, though some benefit may extend to 24 hours. Because there is no pain and vision loss may be gradual in partial occlusions, patients often delay presentation — emphasizing the need for public education about sudden vision loss as a stroke-equivalent emergency.
CRAO accounts for approximately 1 in 10,000 outpatient ophthalmology visits and has an estimated annual incidence of about 1–2 per 100,000 population. The mean age at presentation is the mid-60s, consistent with its strong association with systemic atherosclerosis. Men are affected slightly more than women.
Causes and Embolism Sources
Embolic occlusion is the most common mechanism, identified in approximately 60–70% of CRAO cases. Embolism sources include:
- Carotid atherosclerosis: The most frequent source. Cholesterol (Hollenhorst) plaques appear as bright, refractile, yellow-orange crystals at arterial bifurcations on fundoscopy. Significant carotid stenosis (≥50%) is found in 20–45% of CRAO patients. Fibrin-platelet emboli from carotid plaques are more thrombogenic and less visible than cholesterol crystals.
- Cardiac sources: Atrial fibrillation, valvular disease (rheumatic mitral stenosis, prosthetic valves, infective endocarditis), left atrial myxoma, mural thrombus after myocardial infarction, patent foramen ovale (paradoxical embolism in younger patients), and cardiomyopathy.
- In-situ thrombosis: Local arterial wall disease, hypercoagulable states, vasculitis (giant cell arteritis is a critical cause in patients older than 50), and severe hypotension or circulatory failure.
- Coagulation disorders (especially in young patients): Factor V Leiden mutation, antiphospholipid antibody syndrome (lupus anticoagulant, anticardiolipin antibodies), protein C or protein S deficiency, antithrombin III deficiency, hyperhomocysteinemia.
- Vasospasm: Rare mechanism; associated with migraine, cocaine, and ergot alkaloids. More common in branch retinal artery occlusion.
- Calcific embolism: From degenerative aortic or mitral valve calcification; appear as chalky white plugs, usually immobile, often at the disc.
In 20–25% of cases the cause remains cryptogenic even after thorough evaluation, particularly in younger patients. Emerging evidence implicates occult paroxysmal atrial fibrillation and subclinical carotid disease detected only by advanced imaging.
Risk Factors
CRAO shares the same cardiovascular risk factor profile as ischemic stroke and myocardial infarction:
- Hypertension: Present in 65–75% of CRAO patients; the single most prevalent risk factor.
- Dyslipidemia: Atherosclerosis-driven emboli correlate with elevated LDL and low HDL.
- Diabetes mellitus: Accelerates atherosclerosis and promotes platelet aggregation.
- Smoking: Potentiates endothelial damage, platelet aggregation, and atherosclerosis progression.
- Atrial fibrillation: Present in 10–25% of CRAO; the primary preventable cause of cardiac embolism.
- Prior stroke or TIA: Signals shared vascular risk; CRAO patients have a 10–15% risk of subsequent stroke within 1 year without intervention.
- Giant cell arteritis (GCA): In patients older than 50, GCA must always be excluded; it is the most important arteritic cause of CRAO and is treatable. ESR and CRP are screening tests; temporal artery biopsy is definitive.
- Increased intraocular pressure (IOP): Glaucoma or acute angle-closure crisis can reduce perfusion pressure, precipitating occlusion in the presence of systemic vascular disease.
- Obstructive sleep apnea: Associated with nocturnal hypoxemia and increased platelet aggregability; increasingly recognized as an independent risk factor for retinal vascular occlusion.
Symptoms and Presentation
The hallmark presentation is sudden, painless, profound monocular vision loss. Key features that distinguish CRAO from other causes of acute vision loss:
- Onset: Instantaneous or within seconds; patients often describe waking with the vision loss or noticing it when closing the fellow eye.
- Severity: Vision is typically reduced to counting fingers (CF), hand motion (HM), or light perception (LP) at presentation. Initial visual acuity is 20/400 or worse in approximately 90% of patients.
- Painlessness: The absence of pain is an important diagnostic feature distinguishing CRAO from acute angle-closure glaucoma (painful) and vitreous hemorrhage (floaters, no pain). Giant cell arteritis-associated CRAO may present with headache, jaw claudication, scalp tenderness.
- Intermittent visual loss (amaurosis fugax): Transient monocular visual obscuration lasting seconds to minutes, resolving completely — a preceding warning sign in 12–15% of CRAO patients, analogous to a TIA before stroke.
- Relative afferent pupillary defect (RAPD): Present on examination; a bright light swung to the affected eye produces paradoxical dilation rather than constriction, reflecting reduced afferent input from the ischemic retina.
Fundus Findings
Dilated fundoscopic examination reveals a constellation of findings that are highly characteristic of CRAO:
- Pale, opaque, white retina: The posterior pole develops a diffuse whitish opacity within 30–60 minutes of occlusion, caused by intracellular edema in the ischemic inner retinal layers (ganglion cell layer and nerve fiber layer). The opacity is most prominent in the thickest areas of the inner retina — the arcades and posterior pole — and extends to the periphery in complete CRAO.
- Cherry-red spot at the fovea (pathognomonic): The foveal avascular zone receives nutrition directly from the underlying choroidal circulation through Bruch's membrane and the retinal pigment epithelium. Because the fovea is devoid of inner retinal layers, it remains transparent, allowing the choroidal vasculature's red-orange color to show through against the surrounding white, edematous retina. This cherry-red spot is the single most recognizable sign of CRAO. It appears within hours of occlusion and fades over 4–6 weeks as the inner retina atrophies.
- Cattle-trucking (box-carring) of retinal vessels: Segmentation of the blood column in retinal arterioles due to sluggish or absent flow; columns of red blood cells separated by plasma gaps visible on slit-lamp biomicroscopy or fundus photography.
- Markedly attenuated retinal arterioles: The central retinal artery and its branches appear thread-like compared with veins; arteriovenous ratio is markedly decreased.
- Hollenhorst plaques: Bright, refractile, cholesterol crystals lodged at arterial bifurcations — visible in approximately 20–25% of embolic CRAO; pathognomonic for upstream atheromatous disease.
- Cilioretinal artery sparing: Approximately 15–30% of eyes have a cilioretinal artery (arising from the posterior ciliary circulation rather than the central retinal artery) that supplies the papillomacular bundle. In these eyes, a small island of preserved vision in the central field allows reading vision to be maintained despite complete CRAO — an important finding that significantly improves visual prognosis.
- Late changes: As the acute phase resolves (weeks to months), the white retinal opacity clears, the cherry-red spot disappears, and the retina becomes pale and atrophic with optic disc pallor from ganglion cell axon loss. Optociliary shunt vessels may develop at the disc.
Diagnosis and Workup
CRAO is a clinical and fundoscopic diagnosis. The workup must proceed concurrently with emergency treatment — delays for investigation are not acceptable. Key investigations include:
- Fluorescein angiography (FA): Demonstrates delay or absence of arterial filling; choroidal filling is normal (distinguishing from anterior ischemic optic neuropathy). Arm-to-retina transit time is prolonged; arteries may show staining or leakage. FA is confirmatory but should not delay treatment.
- Optical coherence tomography (OCT): Acute CRAO shows marked inner retinal thickening and hyperreflectivity (edema of ganglion cell and inner plexiform layers) with shadowing of outer retinal layers. Chronic/late CRAO shows inner retinal thinning and atrophy. OCT provides an objective measure of retinal ischemia and is increasingly used to monitor response to treatment.
- Electroretinography (ERG): In acute CRAO, the b-wave (generated by inner nuclear layer Müller and bipolar cells) is markedly reduced or absent; the a-wave (generated by photoreceptors, supplied by choroid) is preserved — the classic "negative ERG" pattern.
- Cardiovascular workup (urgent):
- ECG — screen for atrial fibrillation, recent MI, LVH
- Carotid duplex ultrasound — screen for stenosis, plaque
- Echocardiography (transthoracic; transesophageal if TTE unrevealing and cardiac source suspected) — valvular disease, thrombus, PFO, myxoma
- Brain MRI with DWI — identify concurrent ischemic stroke (present in 25–30%); embolic pattern on DWI indicates cardiac source
- Laboratory tests: CBC with differential, comprehensive metabolic panel, coagulation studies (PT/INR, aPTT), ESR, CRP (GCA screen in patients over 50), fasting lipids, Hgb A1c, fasting glucose, uric acid. In patients younger than 50 or without typical vascular risk factors: hypercoagulable panel (Factor V Leiden, prothrombin G20210A mutation, protein C/S activity, antithrombin III, antiphospholipid antibodies — lupus anticoagulant and anticardiolipin IgG/IgM), homocysteine, SPEP (if multiple myeloma suspected).
- Giant cell arteritis screening: In patients older than 50 with CRAO, GCA must be urgently excluded. ESR >50 mm/hr and CRP >2.45 mg/L are sensitive but not specific. Temporal artery biopsy is the gold standard; high-dose systemic corticosteroids should be initiated before biopsy results if clinical suspicion is high, as GCA-related visual loss is preventable.
Emergency Treatment
No treatment has been proven in large randomized controlled trials to reliably restore vision in CRAO. However, given the severity of the condition and the theoretical basis for several interventions, most centers attempt treatment rapidly when patients present within the therapeutic window. The goal is to dislodge the embolus distally and restore perfusion to as much retina as possible.
- Ocular massage: Immediate, non-invasive, performed while establishing IV access. Firm digital pressure is applied over the closed eyelid for 15 seconds followed by sudden release, repeated for 10–15 minutes. The alternating pressure changes IOP and may dislodge an embolus into a peripheral branch. Case reports document restored perfusion with this maneuver. It is low-risk and should be attempted immediately.
- Anterior chamber paracentesis (ACP): A 27–30 gauge needle is introduced at the limbus to withdraw 0.1–0.2 mL of aqueous humor, acutely reducing IOP from ~15 mmHg to near zero. The resulting perfusion pressure gradient may dilate the obstructed artery and dislodge the embolus. ACP can be performed at the slit lamp by an ophthalmologist within minutes. It carries a small risk of infection, hyphema, lens injury, and cataract.
- IOP-lowering medications: Topical beta-blockers (timolol), alpha-agonists (brimonidine), and carbonic anhydrase inhibitors (dorzolamide); systemic acetazolamide IV 500 mg. These rapidly lower IOP, increasing the arteriovenous pressure gradient.
- Inhaled carbogen (95% O2 / 5% CO2): Carbon dioxide causes vasodilation of the central retinal artery (CO2 is a potent cerebral and ocular vasodilator); the O2 component increases oxygen delivery to ischemic inner retina via diffusion from choroid. Inhaled carbogen (or alternating high-flow O2 with rebreather) has shown benefit in case series and is low-risk; limited availability outside specialized centers.
- Hyperbaric oxygen (HBO): Increases dissolved oxygen in plasma to levels sufficient to oxygenate the inner retina via diffusion from the choroid (PaO2 up to 1500 mmHg at 3 atmospheres absolute). Case series and retrospective studies report visual improvement with HBO within 12–24 hours of onset. A randomized controlled trial (HOCAT) showed improvement in patients treated within 6 hours. HBO requires specialized facilities and is not universally available.
- Intravenous tissue plasminogen activator (IV tPA): Systemic thrombolysis for CRAO remains controversial. The EAGLE trial (a randomized multicenter European study) compared IV tPA to conservative management within 6 hours and found no significant benefit in visual acuity outcomes, with a 9% rate of serious hemorrhagic complications. Current American Academy of Ophthalmology guidance does not recommend IV tPA outside of clinical trials; however, when CRAO accompanies acute ischemic stroke, neurological indication for IV tPA takes precedence.
- Intra-arterial tPA (IA-tPA): Catheter-directed thrombolysis through the ophthalmic artery (selective IA-tPA) delivers higher local drug concentrations. European centers have reported higher rates of arterial recanalization; the EAGLE trial included an IA-tPA arm showing no benefit versus conservative treatment. Not FDA-approved for this indication in the United States; associated with higher complication rates including carotid dissection and intracranial hemorrhage.
- Nd:YAG laser embolysis: Disruption of visible emboli at arterial bifurcations using YAG laser; small case series suggest benefit for branch retinal artery occlusion with visible plaque; rarely used for true CRAO.
Regardless of the specific interventions attempted, CRAO should be treated as a stroke equivalent. Patients should be urgently transferred to a stroke unit or emergency department with stroke capabilities. Brain MRI, cardiac monitoring, and cardiology/neurology consultation should proceed in parallel with ophthalmological interventions.
Secondary Prevention
Because CRAO signals significant underlying systemic vascular disease, secondary prevention is critically important — the primary long-term cause of morbidity and mortality in CRAO patients is not the visual loss but subsequent stroke, myocardial infarction, and cardiovascular death.
- Antiplatelet therapy: Aspirin 81–325 mg/day (or clopidogrel) for non-cardioembolic CRAO (atherosclerotic etiology), analogous to TIA management. Dual antiplatelet therapy (aspirin + clopidogrel) for 21 days then single agent may be considered in the acute period.
- Anticoagulation: Indicated for cardioembolic etiology — warfarin or direct oral anticoagulants (DOACs: apixaban, rivaroxaban, dabigatran) for atrial fibrillation; bridging heparin followed by warfarin or DOAC for prosthetic valve or intracardiac thrombus. Antiphospholipid antibody syndrome requires lifelong anticoagulation with warfarin (DOACs may be less effective in triple-positive APS).
- High-intensity statin therapy: Atorvastatin 40–80 mg or rosuvastatin 20–40 mg daily, regardless of baseline LDL; statins reduce subsequent cardiovascular events by 25–35% in high-risk vascular disease populations. Pleiotropic effects (endothelial stabilization, plaque stabilization, anti-inflammatory) extend beyond LDL reduction.
- Blood pressure control: Target <130/80 mmHg per current ACC/AHA guidelines for secondary cardiovascular prevention. Strict BP control reduces recurrent stroke risk by approximately 30%.
- Carotid endarterectomy or stenting: For symptomatic carotid stenosis ≥50% (by NASCET criteria), carotid endarterectomy reduces 2-year stroke risk from approximately 26% to 9% (NASCET trial). CRAO from carotid embolism is considered equivalent to TIA in most vascular surgery guidelines — early revascularization (within 2 weeks) is associated with greatest benefit.
- Giant cell arteritis: Immediate high-dose corticosteroids (IV methylprednisolone 500–1000 mg/day for 3 days, then prednisone 1 mg/kg/day) to prevent involvement of the fellow eye; risk of bilateral visual loss in untreated GCA is approximately 25–50%. Tocilizumab (anti-IL-6) added for steroid-sparing maintenance. The fellow eye may be at risk for weeks after the initial event without treatment.
- Risk factor modification: Smoking cessation (reduces subsequent vascular events by 30%), glycemic control (HbA1c <7%), and treatment of obstructive sleep apnea (CPAP reduces systemic inflammation and platelet aggregation).
Prognosis and Outcomes
Visual prognosis in CRAO is generally poor without treatment. Natural history studies from the pre-intervention era:
- Approximately 65–75% of untreated CRAO patients retain final visual acuity of 20/400 or worse (legally blind in the affected eye).
- Only 10–15% recover to 20/40 or better spontaneously, usually in the setting of cilioretinal artery sparing or partial/branch occlusion.
- Treatment within 6 hours using available interventions may improve final visual acuity in a subset — systematic reviews suggest that approximately 30–35% of treated patients achieve visual improvement compared with 10–20% in historic controls, though high-quality randomized evidence is limited.
- Cilioretinal artery sparing is the strongest predictor of preserved central vision; these patients may retain ambulatory vision or even reading vision despite complete CRAO.
- Systemic prognosis is sobering: the 10-year mortality of CRAO patients is approximately 40–50%, driven primarily by cardiovascular events. The 1-year risk of stroke after CRAO is 7–10% without secondary prevention.
- Neovascularization (of the iris — rubeosis iridis, or of the retina) develops in approximately 15–20% of CRAO eyes over weeks to months, driven by ischemia-induced VEGF release, and can lead to neovascular glaucoma — a blinding complication that requires urgent panretinal photocoagulation and IOP-lowering therapy.
Special Populations
Young Patients (<50 years)
CRAO in patients younger than 50 accounts for approximately 10–15% of cases and has a distinct etiology profile. Classic atherosclerotic risk factors are less prominent; instead, evaluation should prioritize cardiac sources (PFO with paradoxical embolism, mitral valve prolapse, valvular disease from rheumatic heart disease), hypercoagulable states, vasospasm (migraine, recreational drug use — cocaine, amphetamines), vasculitis (SLE, antiphospholipid syndrome, Behçet's disease), and sickle cell disease. These patients should receive a full hypercoagulable workup, echocardiography with bubble study (PFO screen), and rheumatological evaluation if systemic disease is suspected. PFO closure may be considered for cryptogenic CRAO in young patients after multidisciplinary review.
Giant Cell Arteritis
GCA-related CRAO is an ophthalmic emergency within an emergency. Bilateral involvement without immediate treatment carries a 50% risk of fellow-eye involvement within days. Systemic steroids must be initiated empirically — before biopsy results are available — if clinical suspicion is high (age >50, new headache, jaw claudication, scalp tenderness, polymyalgia rheumatica symptoms, markedly elevated ESR/CRP). IV methylprednisolone 1000 mg/day for 3 days is appropriate for vision-threatening GCA. Temporal artery biopsy should be obtained within 1–2 weeks of starting steroids (histological changes persist for 2–4 weeks on steroids).
Perioperative CRAO
CRAO during or after cardiac surgery, spine surgery (especially prone positioning), or any prolonged procedure with hemodynamic instability and external ocular pressure (prone head positioning with eye compression) accounts for a small but important minority of cases. Mechanisms include embolism from manipulation of atheromatous vessels (cardiac surgery), direct external ocular pressure reducing perfusion pressure (prone-position spine surgery — "position eye"), and hypotension combined with increased IOP. Prevention in spine surgery requires meticulous eye protection and avoidance of prolonged hypotension.
Key Research Papers
- Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140(3):376–391 — Search PubMed
- Schmidt D, Hetzel A, Geibel-Zehender A, Schulte-Mönting J. Systemic diseases in non-inflammatory branch and central retinal artery occlusion — an overview of 416 patients. Eur J Med Res. 2007;12(12):595–603 — Search PubMed
- Schumacher M, Schmidt D, Jurklies B, et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. 2010;117(7):1367–1375 — Search PubMed
- Biousse V, Calvetti O, Drews-Botsch CD, Newman NJ. Management of acute retinal ischemia: follow the stroke guidelines! Ophthalmology. 2018;125(8):1143–1151 — Search PubMed
- Rudkin AK, Lee AW, Aldrich E, et al. Clinical characteristics and outcome of current standard management of central retinal artery occlusion. Clin Exp Ophthalmol. 2010;38(5):496–501 — Search PubMed
- Mac Grory B, Schrag M, Biousse V, et al. Management of central retinal artery occlusion: a scientific statement from the American Heart Association. Stroke. 2021;52(6):e282–e294 — Search PubMed
- Park SJ, Choi NK, Park KH, Woo SJ. Five year nationwide incidence of retinal vein occlusion indicating an association with hypertension and diabetes. Ophthalmology. 2012;119(12):2543–2549 — Search PubMed
- Rahimy E, Sarraf D, Rhee RL, et al. Paracentral acute middle maculopathy in a broad spectrum of retinal vascular diseases. Am J Ophthalmol. 2014;158(6):1206–1215 — Search PubMed
- Hayreh SS, Zimmerman MB, Kimura A, Sanon A. Central retinal artery occlusion: retinal survival time. Exp Eye Res. 2004;78(3):723–736 — Search PubMed
- Callizo J, Feltgen N, Pantenburg S, et al. Cardiovascular risk factors in central retinal artery occlusion: results of a prospective and standardized medical examination. Ophthalmology. 2015;122(9):1881–1888 — Search PubMed
- Cugati S, Varma DD, Chen CS, Lee AW. Treatment options for central retinal artery occlusion. Curr Treat Options Neurol. 2013;15(1):63–77. PMID: 23070637
- Chen CS, Lee AW, Campbell B, et al. Efficacy of intravenous tissue-type plasminogen activator in central retinal artery occlusion: report from a randomized, controlled trial. Stroke. 2011;42(8):2229–2234 — Search PubMed
Connections
- Ophthalmology
- Retinal Vein Occlusion
- Diabetic Retinopathy
- Macular Degeneration
- Glaucoma
- Optic Neuritis
- Atrial Fibrillation
- Ischemic Stroke
- Uveitis
- Thyroid Eye Disease
- Lab Tests — Reference
- Retinal Detachment