Leukemia: History and Discovery
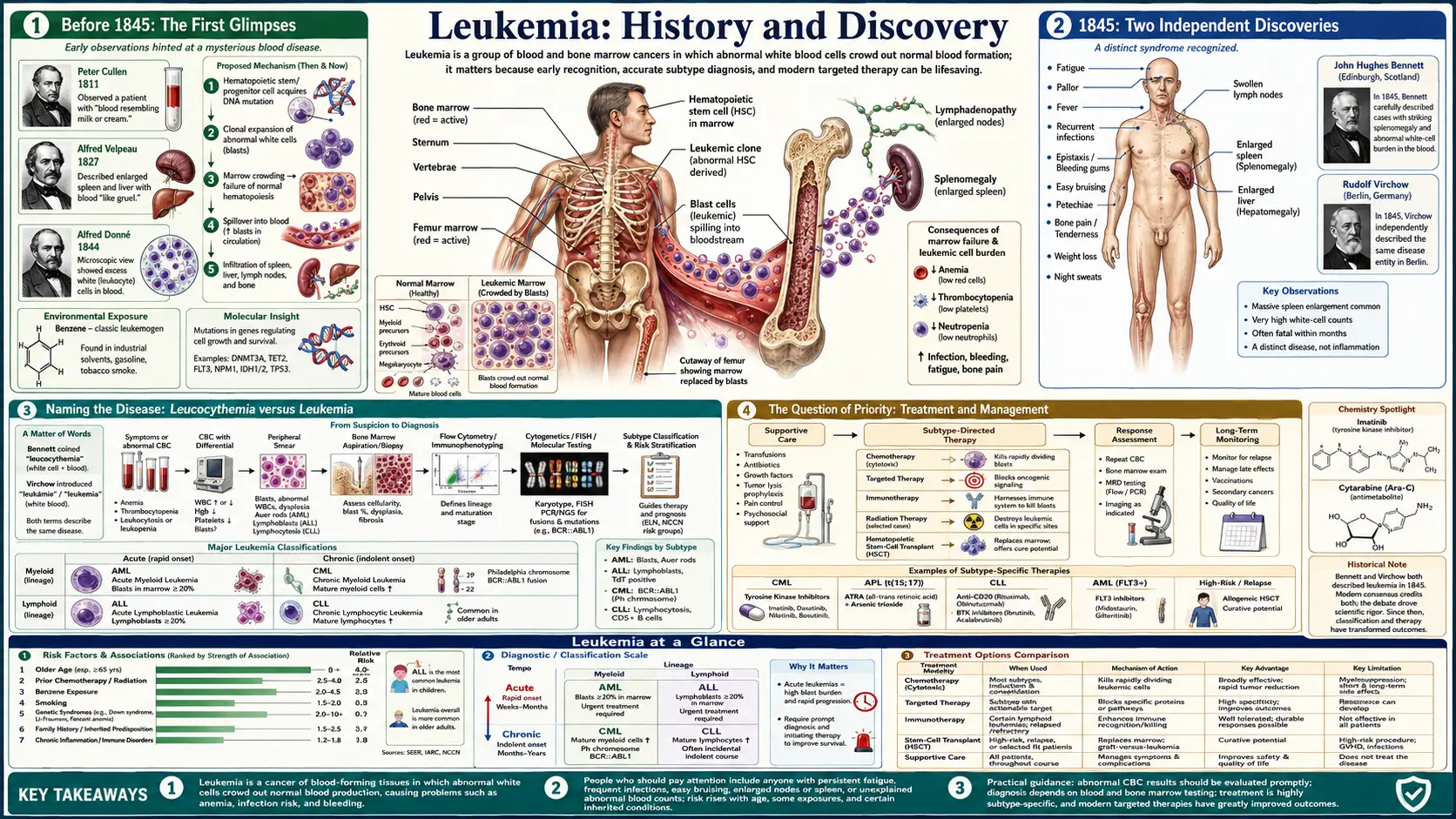
Leukemia — cancer of the blood-forming tissues — was first recognized as a distinct disease in 1845, when two physicians working independently, Rudolf Virchow in Berlin and John Hughes Bennett in Edinburgh, described patients whose blood held an extraordinary excess of pale, colorless cells. Bennett called it leucocythemia and blamed infection; Virchow, unconvinced, named it weisses Blut (“white blood”) and, in 1847, coined the enduring Greek term leukämie — leukemia. From that disputed beginning the story runs through Ernst Neumann’s discovery of the bone marrow as its source, the carving-out of acute and chronic, myeloid and lymphoid subtypes, the first chemotherapy remissions of 1948, the 1960 discovery of the Philadelphia chromosome, and the 2001 arrival of imatinib — one of the longest and most instructive arcs in the history of medicine.
Table of Contents
- Before 1845: The First Glimpses
- 1845: Two Independent Discoveries
- Naming the Disease: Leucocythemia versus Leukemia
- The Question of Priority
- Ernst Neumann and the Bone Marrow
- Defining the Subtypes
- The First Remissions: Chemotherapy Begins
- The Philadelphia Chromosome, 1960
- Targeted Therapy and the Imatinib Era
- Research Papers and References
- Connections
- Featured Videos
Before 1845: The First Glimpses
The disease that would later be named leukemia did not announce itself all at once. Through the late eighteenth and early nineteenth centuries, several physicians recorded autopsies of patients with hugely enlarged spleens and oddly thick, pale, almost milky blood — observations that, in hindsight, were probably leukemia but were not understood as a disease of the blood itself. Scattered case reports by physicians such as Alfred-François Velpeau (who in 1827 described a florist and lemonade-seller with an enormous spleen and blood “like gruel”) and Alfred Donné are now read as early encounters with the condition, but at the time the changes in the blood were not recognized as the heart of the matter.
The single most important pre-1845 contribution came from the French microscopist Alfred Donné. In 1844 — about a year before the famous 1845 papers — Donné used the microscope (and even early daguerreotype photomicrographs) to examine leukemic blood and noted what he interpreted as a failure of the white cells to mature normally, distinguishing these colorless corpuscles from pus. Donné is therefore often credited as the first to give an accurate microscopic description of the altered blood seen in leukemia. It is historically honest to say that he saw the abnormality before Bennett and Virchow did; what he did not do was define it as a new, distinct disease entity.
This distinction — between observing an abnormality and recognizing a disease — matters for telling the story accurately. The microscope was still a young and distrusted instrument in clinical medicine, and the idea that the blood itself could be the seat of a primary disease ran against the prevailing humoral and inflammatory thinking. The stage was set for someone to look at the same pale corpuscles and argue, against the grain, that they defined a condition in their own right.
1845: Two Independent Discoveries
The year 1845 is the conventional birth-date of leukemia as a recognized disease, and remarkably it was described twice that year by two physicians who did not know of each other’s work. In Edinburgh, the pathologist John Hughes Bennett (1812–1875) published, in the Edinburgh Medical and Surgical Journal, a detailed case of a patient who had died with a massively enlarged spleen and liver and blood teeming with colorless cells. Bennett’s account, appearing in October 1845, is generally regarded as the first published clinical-pathological description of the condition as a named entity.
Roughly six weeks later in Berlin, the young pathologist Rudolf Virchow (1821–1902) independently published his own autopsy case — a woman, a cook, with a greatly enlarged spleen and blood so full of pale corpuscles that the white cells rivaled or outnumbered the red. Virchow’s paper carried the plain, arresting title Weisses Blut (“White Blood”). Because the two reports appeared so close together, in different countries and languages, and reached different conclusions about the cause, 1845 is rightly remembered as a case of near-simultaneous independent discovery rather than a single eureka moment.
Both men were looking at what we now recognize as a chronic leukemia — almost certainly chronic myeloid leukemia in at least one of the cases — with its hallmark huge spleen and dramatic white-cell excess. What separated their accounts from Donné’s earlier microscopy was the explicit claim that this represented a coherent disease, a real and reproducible state of the blood and blood-forming organs, rather than an incidental finding or a variant of suppuration. That claim is what makes 1845 the founding year.
Naming the Disease: Leucocythemia versus Leukemia
The two discoverers disagreed sharply about what they had found, and their disagreement is preserved in the names they chose. Bennett believed the abundant pale cells were essentially pus, and that the condition arose from suppuration — a hidden infection or inflammation seeding the blood with purulent material. Consistent with that interpretation he named the disease leucocythemia (literally “white-cell blood”), a term that described the appearance while implying his infectious theory. For some decades “leucocythemia” remained in common use, especially in Britain.
Virchow rejected the infection theory. Examining his case, he concluded that the white, pus-like material was not infectious matter at all but an enormous, primary excess of the blood’s own colorless corpuscles — the cells we now call white blood cells (leukocytes). In 1845 he simply called the condition weisses Blut, German for “white blood.” Two years later, in 1847, he replaced this plain description with a coined scientific term built from Greek: leukämie, from leukos (“white”) and haima (“blood”) — the direct ancestor of the English word leukemia (British leukaemia). It is this 1847 coinage, not the 1845 papers, that gave the disease its lasting name.
Virchow’s naming was more than a label; it embodied a correct and radical idea — that leukemia is a primary disorder of the blood-forming system rather than a by-product of infection. As his pathological thinking matured he went further, distinguishing (by the mid-1850s) between a “splenic” form centered on the spleen and a “lymphatic” form centered on the lymph nodes, an early intuition of the later split between myeloid leukemias and the lymphoid leukemias and lymphomas. The terminology shifted gradually over the following decades, and Virchow’s “leukemia” ultimately prevailed over Bennett’s “leucocythemia” precisely because Virchow’s underlying explanation proved correct.
The Question of Priority
Because Bennett and Virchow described the disease within weeks of each other, a question of priority — who deserved credit for the discovery — inevitably arose, and it deserves to be told honestly rather than flattened into a tidy “Virchow discovered leukemia.” By the strict measure of publication date, Bennett’s 1845 paper appeared first, and several historical reviews accordingly credit him with the earliest published description of the disease as an entity. Virchow himself, the more famous figure, is frequently but somewhat unfairly remembered as the sole discoverer.
What is striking is how the priority issue was resolved. Rather than feuding bitterly, Virchow is recorded as having acknowledged Bennett’s priority of publication, and the relationship between the two men remained cordial — by some accounts Virchow even wrote in support of Bennett’s professional advancement. The lasting verdict of medical history is a shared one: Bennett gave the first published clinical description and the first name (leucocythemia), while Virchow supplied the correct interpretation and the enduring name (leukemia) and built it into a broader theory of blood disease.
Fairness also requires keeping Alfred Donné in the picture, since his 1844 microscopy preceded both. A balanced summary — and the one best supported by the historical literature — is that Donné first saw the abnormal blood, Bennett first published it as a disease, and Virchow first correctly explained and named it. No single person “discovered leukemia” in isolation; the recognition emerged from several observers within a remarkably short span, which is itself a characteristic pattern in the history of medicine.
Ernst Neumann and the Bone Marrow
The 1845 discoverers had localized leukemia to the blood, the spleen, and the lymph nodes, but they did not know where the excess white cells actually came from. That answer arrived a generation later through the German pathologist Franz Ernst Christian Neumann (1834–1918) of Königsberg. In a series of papers around 1868–1872, Neumann established that blood cells are produced in the bone marrow — a then-novel idea — and, crucially, that leukemia is a disease of the marrow itself. He observed that the marrow of leukemic patients was abnormal and concluded that the disorder originated there rather than in the circulating blood or the spleen alone.
Neumann’s insight was foundational for hematology as a whole. He is credited with first proposing the bone marrow as the body’s blood-forming organ in postembryonic life and with the concept that the various blood cells share a common origin there — an early ancestor of the modern stem-cell idea. Reflecting this marrow-centered understanding, he introduced the term myelogenous leukemia (from Greek myelos, “marrow”) for the form arising from marrow cells, distinguishing it from the lymphatic form arising in the lymphoid tissue.
With Neumann’s work the basic anatomy of leukemia fell into place: an abnormal, uncontrolled production of white cells originating in the bone marrow, spilling into the blood and enlarging the spleen and lymph nodes. This marrow-based framework is the one still used today, and it set the stage for classifying leukemias by which marrow or lymphoid lineage had gone wrong.
Defining the Subtypes
Once leukemia was accepted as a marrow disease, physicians began to notice that it was not one disease but several, differing in tempo and in the kind of cell involved. Two great axes of classification emerged in the second half of the nineteenth century. The first axis — acute versus chronic — was opened by the German pathologist Nikolaus Friedreich, who in 1857 reported a strikingly rapid, fulminant case quite unlike the slow, spleen-dominated illness Bennett and Virchow had described. The explicit term acute leukemia was used to mark this fast, aggressive form, and in 1889 Wilhelm Ebstein helped fix the clinical distinction between acute and chronic leukemia in the medical vocabulary.
The second axis — myeloid versus lymphoid — depended on being able to tell blood cells apart under the microscope, and that became possible through the staining revolution led by Paul Ehrlich. From 1877 onward Ehrlich’s aniline dyes and differential stains allowed the granulated myeloid cells to be distinguished from lymphoid cells, making it possible to separate myeloid leukemias (arising from the granulocyte-producing marrow lineage) from lymphoid leukemias (arising from lymphocytes). Building on such staining, hematologists including Otto Naegeli later defined the myeloblast and formalized the division of leukemia into myeloid and lymphocytic types.
Combining the two axes produced the four classic categories that organize the disease to this day: acute myeloid leukemia (AML), chronic myeloid leukemia (CML), acute lymphoblastic/lymphocytic leukemia (ALL), and chronic lymphocytic leukemia (CLL). This framework was not the work of any one person or year; it accreted over roughly half a century as clinical observation of disease course was joined to microscopic identification of cell type. It remains the scaffold onto which all later molecular discoveries — chromosomes, fusion genes, targeted drugs — were eventually fitted.
The First Remissions: Chemotherapy Begins
For its first century leukemia was essentially untreatable; a diagnosis, especially of an acute leukemia in a child, was a death sentence measured in weeks or months. The first genuine crack in that wall came in 1948 and grew out of an apparent failure. The Boston pathologist Sidney Farber (1903–1973) had observed that folic acid, far from helping, seemed to accelerate leukemia in children. Reasoning that a compound which blocked folic acid might do the opposite, he turned to folate antagonists synthesized by Yellapragada Subbarow and colleagues at Lederle Laboratories.
Using the antifolate drug aminopterin, Farber treated a small group of children with acute lymphoblastic leukemia and, in several of them, achieved temporary complete remissions — the leukemic blasts cleared from the blood and marrow and normal blood production briefly returned. He reported the results in the New England Journal of Medicine on June 3, 1948, in a paper describing temporary remissions in childhood acute leukemia produced by a folic-acid antagonist. The remissions were not cures — the disease relapsed — but they proved for the first time that a drug could drive leukemia into retreat.
The importance of 1948 is hard to overstate: it is widely regarded as the dawn of modern cancer chemotherapy, and Farber is often called the father of that field. Aminopterin’s close relative methotrexate (amethopterin) soon followed and remains in use against leukemia and other cancers today. Over the following decades, combination chemotherapy — stacking several drugs with different mechanisms — transformed childhood ALL in particular from an almost uniformly fatal disease into one that is now curable in the large majority of children, one of the signal achievements of twentieth-century medicine.
The Philadelphia Chromosome, 1960
The next landmark shifted leukemia from a disease defined by cells to a disease defined by genes. In 1960, two researchers in Philadelphia — Peter Nowell of the University of Pennsylvania and David Hungerford, a graduate student at the Fox Chase Cancer Center (then the Institute for Cancer Research) — reported that cells from patients with chronic myeloid leukemia consistently carried an abnormally small chromosome 22. The minute chromosome was named the Philadelphia chromosome after the city where it was found.
What made this finding historic was its consistency. Earlier studies had glimpsed chromosomal disorder in cancer cells, but those changes looked random and idiosyncratic. The Philadelphia chromosome was different: it turned up reliably, case after case, in the same type of leukemia. This made it the first consistent (nonrandom) chromosomal abnormality linked to a specific human cancer — powerful early evidence that cancer is, at root, a genetic disease of the cell, a then-controversial idea that the Philadelphia chromosome helped to establish.
The discovery’s full meaning unfolded only later. In 1973 Janet Rowley, using newer chromosome-banding techniques, showed that the Philadelphia chromosome is produced by a reciprocal translocation — a swap of material between chromosomes 9 and 22 — rather than a simple deletion. By the 1980s researchers had pinned down that this translocation fuses two genes, BCR and ABL, creating a BCR-ABL fusion gene whose product is an abnormally switched-on tyrosine kinase enzyme that drives the leukemia. That precise molecular knowledge turned the Philadelphia chromosome from a diagnostic curiosity into a drug target.
Targeted Therapy and the Imatinib Era
The line that began with a small chromosome in 1960 reached a triumphant conclusion at the turn of the millennium. Once the BCR-ABL fusion protein was understood to be a constantly active tyrosine kinase — the engine of chronic myeloid leukemia — it became possible to imagine a drug designed to switch that one engine off, sparing healthy cells. The oncologist Brian Druker, working with chemists at the company then known as Ciba-Geigy/Novartis, championed exactly such a molecule: a small-molecule kinase inhibitor first labeled STI-571 and later named imatinib, marketed as Gleevec (Glivec outside the United States).
Imatinib’s clinical trials were stunning. Patients with chronic-phase CML, many of whom would previously have died within a few years, achieved deep and durable remissions with a well-tolerated daily pill. The U.S. Food and Drug Administration approved imatinib for CML on May 10, 2001, in record time, and the drug famously appeared on the cover of Time magazine as a symbol of a new era. Long-term follow-up has since shown that imatinib turned CML from a frequently fatal disease into a chronic, manageable condition for most patients, with five-year survival rising dramatically.
Imatinib’s deeper significance is that it was the first widely successful example of rationally designed, molecularly targeted cancer therapy — a drug aimed at the specific genetic lesion driving a cancer, rather than a general poison of dividing cells. It validated the entire concept of precision oncology and inspired a generation of later targeted drugs, including newer BCR-ABL inhibitors (dasatinib, nilotinib, and others) for patients who relapse or cannot tolerate imatinib. In a single disease, leukemia thus traces the full sweep of modern oncology: from a pale corpuscle under Donné’s microscope, to Virchow’s naming, to a marrow disorder, to a fusion gene, to a pill that switches that gene’s product off.
Research Papers and References
The references below combine peer-reviewed historical reviews with curated PubMed topic-search links into the literature on the discovery and early understanding of leukemia. Nineteenth-century primary texts (Bennett’s 1845 case report, Virchow’s Weisses Blut and 1847 coinage of leukämie, Donné’s 1844 microscopy, and Neumann’s 1868–1872 marrow papers) are named in the article as historical sources rather than as modern citations. Each link opens at the National Library of Medicine (PubMed) or the cited journal in a new tab.
- Kampen KR. The discovery and early understanding of leukemia. Leukemia Research. 2012;36(1):6-13. — doi:10.1016/j.leukres.2011.09.028
- Piña-Oviedo S, et al. John Hughes Bennett, Rudolph Virchow… and Alfred Donné: the first description of leukemia. The Hematology Journal (review of priority). — PubMed 11920227
- Geary CG. The story of chronic myeloid leukaemia. British Journal of Haematology. 2000;110(1):2-11. — doi:10.1046/j.1365-2141.2000.02137.x
- Nowell PC, Hungerford DA. A minute chromosome in human chronic granulocytic leukemia. Science. 1960;132:1497. (The Philadelphia chromosome.) — PubMed: Nowell & Hungerford 1960
- Nowell PC. Discovery of the Philadelphia chromosome: a personal perspective. Journal of Clinical Investigation. 2007;117(8):2033-2035. — doi:10.1172/JCI31771
- Rowley JD. A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature. 1973;243:290-293. (The 9;22 translocation.) — doi:10.1038/243290a0
- Farber S, Diamond LK. Temporary remissions in acute leukemia in children produced by folic acid antagonist, 4-aminopteroyl-glutamic acid (aminopterin). New England Journal of Medicine. 1948;238(23):787-793. — doi:10.1056/NEJM194806032382301
- Druker BJ, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. New England Journal of Medicine. 2001;344(14):1031-1037. — doi:10.1056/NEJM200104053441401
- Wapner J / historical reviews of imatinib (Gleevec) and the BCR-ABL story — PubMed: imatinib history and BCR-ABL targeted therapy
- Franz Ernst Christian Neumann and the bone marrow as the blood-forming organ — PubMed: Neumann, bone marrow and leukemia history
- History of the acute/chronic and myeloid/lymphoid classification of leukemia (Friedreich, Ebstein, Ehrlich, Naegeli) — PubMed: history of leukemia classification
- Rudolf Virchow and the founding of cellular pathology — PubMed: Virchow, cellular pathology and leukemia
- Sidney Farber and the origins of cancer chemotherapy — PubMed: Sidney Farber and the origins of chemotherapy
- General history of leukemia diagnosis and treatment, beginnings to the present — PubMed: history of leukemia discovery, diagnosis and treatment
External Authoritative Resources
- National Cancer Institute (NCI) — Leukemia
- NCI — How Gleevec (imatinib) Transformed Leukemia Treatment
- PubMed — All research on the history of leukemia