Delirium
Delirium is an acute neurocognitive emergency defined by sudden-onset, fluctuating disturbances in attention, awareness, and cognition that cannot be explained by a pre-existing or evolving neurodegenerative disorder. It is one of the most common and consequential complications of hospitalization, affecting 10–30% of all admitted adults, 14–56% of ICU patients, and up to 80% of those receiving mechanical ventilation. Despite its frequency and severity — delirium independently prolongs hospital stays, accelerates cognitive decline, and increases both short- and long-term mortality — it remains dramatically underrecognized, particularly the hypoactive subtype, which is routinely mistaken for depression or simple fatigue. Understanding delirium as a brain emergency rather than an expected inconvenience of illness is the single most important shift in modern hospital medicine.
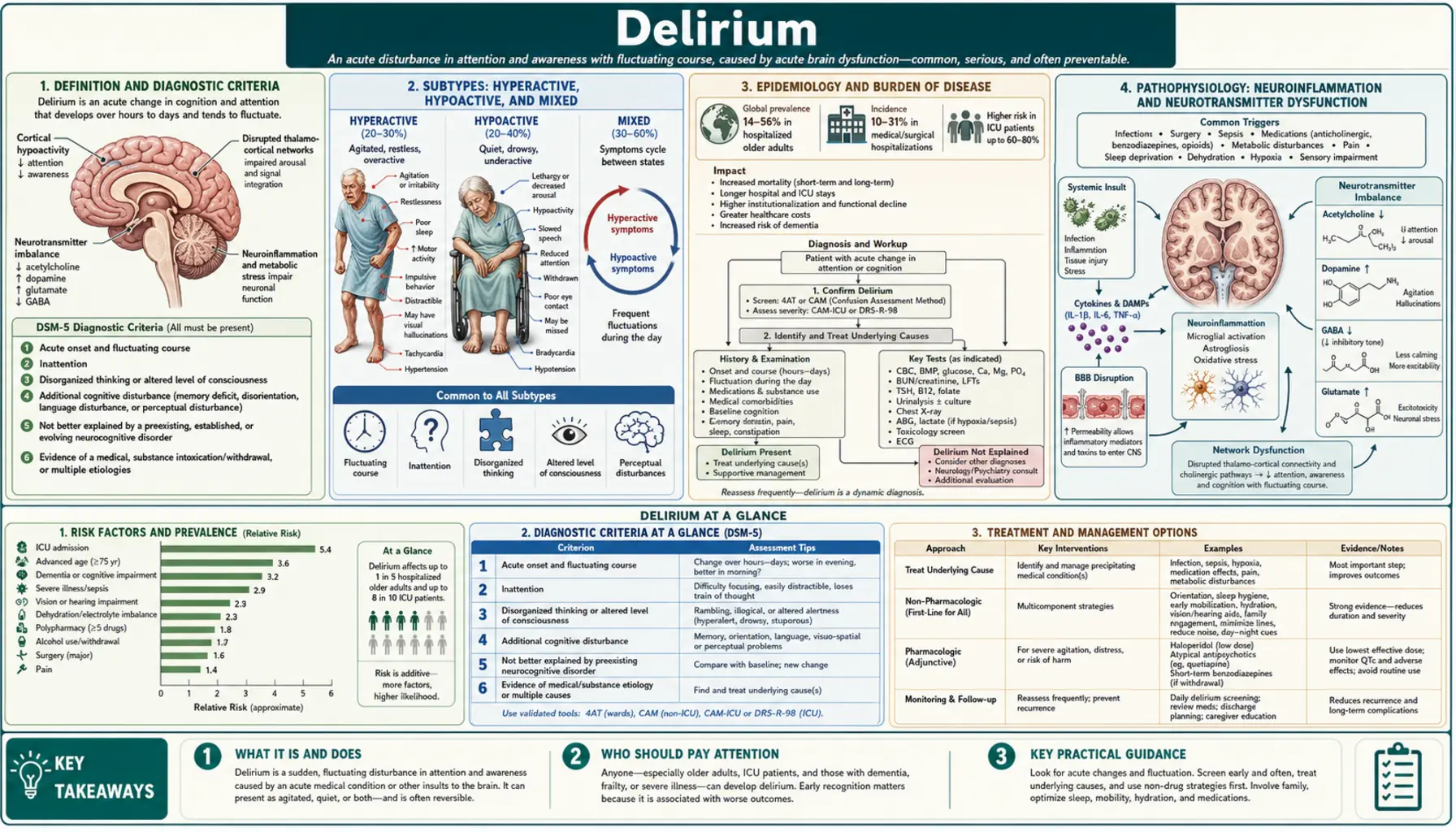
- Definition and Diagnostic Criteria
- Subtypes: Hyperactive, Hypoactive, and Mixed
- Epidemiology and Burden of Disease
- Pathophysiology: Neuroinflammation and Neurotransmitter Dysfunction
- Precipitants and Predisposing Risk Factors
- Diagnosis and Assessment Tools
- Investigations and Key Differentials
- Non-Pharmacological Management: The HELP Protocol
- Pharmacological Treatment and Special Scenarios
- Outcomes: Mortality, Cognitive Decline, and Long-Term Consequences
- Key Research Papers
- Connections
Definition and Diagnostic Criteria
The DSM-5 defines delirium by five core criteria: (1) a disturbance in attention — reduced ability to direct, focus, sustain, and shift attention — and in awareness; (2) the disturbance develops over a short period (hours to days) and tends to fluctuate during the course of a day; (3) an additional disturbance in cognition — memory deficit, disorientation, language disturbance, visuospatial ability, or perception; (4) the disturbances are not better explained by a pre-existing or evolving neurodegenerative disorder; and (5) there is evidence from the history, physical exam, or laboratory findings that the disturbance is a direct physiological consequence of a medical condition, substance intoxication or withdrawal, or medication exposure.
The defining features can be remembered with the mnemonic AIOU: Acute onset and Attention deficit, Inattention (core), Over a fluctuating course, and Underlying organic cause. The fluctuating course — characteristically worse at night ("sundowning") and transiently better with stimulation — distinguishes delirium from dementia, which is progressive and non-fluctuating. Inattention is the cardinal feature: a delirious patient cannot recite the months of the year backward, cannot track an interview topic, and will lose the thread of conversation mid-sentence.
It is essential to distinguish delirium from dementia (chronic, stable attention, no acute onset), depression (preserved attention, no disorientation, no fluctuation), and primary psychotic disorders (chronic, no fluctuating course, generally in younger patients without acute medical illness). Critically, delirium and dementia coexist in the majority of elderly patients — pre-existing dementia is the single strongest risk factor for delirium, and delirium itself accelerates underlying dementia.
Back to Table of ContentsSubtypes: Hyperactive, Hypoactive, and Mixed
Delirium is classified into three motor subtypes based on the level of psychomotor activity. Recognition of subtype is critical because only one is easy to detect at the bedside, and the others carry worse prognoses despite — or because of — going undetected.
Hyperactive delirium is the most recognizable but least common subtype, accounting for approximately 25% of cases. Patients are agitated, combative, restless, and may attempt to remove intravenous lines, catheters, or endotracheal tubes. Hallucinations — most commonly visual — are prominent. Patients may be verbally aggressive or attempt to climb out of bed. Because this subtype is impossible to ignore, it is promptly diagnosed, but it represents only a minority of the delirium burden.
Hypoactive delirium is the most common subtype (approximately 50% of cases) and the most dangerous precisely because it is most frequently missed. Patients are quiet, withdrawn, somnolent, and minimally responsive. They appear "comfortable" or "sleeping off their illness," and nurses and physicians may interpret this as appropriate rest. This subtype is most common in the elderly and in patients with pre-existing dementia. Studies show hypoactive delirium carries a worse prognosis than hyperactive delirium, likely because the underlying cause goes unaddressed for longer. It is routinely misdiagnosed as depression or fatigue.
Mixed delirium accounts for approximately 25% of cases and fluctuates between hyperactive and hypoactive features over the course of a day. A patient may be combative at 2 a.m. and minimally responsive by morning rounds. Mixed delirium requires vigilant reassessment at multiple time points because a single snapshot evaluation may completely mischaracterize the clinical picture.
Back to Table of ContentsEpidemiology and Burden of Disease
Delirium affects an estimated 7 million hospitalized Americans annually. Prevalence on general medical wards ranges from 10–30%; in surgical patients following major operations (particularly cardiac and orthopedic surgery), rates climb to 15–53%. In the ICU, delirium affects 14–56% of patients overall and up to 60–80% of those receiving mechanical ventilation. Postoperative delirium is one of the most common surgical complications in patients over 65, with hip fracture repair carrying among the highest rates of any procedure.
The economic burden is enormous. Each episode of delirium is associated with increased ICU and hospital length of stay, higher rates of in-hospital complications (falls, aspiration, pressure ulcers, self-extubation), increased discharge to skilled nursing or long-term care facilities rather than home, and direct mortality. A landmark analysis estimated the annual healthcare cost attributable to delirium in the United States at $143–$152 billion, exceeding the costs of falls and diabetes-related complications.
Long-term consequences extend far beyond the hospital stay. Patients who experience delirium — even a single episode — have a significantly increased risk of subsequent dementia and accelerated cognitive decline, even after adjusting for baseline cognitive function. The relationship between delirium and dementia is bidirectional: dementia predisposes to delirium, and delirium accelerates and may directly cause dementia through neuroinflammatory injury. Hospital-acquired delirium is now recognized as a major driver of the post-intensive care syndrome (PICS), which includes persistent cognitive impairment, psychiatric morbidity, and physical debilitation lasting months to years after ICU discharge.
Back to Table of ContentsPathophysiology: Neuroinflammation and Neurotransmitter Dysfunction
The pathophysiology of delirium is genuinely multifactorial, and no single unifying mechanism explains all cases. Several complementary hypotheses have substantial supporting evidence, and they converge on a common endpoint: acute widespread cortical and subcortical dysfunction impairing the neural networks that sustain attention and arousal.
The neuroinflammatory hypothesis is currently the most influential framework. Peripheral inflammatory triggers — infection, surgery, trauma, or critical illness — cause systemic release of pro-inflammatory cytokines including interleukin-1β, interleukin-6, and tumor necrosis factor-alpha. These cytokines cross or circumvent the blood-brain barrier through active transport, circumventricular organs, or barrier disruption, activating microglia and astrocytes. Neuroinflammation then disrupts the cholinergic, dopaminergic, and glutamatergic systems. A core feature of the resulting neurotransmitter imbalance is cholinergic deficiency combined with dopaminergic excess — the same pharmacological imbalance deliberately created by anticholinergic drugs, which are a major precipitant of delirium. Acetylcholine plays a central role in maintaining cortical arousal and attentional networks; its deficiency impairs these systems acutely.
The oxidative stress and mitochondrial dysfunction hypothesis proposes that acute illness, hypoxia, and metabolic derangements impair neuronal aerobic metabolism, increasing reactive oxygen species, disrupting neurotransmitter synthesis, and triggering synaptic failure. This hypothesis explains why metabolic derangements (hypoxia, uremia, hyponatremia, hypoglycemia) are such powerful delirium precipitants. Genetic factors also play a role: polymorphisms in genes involved in inflammatory signaling, cholinergic neurotransmission, and apolipoprotein E (APOE-ε4 genotype) confer increased susceptibility to delirium.
Back to Table of ContentsPrecipitants and Predisposing Risk Factors
Delirium is best understood as a two-hit phenomenon: predisposing vulnerabilities lower the threshold for delirium, while precipitating insults trigger it. Understanding both components is essential for prevention and treatment.
Predisposing (baseline) risk factors include: advanced age (the single most important predisposing factor); pre-existing dementia or cognitive impairment (increases delirium risk 2–5 fold); functional impairment and dependence in activities of daily living; vision or hearing impairment; dehydration at baseline; and prior episodes of delirium. These factors reduce the brain's reserve, so that even minor precipitants can trigger delirium in vulnerable patients.
Precipitating factors include the common mnemonic triggers — infection (most common: urinary tract infection, pneumonia, sepsis), medications, metabolic derangements, and environmental factors:
- Infection and sepsis: The most common precipitant. Any infection can cause delirium in vulnerable patients, and delirium may be the only presenting sign of sepsis in the elderly.
- Medications (Beers Criteria drugs): Anticholinergics (diphenhydramine, promethazine, tricyclic antidepressants, bladder antimuscarinics, scopolamine), benzodiazepines, opioids, corticosteroids, and polypharmacy (≥5 medications) are major precipitants. Medication review is mandatory in every case of delirium.
- Metabolic derangements: Hyponatremia or hypernatremia, uremia, hepatic encephalopathy, hypoglycemia or hyperglycemia, hypothyroidism or hyperthyroidism, hypercalcemia, and hypoxia or hypercapnia.
- Pain and urinary retention: Uncontrolled pain and the discomfort of urinary retention are underrecognized precipitants that respond to simple interventions.
- Constipation and fecal impaction: Particularly in elderly patients, severe constipation can precipitate delirium.
- Sensory deprivation: Absence of glasses, hearing aids, or familiar stimuli in an unfamiliar hospital environment profoundly impairs the brain's ability to orient.
- Sleep deprivation and disruption: ICU environments with continuous lighting, noise, and frequent nighttime interventions are powerful precipitants.
- Immobility: Prolonged bed rest and restraint use (physical or chemical) independently worsen and prolong delirium.
Diagnosis and Assessment Tools
Delirium is a clinical diagnosis. No laboratory test or imaging finding is pathognomonic; the diagnosis rests on recognizing the characteristic clinical features — acute onset, fluctuating course, inattention, and altered cognition — and applying validated assessment tools.
The Confusion Assessment Method (CAM), developed by Inouye and colleagues in 1990, is the gold standard bedside delirium screening tool with sensitivity of 94–100% and specificity of 90–95%. The CAM algorithm requires: (1) acute onset and fluctuating course (and) (2) inattention (and either) (3) disorganized thinking (or) (4) altered level of consciousness. All four features should be assessed; delirium is diagnosed if features 1 and 2 are present, plus either feature 3 or 4. A common error is diagnosing delirium based only on altered consciousness without confirming inattention and fluctuation.
The CAM-ICU is a validated adaptation for use in intubated patients who cannot speak. It assesses the same four features using nonverbal tasks — for example, inattention is assessed by squeezing the examiner's hand only when the letter "A" is said in a sequence of letters recited aloud. The CAM-ICU has sensitivity of 76–96% and specificity of 72–96% across validation studies and is the standard tool recommended by the Society of Critical Care Medicine's PADIS guidelines.
The 3-Minute Diagnostic Assessment for Confusion (3D-CAM) and the brief CAM (bCAM) are validated short-form instruments suitable for non-ICU settings where formal delirium screening by nursing or medical staff takes only a few minutes. The Glasgow Coma Scale (GCS) alone is insufficient for diagnosing delirium because it captures level of consciousness but not inattention or cognitive quality.
Back to Table of ContentsInvestigations and Key Differentials
Investigation in delirium serves two purposes: identifying the underlying cause(s) and excluding critical mimics. The investigation must be broad because delirium is a syndrome, not a diagnosis, and the underlying cause is frequently multifactorial.
Standard workup includes: complete blood count (CBC) for infection, anemia; basic metabolic panel (BMP) for sodium, potassium, glucose, renal function, bicarbonate; liver function tests (LFTs) for hepatic encephalopathy; thyroid-stimulating hormone (TSH) for thyroid dysfunction; urinalysis and urine culture; blood cultures if infection is suspected; oxygen saturation and arterial blood gas if hypoxia or hypercapnia is possible; and a thorough medication review. Chest imaging, urine toxicology, and blood alcohol level are added based on clinical context. A brain CT scan is indicated if there is new focal neurological deficit, history of head trauma, fever and nuchal rigidity suggesting meningitis, or first-episode delirium in a young patient without a clear cause.
Critical differentials that must be actively excluded include: non-convulsive status epilepticus (NCSE) — an EEG is essential when delirium is unexplained or unusually prolonged, because NCSE can mimic delirium and is treatable; Wernicke's encephalopathy — in any malnourished or alcoholic patient, give empirical IV thiamine before glucose; autoimmune encephalitis (anti-NMDAR, anti-LGI1, anti-CASPR2) — suspect in subacute delirium with psychiatric features, new-onset seizures, or autonomic instability, especially in younger patients; and meningitis or encephalitis — lumbar puncture is essential when fever plus delirium plus any meningeal sign is present.
Back to Table of ContentsNon-Pharmacological Management: The HELP Protocol
Non-pharmacological interventions are first-line for both prevention and treatment of delirium. Multiple randomized controlled trials demonstrate that multicomponent non-pharmacological protocols reduce delirium incidence by 30–40% in high-risk hospitalized patients. The most rigorously studied program is the Hospital Elder Life Program (HELP), developed by Inouye and colleagues at Yale.
HELP targets six primary delirium risk factors with the following interventions:
- Cognitive impairment: Reorientation (orientation board with date, location, care team names), cognitive activities (word games, reminiscing), provision of familiar stimuli (family photos, favorite music, personal items from home).
- Sleep deprivation: Non-pharmacological sleep protocol — warm milk or herbal tea at bedtime, relaxation music, back massage, noise-reduction strategies (earplugs, staff education about nighttime noise), clustering of nighttime care to minimize disruptions.
- Immobility: Early mobilization — ambulation three times daily or active range-of-motion exercises for patients unable to ambulate; minimize bed rest, avoid restraints which worsen agitation and immobility.
- Visual impairment: Ensure glasses are at bedside and worn; use magnifying lenses if needed; adequate lighting.
- Hearing impairment: Portable amplifying devices; ensure hearing aids are in and functioning; reduce background noise.
- Dehydration: Early recognition and treatment; encourage oral fluid intake; eliminate unnecessary fluid restrictions.
The ABCDEF bundle (Assess, prevent and manage pain; Both SAT and SBT; Choice of analgesia and sedation; Delirium monitoring and management; Early mobility; Family engagement and empowerment) is the ICU equivalent and is recommended by the Society of Critical Care Medicine. Family presence and engagement, in particular, has a strong effect on delirium prevention and treatment in the ICU by providing familiar stimuli and reorientation.
Back to Table of ContentsPharmacological Treatment and Special Scenarios
Pharmacological treatment of delirium should be reserved for agitation that poses immediate safety risk to the patient or staff, after non-pharmacological measures have been attempted. No medication reduces delirium incidence, shortens duration, or improves mortality outcomes in unselected patients — this was definitively shown for haloperidol in the MIND-USA trial (Hope et al., 2018, NEJM) and for haloperidol and ziprasidone in the MIND trial.
Antipsychotics are the most commonly used agents for agitation management. Low-dose haloperidol (0.5–1 mg IV or IM, repeated every 4 hours as needed) remains the most studied agent. Quetiapine (25–50 mg orally twice daily) and olanzapine are alternatives with sedating properties useful in specific contexts. All antipsychotics carry risks of QTc prolongation, extrapyramidal side effects, and — in patients with dementia — increased stroke and mortality risk (black box warning). They should be used at the lowest effective dose for the shortest time and should be tapered and discontinued as soon as agitation resolves.
Dexmedetomidine, a selective alpha-2 agonist, is preferred for managing hyperactive delirium in mechanically ventilated ICU patients because it provides sedation without worsening delirium by the mechanism of benzodiazepines. Multiple trials demonstrate lower delirium incidence and shorter time to extubation with dexmedetomidine versus benzodiazepine-based sedation.
Benzodiazepines must be avoided in most delirium — they worsen delirium by enhancing GABAergic inhibition and impairing cholinergic neurotransmission. The critical exception is alcohol withdrawal delirium (delirium tremens), where benzodiazepines are the first-line and potentially life-saving treatment. Delirium tremens typically begins 24–72 hours after the last drink, features autonomic hyperactivity (tachycardia, hypertension, diaphoresis, fever) and seizures, and carries up to 5% mortality if untreated. The CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol) protocol guides benzodiazepine dosing in this specific scenario.
Back to Table of ContentsOutcomes: Mortality, Cognitive Decline, and Long-Term Consequences
Delirium is an independent predictor of adverse outcomes even after controlling for severity of illness, pre-existing dementia, and comorbidities. In-hospital delirium is associated with a 2–5 fold increase in mortality during hospitalization, an approximately 2-fold increase in 1-year mortality, and significantly increased rates of discharge to nursing home rather than home. In the ICU, each additional day of delirium is associated with a 10% increase in the hazard of death at 1 year (Shehabi et al., 2010).
Perhaps the most clinically important but underappreciated long-term consequence is accelerated cognitive decline. The BRAIN-ICU study (Pandharipande et al., NEJM 2013) demonstrated that 3-month and 12-month cognitive impairment in ICU survivors — measured by standard neuropsychological testing — was linearly associated with the number of days spent delirious during the ICU stay, even in patients with no prior cognitive impairment. The severity of cognitive impairment in many survivors resembled that of mild-to-moderate Alzheimer's disease.
Delirium prevention through multicomponent non-pharmacological programs, early mobility, optimization of sedation, and treatment of precipitants remains the most impactful intervention. When delirium does occur, prompt identification of the underlying cause and early non-pharmacological management reduce its duration and mitigate long-term consequences. Systematic delirium screening using validated tools (CAM, CAM-ICU) at least once per shift in high-risk patients transforms delirium from a hidden complication to a recognized, addressable medical problem.
Back to Table of ContentsKey Research Papers
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: The Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. PMID: 2240918. Development and validation of the CAM instrument (sensitivity 94–100%, specificity 90–95%); the foundational diagnostic tool for delirium.
- Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–676. PMID: 10053175. Landmark RCT of the HELP protocol; 40% relative risk reduction in incident delirium.
- Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: Validity and reliability of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). JAMA. 2001;286(21):2703–2710. PMID: 11730446. Validated the CAM-ICU for nonverbal ICU patients; specificity 93–100%.
- Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–1316. PMID: 24088092. BRAIN-ICU study: delirium duration linearly predicted 3- and 12-month cognitive impairment resembling dementia in ICU survivors.
- Hope AA, Abuelo A, Cai X, et al. (MIND-USA Investigators). Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N Engl J Med. 2018;379(26):2506–2516 — Search PubMed. MIND-USA trial: neither haloperidol nor ziprasidone improved survival, delirium-free days, or functional outcomes in ICU patients versus placebo.
- Devlin JW, Skrobik Y, Gélinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med. 2018;46(9):e825–e873. PMID: 30113379. Society of Critical Care Medicine PADIS guidelines; comprehensive evidence-based framework for ICU delirium prevention.
- Shehabi Y, Riker RR, Bokesch PM, et al. Delirium duration and mortality in lightly sedated mechanically ventilated ICU patients. Crit Care Med. 2010;38(12):2311–2318 — Search PubMed. Each additional day of delirium independently increased hazard of death at 1 year by 10%.
- van den Boogaard M, Schoonhoven L, Evers AW, et al. Delirium in critically ill patients: Impact on long-term health-related quality of life and cognitive functioning. Crit Care Med. 2012;40(1):112–118 — Search PubMed. Delirium in ICU independently reduced health-related QoL and cognitive function at 18 months.
- Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs Midazolam for Sedation of Critically Ill Patients: A Randomized Trial. JAMA. 2009;301(5):489–499. PMID: 19188334. SEDCOM trial: dexmedetomidine reduced delirium prevalence and time to extubation vs. midazolam in ICU patients.
- Fong TG, Davis D, Growdon ME, Albuquerque A, Inouye SK. The interface between delirium and dementia in elderly adults. Lancet Neurol. 2015;14(8):823–832 — Search PubMed. Comprehensive review of bidirectional delirium-dementia relationship; shared pathophysiology and long-term cognitive consequences.
- Marcantonio ER, Flacker JM, Wright RJ, Resnick NM. Reducing delirium after hip fracture: A randomized trial. J Am Geriatr Soc. 2001;49(5):516–522. PMID: 11380742. Geriatric consultation reduced delirium incidence by 36% and severe delirium by 40% after hip fracture repair.
- Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. PMID: 23992774. Landmark comprehensive review of delirium epidemiology, pathophysiology, prevention, and treatment; essential reference.
Connections
- Neurology
- Wernicke-Korsakoff Syndrome
- Dementia
- Alzheimer's Disease
- Encephalitis
- Huntington's Disease
- Epilepsy
- Meningitis
- Thiamine (Vitamin B1)