Essential Thrombocythemia
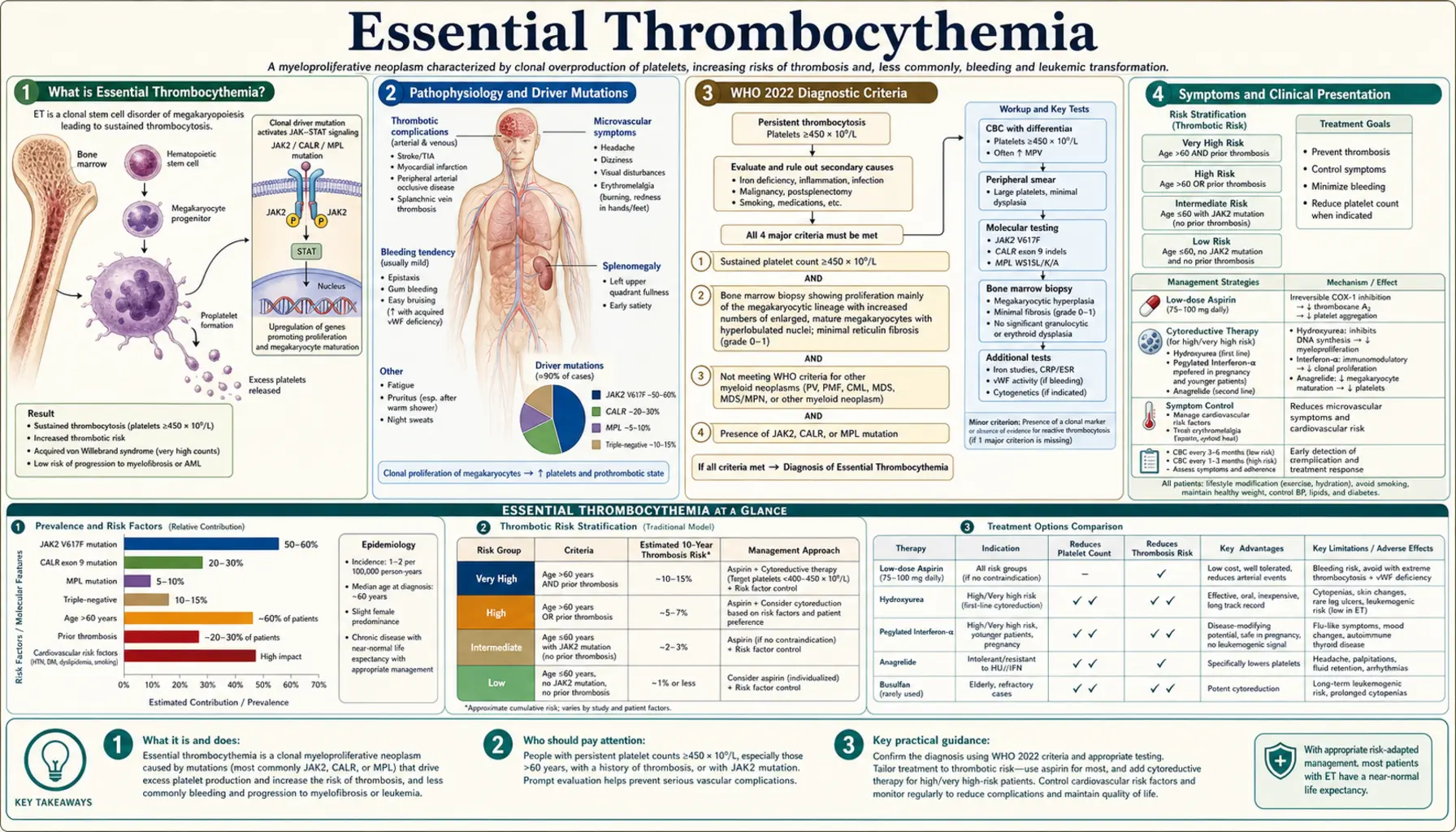
Table of Contents
- What is Essential Thrombocythemia?
- Pathophysiology and Driver Mutations
- WHO 2022 Diagnostic Criteria
- Symptoms and Clinical Presentation
- Thrombosis and Bleeding Risk
- Risk Stratification (IPSET-Thrombosis Revised)
- Treatment Approach
- Prognosis and Disease Progression
- Research Papers
- Connections
- Featured Videos
What is Essential Thrombocythemia?
Essential Thrombocythemia (ET) is a clonal hematopoietic stem cell disorder belonging to the Philadelphia chromosome-negative myeloproliferative neoplasms (MPNs), characterized by sustained thrombocytosis with a platelet count persistently at or above 450 × 109/L. It is the second most common MPN after polycythemia vera, and carries a relatively benign course compared to other MPNs — yet the major risks of thrombosis and hemorrhage can significantly affect quality of life and longevity.
The annual incidence is approximately 1–2.5 per 100,000 persons per year. ET shows a bimodal age distribution: a younger peak in women during their 30s (possibly reflecting hormonal influences on clonal expansion) and a larger peak in both sexes during their 50s and 60s. Most patients have a sustained normal life expectancy with appropriate management. The principal long-term risks are thrombosis, hemorrhage, progression to post-ET myelofibrosis (10–20% at 15–20 years), and — less commonly — transformation to acute myeloid leukemia (AML, fewer than 5%).
Pathophysiology and Driver Mutations
ET arises from an acquired somatic mutation in a multipotent hematopoietic stem cell that drives constitutive activation of the JAK-STAT signaling pathway, resulting in excessive megakaryocyte proliferation and platelet production. Three principal driver mutations account for approximately 83% of ET cases:
JAK2 V617F (approximately 55% of ET)
A point mutation (valine-to-phenylalanine substitution at codon 617) in the pseudo-kinase domain of Janus kinase 2. This mutation disables the autoinhibitory JH2 domain, causing constitutive JAK2 kinase activity and continuous downstream STAT3/STAT5 signaling independent of thrombopoietin (TPO) or erythropoietin binding. JAK2-mutated ET carries a higher risk of arterial thrombosis, higher red blood cell and white blood cell counts, and greater polycythemia vera-like features than other mutation subtypes.
CALR Exon 9 Mutations (approximately 25% of ET)
Insertions or deletions in exon 9 of the calreticulin gene create a frameshift producing a novel mutant C-terminus. This abnormal calreticulin protein binds and activates the thrombopoietin receptor MPL (myeloproliferative leukemia protein) in a ligand-independent manner, driving megakaryocyte expansion. Two main types exist: Type 1 (52-bp deletion) and Type 2 (5-bp insertion). CALR-mutated ET has a lower thrombosis risk compared to JAK2-mutated ET but a somewhat higher long-term risk of transformation to post-ET myelofibrosis. Prognosis hierarchy for thrombosis risk: JAK2 V617F > CALR type 1 > CALR type 2 > MPL.
MPL W515L/K Mutations (approximately 3% of ET)
Activating mutations in codon 515 of the thrombopoietin receptor gene (MPL) directly activate the receptor without ligand binding, producing constitutive JAK-STAT pathway signaling and megakaryocytic hyperplasia similar to JAK2 V617F.
Triple-Negative ET (approximately 17%)
Patients lacking JAK2, CALR, and MPL mutations. Some harbor mutations in other signaling genes (e.g., SH2B3). Diagnosis requires strict exclusion of reactive thrombocytosis and other myeloid neoplasms; bone marrow biopsy is particularly important in this group.
Driver mutations alone are insufficient to cause ET — the defining bone marrow finding is megakaryocyte hyperplasia with characteristic large, mature megakaryocytes featuring hyperlobated ("staghorn") nuclei and loose clustering, without significant granulocyte or erythrocyte proliferation.
WHO 2022 Diagnostic Criteria
The 2022 WHO Classification of Haematolymphoid Tumours requires all four major criteria, or the first three major criteria plus the one minor criterion, for a diagnosis of ET:
Major Criteria
- Platelet count ≥450 × 109/L on two measurements at least 4 weeks apart.
- Bone marrow biopsy showing megakaryocyte hyperplasia with large, mature megakaryocytes with hyperlobated (staghorn) nuclei; no significant increase in neutrophil granulopoiesis or erythropoiesis; very rarely increased reticulin fibrosis (grade 1).
- Not meeting WHO criteria for BCR-ABL1-positive chronic myeloid leukemia (CML), polycythemia vera (PV), primary myelofibrosis (PMF), myelodysplastic syndrome (MDS), or other myeloid neoplasm.
- Presence of a JAK2 V617F, CALR, or MPL mutation.
Minor Criterion
- Presence of a clonal marker (e.g., abnormal karyotype by conventional cytogenetics) OR absence of evidence of reactive thrombocytosis.
Reactive Thrombocytosis: Mimics to Exclude
Before diagnosing ET, common causes of secondary (reactive) thrombocytosis must be ruled out, as reactive platelet elevation rarely causes thrombotic complications:
- Iron deficiency anemia (most common cause of thrombocytosis in young women)
- Acute or chronic infection and inflammation (IL-6 drives hepatic TPO production)
- Post-splenectomy state (loss of platelet sequestration)
- Tissue damage, surgery, or trauma (acute phase response)
- Rebound thrombocytosis following recovery from thrombocytopenia
- Certain malignancies producing inflammatory cytokines
Symptoms and Clinical Presentation
Approximately 50% of ET patients are asymptomatic at diagnosis, with the condition discovered incidentally on a routine complete blood count. When symptoms are present, they generally fall into two categories: microvascular disturbances and major thrombohemorrhagic events.
Microvascular Symptoms
- Erythromelalgia: Burning, aching pain with redness and warmth of the hands and feet, caused by platelet-mediated arteriolar occlusion of small vessels. Dramatically and rapidly responsive to aspirin — one of the most specific features of ET among MPNs.
- Headaches and dizziness: Due to impaired microvascular circulation in cerebral vessels; often relieved by aspirin.
- Visual disturbances: Transient scotomas, blurred vision, or amaurosis fugax from ocular microvascular platelet plugging.
- Paresthesias: Tingling or numbness in hands and feet from peripheral microvascular platelet-mediated ischemia.
- Aquagenic pruritus: Itching triggered by water contact; less common in ET than in polycythemia vera.
Splenomegaly
Present in approximately 40% of ET patients. Usually mild to moderate; massive splenomegaly suggests progression toward post-ET myelofibrosis.
Thrombotic Events
Arterial and venous thromboses are the leading causes of morbidity and mortality in ET. Arterial events are more common than in other MPNs and include stroke and TIA, myocardial infarction, and peripheral arterial occlusion. Venous events include deep vein thrombosis, pulmonary embolism, and splanchnic vein thrombosis (Budd-Chiari syndrome, portal vein thrombosis, mesenteric vein thrombosis).
Hemorrhagic Manifestations
Paradoxically, marked thrombocytosis (platelets >1,000–1,500 × 109/L) can cause bleeding rather than clotting, because very high platelet numbers lead to excessive binding and proteolytic degradation of large von Willebrand factor (vWF) multimers by ADAMTS13 — a condition called acquired von Willebrand syndrome. Loss of these high-molecular-weight vWF multimers impairs platelet adhesion, and bleeding ensues despite the very high platelet count. Manifestations include gastrointestinal bleeding, epistaxis, easy bruising, and mucosal hemorrhage.
Pregnancy Complications
ET poses specific risks during pregnancy, including first-trimester miscarriage (placental microthrombi), placental insufficiency, fetal growth restriction, preeclampsia, and postpartum thrombosis.
Thrombosis and Bleeding Risk
Understanding the dual thrombotic and hemorrhagic risk in ET is essential for guiding therapy. The relationship between platelet count and clinical events is not strictly linear, and individual mutation profile strongly modulates risk.
Arterial vs. Venous Thrombosis
Arterial thrombosis predominates in ET (particularly in JAK2-mutated patients), in contrast to venous predominance in PV. The excess of reactive oxygen species from JAK2 V617F platelets activates endothelial cells and promotes platelet-leukocyte aggregates. Major arterial events include ischemic stroke and TIA, myocardial infarction, and peripheral arterial occlusion. Major venous events include DVT/PE and splanchnic vein thrombosis — the latter can be the initial manifestation of an underlying MPN in young patients presenting with Budd-Chiari syndrome or portal vein thrombosis.
Acquired von Willebrand Syndrome
When platelet counts exceed 1,000 × 109/L, screen for acquired vWF deficiency before starting aspirin. If vWF ristocetin cofactor activity falls below 30% of normal, aspirin is contraindicated due to bleeding risk. Cytoreductive therapy normalizing the platelet count reverses the acquired vWD and restores high-molecular-weight vWF multimers — eliminating the hemorrhagic risk.
Cardiovascular Risk Factors
Traditional cardiovascular risk factors (hypertension, diabetes, hyperlipidemia, smoking, obesity) synergize powerfully with ET-related platelet activation to increase arterial thrombosis risk. Aggressive management of modifiable cardiovascular risk factors is a core component of ET care independent of cytoreductive therapy decisions.
Risk Stratification (IPSET-Thrombosis Revised)
The Revised International Prognostic Score for ET Thrombosis (IPSET-Thrombosis Revised) categorizes patients into three risk groups to guide cytoreductive treatment decisions. The revised model incorporates JAK2 mutation status — a significant advance over earlier age-only models:
Low Risk
- Age <60 years AND
- No prior thrombosis AND
- No cardiovascular risk factors AND
- JAK2 V617F mutation absent (CALR- or MPL-mutated, or triple-negative)
Management: Observation alone or low-dose aspirin for microvascular symptoms. Cytoreductive therapy not indicated.
Intermediate Risk
- Age <60 years AND
- No prior thrombosis AND
- JAK2 V617F mutation present OR cardiovascular risk factors present
Management: Low-dose aspirin (and aggressive cardiovascular risk factor modification). Cytoreduction is considered in patients with additional risk features or progressive microvascular symptoms refractory to aspirin.
High Risk
- Age ≥60 years OR
- Prior thrombosis (arterial or venous) at any age
Management: Cytoreductive therapy plus low-dose aspirin (unless contraindicated by acquired vWD or prior hemorrhage).
Treatment Approach
Treatment goals in ET are to prevent thrombotic and hemorrhagic complications, control microvascular symptoms, and minimize the small risk of disease transformation. Cure is not achievable with current therapies except potentially with allogeneic stem cell transplantation, which is rarely indicated in ET given its relatively indolent course.
Aspirin in All Risk Groups
Low-dose aspirin (81–100 mg/day) is recommended for virtually all ET patients unless specifically contraindicated. Aspirin inhibits thromboxane A2-mediated platelet activation and reliably resolves erythromelalgia and microvascular symptoms. Critical exception: Screen vWF activity before aspirin initiation when platelet count exceeds 1,000 × 109/L. If vWF ristocetin cofactor activity is below 30%, aspirin is contraindicated and cytoreduction to normalize the platelet count takes precedence.
Cytoreductive Therapy: First-Line Options
Hydroxyurea (Hydroxycarbamide)
First-line cytoreductive therapy for high-risk ET. The landmark PT-1 trial (Harrison et al., 2005) demonstrated that hydroxyurea plus aspirin significantly reduced major thrombotic events compared to anagrelide plus aspirin (3.6% vs 8.8% major arterial events at 5 years). Hydroxyurea suppresses DNA synthesis in all rapidly dividing cells, including megakaryocyte progenitors. Typical dosing: 500–1,000 mg/day titrated to platelet count target (typically <400 × 109/L). Long-term use in young patients is avoided due to theoretical leukemogenic risk and teratogenicity.
Pegylated Interferon-Alpha (pegIFN-α2a)
Preferred cytoreductive agent for young patients (<40 years), patients of childbearing potential, or those who are pregnant or planning pregnancy (hydroxyurea is teratogenic and contraindicated). PegIFN-α2a directly suppresses clonal hematopoiesis at the stem cell level. A unique advantage is the potential for molecular remission — reduction or elimination of the JAK2 V617F or CALR allele burden — which is not achievable with hydroxyurea. Molecular responses occur in 15–30% of patients treated for several years. Tolerability is improved versus standard interferon, but side effects (fatigue, depression, autoimmune phenomena) still limit use.
Anagrelide
Reduces platelet count by inhibiting megakaryocyte maturation (platelet production is selectively impaired). However, the PT-1 trial demonstrated anagrelide is inferior to hydroxyurea for high-risk ET: the anagrelide arm had significantly more arterial thrombotic events, more episodes of myelofibrotic transformation, and more bleeding complications. Anagrelide is now reserved for patients who are intolerant of or refractory to both hydroxyurea and pegIFN. Cardiovascular side effects (palpitations, fluid retention) due to its vasodilatory/inotropic properties require attention in older patients.
Second-Line and Special Situations
- Busulfan: An alkylating agent that provides durable platelet control in elderly patients; not used in younger patients due to leukemogenicity. Well-tolerated in patients over 70.
- Ruxolitinib (JAK1/JAK2 inhibitor): Used for hydroxyurea-resistant or hydroxyurea-intolerant ET; reduces splenomegaly and constitutional symptoms via JAK pathway blockade. Not curative; disease rebounds on discontinuation.
- Pregnancy management: Low-dose aspirin throughout pregnancy; cytoreduction with pegIFN-α2a if cytoreduction is required (hydroxyurea, busulfan, and anagrelide are all contraindicated during pregnancy). Low molecular weight heparin added peripartum for high-risk patients. Close obstetric monitoring for placental complications.
Prognosis and Disease Progression
The natural history of ET is generally favorable compared to other MPNs. Many low-risk patients have a near-normal life expectancy. The 10-year overall survival is approximately 80%, with most deaths related to cardiovascular complications, thrombosis, or transformation rather than to ET-specific disease burden.
Disease Transformation
- Post-ET Myelofibrosis: Occurs in approximately 10–20% of patients at 15–20 years of follow-up (fibrotic progression, splenomegaly, constitutional symptoms, cytopenias). Post-ET MF has worse prognosis than ET but better prognosis than primary myelofibrosis. CALR mutations, particularly type 1, carry a somewhat higher transformation risk than JAK2.
- Acute Myeloid Leukemia (AML): Blastic transformation occurs in fewer than 5% of ET patients and is significantly more likely in those who receive alkylating agents (busulfan, pipobroman) or radioactive phosphorus — now avoided in younger patients for this reason. Spontaneous AML transformation is rare in ET, lower than in MDS or PV.
Prognostic Factors
- Mutation type: JAK2 V617F confers higher thrombosis risk; CALR type 1 has the longest median survival and lowest thrombosis risk. Triple-negative ET carries intermediate prognosis.
- Age and prior thrombosis: The two strongest independent predictors of future thrombotic events and overall survival.
- White blood cell count: Leukocytosis (WBC >11 × 109/L) is an emerging independent risk factor for thrombosis and overall survival in several cohort studies.
- IPSS-ET score: Incorporates age, WBC count, and prior thrombosis to stratify overall survival risk separate from thrombosis risk.
Research Papers
The following PubMed links point to pivotal peer-reviewed studies on essential thrombocythemia, covering clinical trials, molecular pathogenesis, diagnostic criteria, and risk stratification.
- Search PubMed
- Search PubMed
- Klampfl et al. (2013) Somatic CALR mutations in MPNs — PMID 24325356
- Nangalia et al. (2013) CALR mutations in ET and myelofibrosis — PMID 24325359
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Hematology
- Polycythemia Vera
- Primary Myelofibrosis
- Myelodysplastic Syndrome
- Acute Myeloid Leukemia
- Thrombocytopenia
- Deep Vein Thrombosis
- Disseminated Intravascular Coagulation
- Anemia
- Complete Blood Count
- Hemophilia
- Atrial Fibrillation
- Stroke