Ulcerative Colitis: History and Discovery
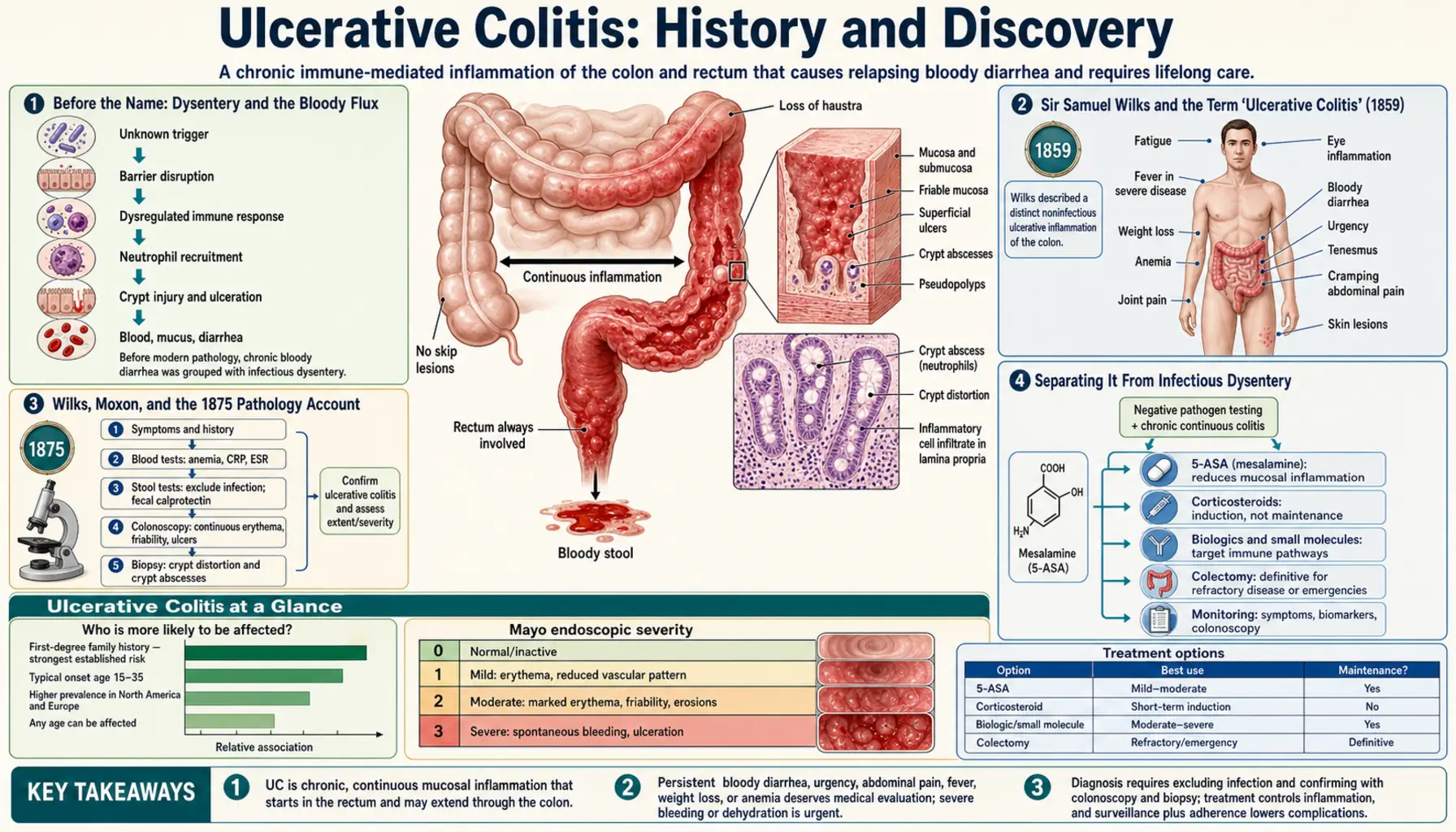
For most of recorded history, bloody diarrhea simply meant "dysentery" — an infection to be survived or not. The story of ulcerative colitis is the slow, difficult work of pulling one disease out of that crowd: recognizing that some people develop chronic, relapsing inflammation and ulceration of the colon with no germ behind it. The London physician Sir Samuel Wilks is credited with first using the term "ulcerative colitis" in 1859, and with Walter Moxon gave a fuller account in their 1875 pathology textbook. It would take the bacteriology of the 1890s to separate it cleanly from infectious dysentery, the year 1932 to define Crohn's disease as a related-but-distinct illness, and Swedish researcher Nanna Svartz in the 1940s to find the first reliably effective drug. The fundamental cause is still unknown — but unlike Crohn's, ulcerative colitis can be cured by removing the colon.
Table of Contents
- Before the Name: Dysentery and the Bloody Flux
- Sir Samuel Wilks and the Term "Ulcerative Colitis" (1859)
- Wilks, Moxon, and the 1875 Pathology Account
- Separating It From Infectious Dysentery
- Crohn 1932 and the Birth of the IBD Concept
- Sulfasalazine, Cortisone, and the First Effective Drugs
- Surgery and the Curative Colectomy
- A Cause Still Unknown
- Research Papers and References
- Connections
- Featured Videos
Before the Name: Dysentery and the Bloody Flux
Bloody diarrhea is one of the oldest recorded human afflictions, and for thousands of years it had a single name: dysentery, the "bloody flux." Greek, Roman, medieval, and early-modern physicians described patients wasting away from frequent stools streaked with blood and mucus, but they had no way to tell the difference between an acute infection and a chronic, non-infectious inflammation of the bowel. The two looked and felt the same at the bedside: cramping, urgency, fever, blood, and exhaustion. Some historians have wondered whether certain famous historical cases of chronic flux were in fact what we would now call ulcerative colitis, but without tissue examination or microbiology such retrospective diagnoses can never be confirmed, and this page does not claim them as fact.
The obstacle was conceptual as much as technical. Until the germ theory of disease took hold in the second half of the nineteenth century, there was no framework in which to ask whether a given case of bloody flux was caused by an invading organism or by the body inflaming its own colon for no apparent reason. The colon could only be examined after death, and even then a chronically ulcerated bowel could be read as the aftermath of a severe infection rather than a disease in its own right. Pulling a distinct, idiopathic "ulcerative colitis" out of the broad category of dysentery required both better pathology and a new way of thinking — and that is what began to happen in mid-nineteenth-century London.
Sir Samuel Wilks and the Term "Ulcerative Colitis" (1859)
Sir Samuel Wilks (1824–1911), a physician and pathologist at Guy's Hospital in London, is the figure most consistently credited with first using the term "ulcerative colitis," in 1859. The case that prompted it was a woman who died after months of diarrhea and fever; at autopsy Wilks found extensive ulceration and inflammation of the colon that he judged was not the result of an ordinary dysenteric infection. He described it as a "simple ulcerative colitis" — simple meaning, in the language of the day, not caused by a recognized contagion. The conceptual leap mattered more than the wording: Wilks was proposing that inflammation and ulceration of the large bowel could be a condition in itself, not merely the scar of a passing infection.
An important and honest caveat belongs here. Modern historical reviews note that the specific 1859 case Wilks described — which involved inflammation extending into the terminal ileum — may actually have been closer to what we now call Crohn's disease than to ulcerative colitis as currently defined. In other words, Wilks coined the term for a case that, by today's stricter criteria, might be reclassified. This does not diminish his priority for the name or for the underlying idea of a non-infectious inflammatory colitis; it simply reflects that the modern distinction between ulcerative colitis and Crohn's disease did not yet exist, and would not for another seventy years. Wilks himself went on to a distinguished career, was knighted, and is remembered for several other "firsts" in pathology.
Wilks, Moxon, and the 1875 Pathology Account
The more substantial and frequently cited description came in 1875, when Wilks, together with his Guy's Hospital colleague Walter Moxon (1836–1886), published a fuller account in their influential textbook Lectures on Pathological Anatomy. There they documented ulceration and inflammation involving the entire colon in a young woman who had died of severe bloody diarrhea — a case that aligns much more convincingly with ulcerative colitis as it is understood today. For this reason a number of historical sources credit the 1875 Wilks-and-Moxon description, rather than the 1859 note, as the founding clinical-pathological account of the disease. Both dates appear in the literature, which is why this page presents the nuance plainly: the term traces to Wilks in 1859, while the classic pathological description is the joint 1875 work.
The Wilks-and-Moxon account did something the older dysentery literature could not: it tied a clinical picture (chronic, relapsing, bloody diarrhea in an otherwise non-infected patient) to a consistent pathological finding (continuous ulceration of the colonic mucosa). Over the following decades, English physicians built on this foundation. William Henry Allchin reported cases in 1885, and Sir William Hale-White published a series at Guy's Hospital in 1888 of diarrheal cases that could not be attributed to any infectious cause. From roughly that point onward, "ulcerative colitis" entered the medical vocabulary as the accepted name for this idiopathic inflammatory disease of the large bowel.
Separating It From Infectious Dysentery
Naming the disease was one thing; reliably telling it apart from infectious dysentery at the bedside was another, and it remained genuinely difficult for decades. The breakthrough came not from gastroenterology but from microbiology. In 1897 the Japanese bacteriologist Kiyoshi Shiga identified the dysentery bacillus — the organism now named Shigella in his honor — as the cause of epidemic bacillary dysentery. At about the same time, the protozoan parasite Entamoeba histolytica was established as the cause of amoebic dysentery. For the first time, physicians had laboratory tests that could detect a specific pathogen in a patient's stool.
This changed everything for ulcerative colitis. A patient with chronic bloody diarrhea could now be tested for the dysentery bacillus and for amoebae; when those tests came back negative again and again, what remained was, by exclusion, an idiopathic inflammatory colitis — ulcerative colitis. In effect, the disease was defined as much by what it was not (not Shigella, not amoebic, not tuberculous) as by what it was. This diagnosis-by-exclusion remained central well into the twentieth century, and a version of it persists today: even now, confirming ulcerative colitis requires ruling out infectious causes of colitis before the chronic, immune-driven disease can be diagnosed with confidence.
It is worth being precise about three separate questions that the history kept tangled together: naming the disease (Wilks, 1859; Wilks and Moxon, 1875), separating it from infectious dysentery (made possible by the bacteriology of the 1890s), and identifying its cause (still unresolved). Progress on the first two did not deliver the third, and conflating them is a common error in popular accounts. Ulcerative colitis could be named and even diagnosed long before anyone understood why it happens.
Crohn 1932 and the Birth of the IBD Concept
The next great clarification came in 1932, when the American gastroenterologist Burrill B. Crohn, together with the pathologist Leon Ginzburg and surgeon Gordon D. Oppenheimer, published their landmark paper on "regional ileitis" at Mount Sinai Hospital in New York, describing a chronic inflammatory disease of the terminal ileum as a distinct clinical and pathological entity. This condition became known as Crohn's disease. Its recognition was pivotal for ulcerative colitis precisely because it forced physicians to ask a sharper question: among patients with chronic intestinal inflammation, which had ulcerative colitis and which had Crohn's? The two are related but genuinely different diseases, and distinguishing them became — and remains — one of the central tasks of the field.
Out of this grew the unifying concept of inflammatory bowel disease (IBD), an umbrella term covering ulcerative colitis and Crohn's disease as the two major chronic, idiopathic inflammatory diseases of the gut. The distinctions sharpened over the mid-twentieth century: ulcerative colitis was understood to involve continuous, superficial inflammation limited to the colon and rectum, always starting at the rectum and extending proximally, affecting only the inner lining (mucosa). Crohn's disease, by contrast, can strike anywhere from mouth to anus, tends to appear in patchy "skip" lesions, and penetrates the full thickness of the bowel wall. Recognition that Crohn's disease could also affect the colon (Crohn's colitis) — established through reports by Lockhart-Mummery and Morson around 1959–1960 — further complicated and refined the separation.
This distinction is not academic. It drives prognosis, the choice and duration of drug therapy, cancer-surveillance strategy, and — most dramatically — whether surgery can cure the disease, as discussed below. On this site, ulcerative colitis, Crohn's disease, and the shared inflammatory bowel disease framework are covered on dedicated pages.
Sulfasalazine, Cortisone, and the First Effective Drugs
For its first eighty years as a named disease, ulcerative colitis had no specific drug treatment — only rest, diet, and supportive care. The first reliably effective medication arrived through one of medicine's memorable accidents. In the early 1940s the Swedish physician Nanna Svartz (1890–1986) — the first woman to hold a professorial chair in medicine in Sweden, at the Karolinska Institute — worked with the Pharmacia company to create a compound that linked a sulfonamide antibiotic (sulfapyridine) to a salicylate (an aspirin-like anti-inflammatory) by an azo bond. The drug, salicylazosulfapyridine, was marketed as Salazopyrin and is known generically as sulfasalazine; it was registered in Sweden in 1941.
Svartz had designed the drug to treat rheumatoid arthritis, reasoning that an agent combining anti-infective and anti-inflammatory actions might help. Observing that the inflamed tissue in ulcerative colitis resembled the inflamed joint lining of arthritis, she tried sulfasalazine in colitis patients — and found it strikingly effective at calming the bowel. Decades later it was shown that the active anti-inflammatory component delivered to the colon is 5-aminosalicylic acid (5-ASA, mesalazine), the salicylate half of the molecule, which is released by gut bacteria splitting the azo bond. The 5-ASA class remains a first-line therapy for mild-to-moderate ulcerative colitis to this day, and sulfasalazine appears on the World Health Organization's list of essential medicines.
The second pillar of medical therapy followed soon after. In 1955, the Oxford physicians Sidney Truelove and Leslie Witts published a landmark trial in the British Medical Journal showing that cortisone (a corticosteroid) significantly outperformed placebo at inducing remission and reducing mortality in ulcerative colitis. This study is widely regarded as one of the first randomized controlled trials in gastroenterology, and the severity criteria Truelove and Witts devised to grade an attack of colitis are still used by clinicians nearly seventy years later. Corticosteroids became, and remain, the workhorse for bringing a severe flare under control — later joined by immunomodulators and, from the late 1990s onward, biologic therapies such as anti-TNF agents.
Surgery and the Curative Colectomy
Because ulcerative colitis is confined to the colon and rectum, surgeons recognized early that removing the diseased bowel could, in principle, end the disease. Operative attempts were recorded from around 1900, beginning with palliative measures — appendicostomy (creating an opening through the appendix to irrigate the colon), promoted by physicians such as Robert Weir and championed in Britain by Sir Arthur Hurst — and progressing to diverting ileostomy and, eventually, full removal of the colon. The decisive principle is simple and remains true: because the disease never extends beyond the large bowel, removing the entire colon and rectum (proctocolectomy) cures ulcerative colitis. This is one of the most important practical differences between the two main inflammatory bowel diseases — surgery is not curative for Crohn's disease, which can recur in any remaining segment of the gut, but it is curative for ulcerative colitis.
For much of the twentieth century, "cure" came at the cost of a permanent ileostomy and an external bag, a hard trade-off that many patients understandably resisted until illness forced their hand. Surgery also became life-saving in the setting of toxic megacolon — a dangerous, sometimes fatal complication in which a severely inflamed colon balloons and risks perforation — and in the prevention or treatment of the colorectal cancer that long-standing extensive colitis can cause. In these situations, timely colectomy is not a last resort but a rescue.
The major quality-of-life advance came in 1978, when the London surgeons Sir Alan Parks and John Nicholls described restorative proctocolectomy with ileal pouch–anal anastomosis (IPAA). Instead of a permanent stoma, the surgeon fashions an internal reservoir (a "pouch") from the patient's own small intestine and connects it to the anus, preserving the natural route of defecation. The design was refined — notably into the widely used J-shaped pouch by Utsunomiya around 1980 — and IPAA became the modern standard for patients needing surgery who wish to avoid a permanent ileostomy. Surgery thus offers something almost unique among chronic inflammatory diseases: a genuine, definitive cure.
A Cause Still Unknown
Despite more than 160 years of study, the fundamental cause of ulcerative colitis remains unknown — and intellectual honesty requires saying so plainly. From the late nineteenth century onward, investigators searched hard for a responsible microbe (various bacteria such as Bacillus coli, streptococci, and diplostreptococci were proposed), but none ever satisfied Koch's postulates, the formal criteria for proving an organism causes a disease. The infectious-cause hypothesis, attractive as it was, was never confirmed and is not the accepted explanation today. It is correctly described as a historical hypothesis, not an established fact.
The modern understanding is that ulcerative colitis is a multifactorial disease: it arises from an interaction of genetic susceptibility, a dysregulated immune response, the gut microbiome (the community of bacteria living in the colon), and environmental triggers. Dozens of genetic risk loci have been identified, the disease clusters in families, and a striking environmental observation is that ulcerative colitis is, unusually, more common in non-smokers and former smokers than in current smokers — the reverse of Crohn's disease. But no single gene, germ, food, or exposure has been shown to cause the disease, and the precise sequence of events that tips a susceptible person into chronic colonic inflammation is not yet understood. Researchers describe it as a breakdown in the normal tolerance between the immune system and the trillions of microbes in the gut, but the trigger remains unresolved.
This is the honest state of the science, and it shapes how the disease is treated. Because the root cause is unknown, medical therapy aims to control inflammation and maintain remission rather than to cure — while surgical removal of the colon, by eliminating the target organ entirely, sidesteps the unsolved question of cause and provides a definitive cure. The history of ulcerative colitis is therefore a history of remarkable practical progress — in naming, in distinguishing, in treating, and in curing by surgery — built atop a central mystery that medicine has not yet solved.
Research Papers and References
The references below combine peer-reviewed historical reviews of ulcerative colitis and inflammatory bowel disease with the landmark therapeutic trials named in the article, plus curated PubMed topic-search links into the historical literature. The nineteenth-century primary texts (Wilks' 1859 case, Wilks and Moxon's 1875 Lectures on Pathological Anatomy) are named in the article as historical sources rather than as modern citations. Each external link opens in a new tab.
- Mulder DJ, Noble AJ, Justinich CJ, Duffin JM. A tale of two diseases: the history of inflammatory bowel disease. Journal of Crohn's and Colitis. 2014;8(5):341–348. — doi:10.1016/j.crohns.2013.09.009
- Kirsner JB. Historical origins of current IBD concepts. World Journal of Gastroenterology. 2001 / reprint 2016. — PMC4723519
- Baumgart DC, Carding SR. Inflammatory bowel disease: cause and immunobiology. The Lancet. 2007;369(9573):1627–1640. — doi:10.1016/S0140-6736(07)60750-8
- Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on a therapeutic trial. British Medical Journal. 1955;2(4947):1041–1048. — doi:10.1136/bmj.2.4947.1041
- Crohn BB, Ginzburg L, Oppenheimer GD. Regional ileitis: a pathologic and clinical entity. Journal of the American Medical Association. 1932;99(16):1323–1329. — doi:10.1001/jama.1932.02740680019005
- Svartz N. Salazopyrin, a new sulfanilamide preparation. Acta Medica Scandinavica. 1942;110(6):577–598. — doi:10.1111/j.0954-6820.1942.tb06841.x
- Nanna Svartz (1890–1986) and the discovery of sulfasalazine — historical review. — PubMed: Nanna Svartz and sulfasalazine history
- Parks AG, Nicholls RJ. Proctocolectomy without ileostomy for ulcerative colitis. British Medical Journal. 1978;2(6130):85–88. — doi:10.1136/bmj.2.6130.85
- Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. The Lancet. 2017;389(10080):1756–1770. — doi:10.1016/S0140-6736(16)32126-2
- History of inflammatory bowel diseases — review (overview of UC and Crohn's milestones). — PMC6912289
- Ulcerative colitis — history and historical perspective. — PubMed: ulcerative colitis history (Wilks, Moxon)
- Restorative proctocolectomy and ileal pouch–anal anastomosis — historical development and current status. — PubMed: ileal pouch–anal anastomosis history
- Ulcerative colitis — etiology, genetics, microbiome, and environment (cause still unresolved). — PubMed: ulcerative colitis etiology and pathogenesis
External Authoritative Resources
- NIDDK (NIH) — Ulcerative Colitis
- Crohn's & Colitis Foundation — What Is Ulcerative Colitis
- PubMed — All research on the history of ulcerative colitis
Connections
- Gastroenterology
- Ulcerative Colitis
- Crohn's Disease
- Inflammatory Bowel Disease (IBD)
- Irritable Bowel Syndrome (IBS)
- Celiac Disease
- All Conditions