Gastroesophageal Reflux Disease (GERD): History and Discovery
The burning chest pain we call heartburn has been described for as long as people have written about the body, but the modern disease — the idea that stomach acid flowing the wrong way damages the esophagus and can be measured, named, and treated — is barely a century old. This page traces that arc: from the ancient symptom, through the pivotal twentieth-century insight that acid reflux causes esophageal inflammation, to the diagnostic tools and the antacid → H2-blocker → proton-pump-inhibitor revolution that transformed care. Where a name, a date, or a “first” could not be confirmed from at least two independent sources, it is flagged plainly rather than asserted.
Table of Contents
- The Ancient Symptom: Heartburn Before the Disease
- Hiatal Hernia and the First Modern Clues (1900–1930)
- Winkelstein and “Peptic Esophagitis” (1935)
- Allison, Hiatal Hernia, and “Reflux Esophagitis” (1940s–50s)
- Barrett and the Columnar-Lined Esophagus (1950)
- The Sphincter and the pH Probe: Measuring Reflux
- From Heartburn to “GERD”: Naming the Disease
- Treatment Milestones: Antacids to Proton Pump Inhibitors
- Legacy and Honest Limits
- Research Papers and References
- Connections
- Featured Videos
The Ancient Symptom: Heartburn Before the Disease
Heartburn is one of the oldest recorded human complaints. The sensation — a hot, rising discomfort behind the breastbone, often worse after a large meal or when lying down — appears in the classical medical literature of Greece and Rome, where physicians such as Galen wrote about cardialgia, a term that confusingly mingled stomach pain and the burning felt near the heart. For most of recorded history the symptom was understood as a disorder of digestion or of the stomach itself, not of a specific organ called the esophagus, and certainly not as a distinct “disease” with a measurable cause.
It is important to draw a clean line here, because the distinction is the whole point of this history. The symptom of heartburn (and of regurgitation, the effortless rise of sour or bitter fluid into the throat) has been described for thousands of years. The concept that this symptom reflects an underlying disease — acid refluxing from the stomach up into the esophagus, inflaming and sometimes ulcerating its lining — is a product of the late nineteenth and twentieth centuries. Ancient writers had the experience; they did not yet have the mechanism, the anatomy, or the name.
Through the medieval and early-modern periods, heartburn remained a familiar but poorly explained nuisance, treated empirically with alkaline substances — chalk, coral, burnt eggshell, and other carbonate-rich materials — that we would now recognize as crude antacids. The genuinely modern story begins only when physicians could look inside the chest and upper digestive tract, connect the burning symptom to a structural and chemical event, and give it its own name.
Hiatal Hernia and the First Modern Clues (1900–1930)
The first genuinely modern threads were pathological and radiological. In 1906 the American pathologist Wilder Tileston published a careful study of what he called “peptic ulcer of the oesophagus,” and he is widely credited in later historical reviews with correctly attributing the ulceration at the lower esophagus to the action of gastric (peptic) juice — in other words, to reflux of stomach contents. Tileston’s work is an early, prescient hint that the burning and ulceration were chemical injuries from the stomach, even though the full clinical picture would not come together for another generation.
Two developments made the rest possible. First, the spread of the rigid esophagoscope — pioneered in the early twentieth century by clinicians including Chevalier Jackson in the United States — let physicians actually see inflammation and ulceration in the living esophagus for the first time. Second, the new technology of X-ray imaging, especially with a barium swallow, let radiologists visualize the stomach slipping up through the diaphragm into the chest, the condition called hiatal hernia.
In 1925 the Baltimore physicians Friedenwald and Feldman are commonly cited as among the first to discuss heartburn and its possible relationship to hiatal hernia, helping to frame reflux symptoms as an anatomical problem rather than a vague dyspepsia. For much of the early twentieth century, the hiatal hernia itself was thought to be the disease — the symptom-producing lesion — a view that the next two decades would substantially revise, shifting the blame from the displaced anatomy to the acid it allowed to escape.
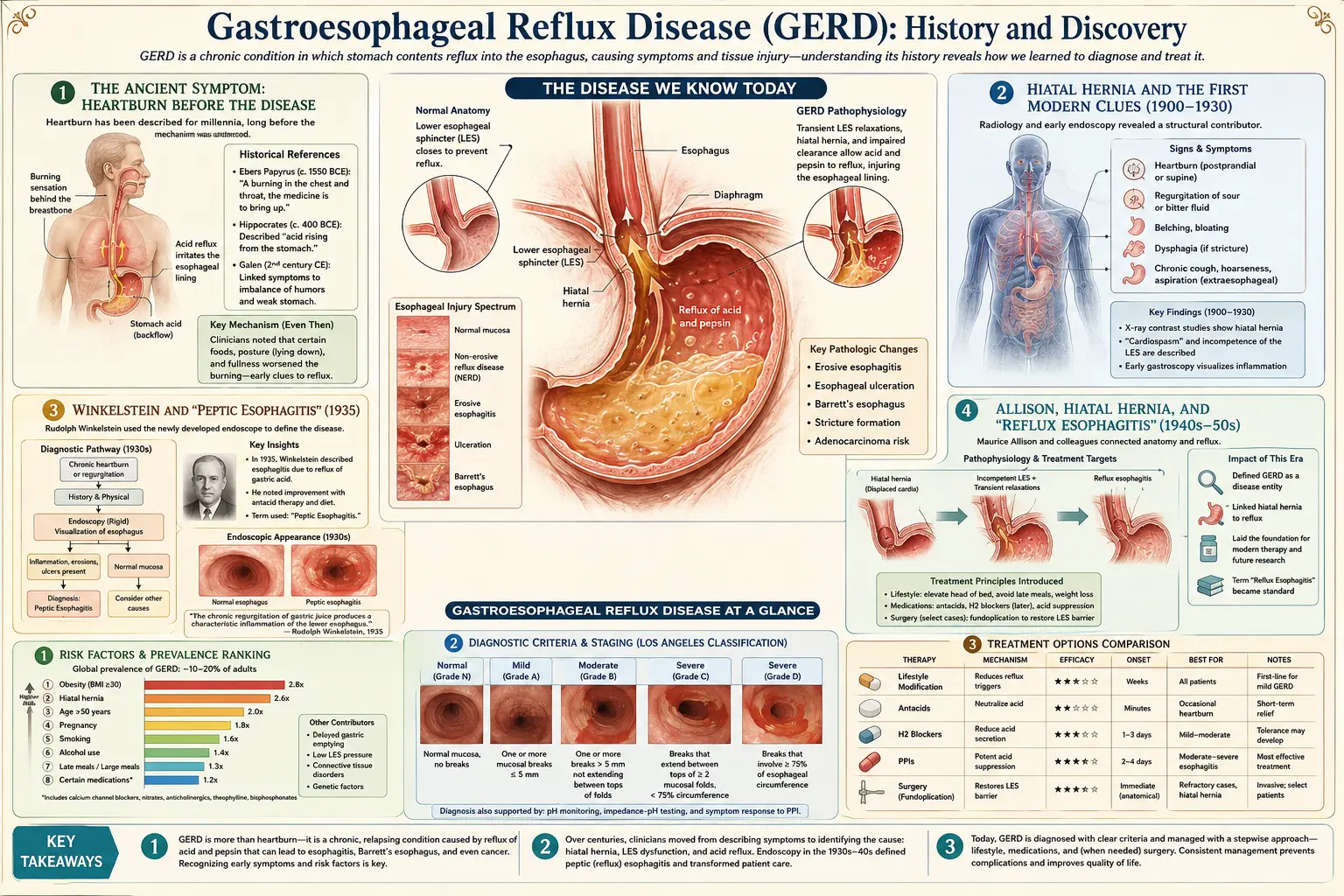
Winkelstein and “Peptic Esophagitis” (1935)
The decisive conceptual step came from the American gastroenterologist Asher Winkelstein. Having presented a small series of cases at the American Medical Association’s annual session in Cleveland in June 1934, he published his landmark paper, Peptic Esophagitis (a new clinical entity), in the Journal of the American Medical Association on 16 March 1935. (The two dates are why some sources cite 1934 and others 1935 — the conference presentation was 1934, the formal publication 1935.) Winkelstein described five patients with severe heartburn and esophageal inflammation and argued that the injury was produced by regurgitated gastric acid and pepsin digesting the lining of the esophagus.
This was the insight that turned a symptom into a disease. By naming the condition “peptic esophagitis,” Winkelstein located the cause squarely in the corrosive action of stomach juice on esophageal tissue — the same “peptic” mechanism already blamed for stomach and duodenal ulcers. It reframed heartburn-with-inflammation as a recognizable clinical entity with an identifiable cause, rather than an obscure complaint of the chest or a mere consequence of a hernia. Note the precise term: Winkelstein coined peptic esophagitis; the closely related phrase reflux esophagitis would be popularized slightly later by others (see the next section).
Winkelstein’s formulation did not win universal or instant acceptance — the relative roles of the hiatal hernia, the acid, and the competence of the lower esophagus would be debated for decades — but the core idea proved durable and correct: acid reflux injures the esophagus. Essentially every later refinement, from sphincter physiology to pH monitoring to acid-suppressing drugs, is built on the foundation Winkelstein laid in the mid-1930s.
Allison, Hiatal Hernia, and “Reflux Esophagitis” (1940s–50s)
If Winkelstein supplied the chemical cause, the British thoracic surgeon Philip Rowland Allison supplied much of the anatomy and the durable vocabulary. Working in the 1940s and 1950s, Allison drew a clear connection between hiatal hernia, the failure of the normal anti-reflux barrier at the gastroesophageal junction, and the resulting acid injury to the esophagus. He is widely credited with coining and popularizing the term “reflux esophagitis” in the late 1940s (commonly dated to 1946–1948 in the historical literature), the phrase that would eventually become the standard description of the inflamed esophagus in reflux disease.
Allison’s contribution was also surgical and demonstrative. With the pathologist A. S. Johnstone, he published in 1953 a series of patients whose lower esophagus was lined by columnar (stomach-type) epithelium, and the pair argued — correctly — that this abnormal lining was esophagus that had undergone change, not displaced stomach. This work directly engaged with, and helped reinterpret, the columnar-lined esophagus that Norman Barrett had described a few years earlier (see below), and it reinforced the central role of reflux as the engine of esophageal damage.
By tying the symptom (heartburn), the cause (acid reflux), the anatomy (an incompetent junction, often with a hiatal hernia), and the tissue injury (esophagitis) into a single coherent picture, Allison and his contemporaries moved the field from Winkelstein’s foundational observation toward the integrated understanding of reflux disease that the second half of the century would formalize and name.
Barrett and the Columnar-Lined Esophagus (1950)
In 1950 the influential London thoracic surgeon Norman Rupert Barrett published a paper on chronic peptic ulcer of the esophagus that addressed a puzzling finding: in some patients, the lower part of what looked like the esophagus was lined not by its usual flat (squamous) cells but by columnar, stomach-like epithelium. Crucially — and this is a point of honest historical nuance — Barrett initially got the interpretation wrong. Because he defined the esophagus by its squamous lining, he argued that this columnar-lined tube must actually be stomach that had been drawn up into the chest, in effect a congenitally short esophagus.
Over the following years this view was overturned, in large part by Allison and Johnstone’s 1953 series and subsequent work, which established that the columnar-lined segment really was esophagus whose lining had changed — a metaplasia driven by chronic acid reflux. By 1957 Barrett himself had accepted the reinterpretation and proposed describing the condition as the “lower oesophagus lined by columnar epithelium.” The eponym “Barrett’s esophagus” came into use thereafter to honor his description of the finding, even though the modern understanding of its cause and significance was supplied by others.
This matters for the GERD story because Barrett’s esophagus is now understood as a complication of long-standing reflux: years of acid exposure can drive the esophageal lining to convert to an intestinal-type epithelium, a change that carries a modestly increased risk of esophageal adenocarcinoma and is the reason chronic reflux is taken seriously and monitored. The 1950 description, and its later correction, are a clean illustration of how the disease’s history advanced — by observation, error, debate, and revision — rather than by a single tidy discovery.
The Sphincter and the pH Probe: Measuring Reflux
For the diagnosis of reflux to become rigorous, two questions had to be answered: what normally keeps stomach contents down, and how can you prove abnormal acid is reaching the esophagus in a given patient. The first was answered by mid-century esophageal physiology. Investigators including Charles F. Code and colleagues at the Mayo Clinic (notably a 1956 study of the gastroesophageal sphincter in healthy people) and Franz Ingelfinger characterized a zone of high pressure at the lower end of the esophagus — the lower esophageal sphincter (LES) — a functional valve whose relaxation or weakness allows reflux. Establishing the LES as the key anti-reflux barrier reframed reflux disease as, in large part, a disorder of a sphincter that fails to do its job.
The second question — objective measurement — was transformed by prolonged (24-hour) esophageal pH monitoring, in which a thin pH-sensitive probe sits in the lower esophagus and records acid exposure across a full day and night of normal eating, activity, and sleep. The surgeon Tom R. DeMeester and colleagues are most closely associated with standardizing and quantifying this test; the composite “DeMeester score,” introduced in the mid-1970s, distilled the many pH measurements into a single number that distinguishes pathological reflux from the small amount of acid exposure seen in healthy people. For the first time, “you have reflux” could be backed by a reproducible measurement rather than by symptoms or endoscopic appearance alone.
Together, sphincter physiology and pH monitoring (later joined by manometry and, more recently, impedance-pH testing that can detect non-acidic reflux) gave clinicians the mechanistic and diagnostic backbone of modern reflux care. They also explained why some patients have classic symptoms with little visible esophagitis and others have damage with few symptoms — the burning sensation and the measurable acid load do not always march in step.
From Heartburn to “GERD”: Naming the Disease
The vocabulary of this condition evolved alongside the understanding of it, and the sequence is worth keeping straight because the names are often confused. The earliest modern label was Winkelstein’s peptic esophagitis (1935), emphasizing the digestive, acid-driven injury. Allison’s reflux esophagitis (late 1940s) emphasized the backward flow as the cause. Both terms, however, describe the visible inflammation of the esophagus — and physicians increasingly recognized that many patients suffer genuine, even severe, reflux symptoms while having little or no detectable esophagitis on endoscopy.
That recognition is what drove the shift to a broader name. The umbrella term “gastroesophageal reflux disease,” abbreviated GERD (or, in British usage, gastro-oesophageal reflux disease, GORD), gained traction in the later twentieth century to encompass the whole spectrum — symptoms, mucosal injury, and complications — rather than only the inflamed-esophagus subset. The terminology was progressively formalized through expert consensus statements; the influential Montreal definition of 2006, for example, defined GERD as a condition that develops when reflux of stomach contents causes troublesome symptoms and/or complications, explicitly making the patient’s symptom burden part of the definition. Historical reviews of the nomenclature emphasize that there was no single inventor of the word “GERD”; it emerged from clinical usage and was ratified by consensus, which is why this page describes its adoption as a gradual standardization rather than attributing it to one person or one year.
The upshot is a layered vocabulary that students of the disease should hold carefully: heartburn is the symptom; reflux is the event; esophagitis (peptic or reflux) is one possible consequence; Barrett’s esophagus and stricture are further complications; and GERD is the overarching disease concept that ties them together. Each term entered medicine at a different moment and for a different reason, and conflating them obscures the real history.
Treatment Milestones: Antacids to Proton Pump Inhibitors
The treatment of reflux advanced in three great waves, each defined by how thoroughly it could quiet stomach acid. The oldest and crudest wave was the antacid: alkaline substances that chemically neutralize acid already in the stomach. Bicarbonate, chalk, and later magnesium and aluminium salts (the familiar twentieth-century antacid mixtures) gave real but brief, partial relief — they mopped up acid for an hour or two without reducing how much the stomach made. For centuries this was essentially all that was available, and for mild, occasional heartburn it remains genuinely useful today.
The first true revolution came in 1976 with cimetidine (brand name Tagamet), the first H2-receptor antagonist — a drug that blocks histamine’s H2 receptors on the stomach’s acid-producing cells and so reduces acid secretion rather than merely neutralizing it. Cimetidine emerged from the deliberate, mechanism-based drug design program of Sir James Black and colleagues at Smith, Kline & French (work for which Black shared the 1988 Nobel Prize in Physiology or Medicine). For the first time, doctors could meaningfully turn down the acid tap; H2 blockers such as cimetidine, ranitidine, and famotidine became mainstays of ulcer and reflux therapy and, later, widely used over-the-counter remedies.
The second and larger revolution came in 1989, when omeprazole (brand name Prilosec/Losec) became the first proton pump inhibitor (PPI) approved in the United States, following its earlier introduction in Europe. Discovered through research at Sweden’s AB Hässle (part of Astra), PPIs act at the final common step of acid production — the gastric proton pump (H+/K+-ATPase) — and suppress acid far more completely and durably than H2 blockers. Severe reflux esophagitis that had resisted earlier drugs could now be healed reliably, and PPIs became some of the most widely prescribed medicines in the world. For selected patients, surgical anti-reflux procedures — the fundoplication, which wraps the upper stomach around the lower esophagus to reinforce the failing valve (associated especially with the surgeon Rudolph Nissen) — offer a mechanical alternative, with minimally invasive laparoscopic versions common from the 1990s.
Legacy and Honest Limits
Seen whole, the history of GERD is a model of how a timeless human symptom became a defined, measurable, and treatable disease within a single century. Heartburn was always there; what the twentieth century added was the chain of understanding — Tileston’s peptic ulceration of the esophagus, Winkelstein’s peptic esophagitis, Allison’s reflux esophagitis and the role of the hiatal hernia, Barrett’s columnar-lined esophagus and its later reinterpretation, the discovery of the lower esophageal sphincter, the quantification of reflux by 24-hour pH monitoring, and finally the H2-blocker and proton-pump-inhibitor drugs that gave clinicians genuine control over stomach acid.
It is worth being candid about the texture of this history. It did not proceed by a single heroic discovery but by accumulation, argument, and the occasional well-documented error — Barrett’s initial misreading of his own finding is the clearest example. Several of the terms (“GERD” itself, the boundaries of “reflux esophagitis”) were settled by consensus rather than coined by one person, and this page deliberately marks those as gradual standardizations rather than inventing a tidy attribution. That honesty is part of the point: real medical history is messier, and more interesting, than a list of lone geniuses.
Finally, a word for the reader living with reflux today. This page is history, not medical advice. Persistent heartburn, difficulty or pain on swallowing, unintended weight loss, vomiting, black or bloody stools, or chest pain that could be cardiac all warrant prompt evaluation by a clinician. Long-standing reflux deserves attention precisely because of the complications — stricture and Barrett’s esophagus — that this century of work taught us to watch for, and the treatments that history produced are genuinely effective when used wisely under medical guidance.
Research Papers and References
The references below combine peer-reviewed historical reviews of reflux disease and its nomenclature with curated PubMed topic-search links for readers who wish to explore the primary literature. Foundational historical papers — Winkelstein’s 1935 Peptic Esophagitis in JAMA, Barrett’s 1950 paper, Allison and Johnstone’s 1953 series, and Code and colleagues’ 1956 sphincter study — are named in the text as historical sources; the PubMed and DOI links below open in a new tab.
- Modlin IM, Kidd M, Lye KD. Historical perspectives on the treatment of gastroesophageal reflux disease. Gastrointestinal Endoscopy Clinics of North America. 2003;13(1):19-55. — PubMed: historical perspectives on GERD treatment
- Bremner CG. When did gastro-esophageal reflux become a disease? A historical perspective on GER(D) nomenclature. (historical review of reflux terminology) — PubMed: when did reflux become a disease (nomenclature)
- Winkelstein A. Peptic esophagitis: a new clinical entity. JAMA. 1935;104(11):906-909. (foundational description of acid-reflux esophageal injury) — PubMed: Winkelstein peptic esophagitis
- The elucidation of peptic esophagitis: from Hamperl to heartburn. Journal of Clinical Gastroenterology. 2007;41 Suppl 2:S95-S103. — PubMed 18027318: elucidation of peptic esophagitis
- Barrett NR. Chronic peptic ulcer of the oesophagus and ‘oesophagitis’. British Journal of Surgery. 1950;38(150):175-182. (original columnar-lined esophagus description) — PubMed: Barrett 1950 chronic peptic ulcer of the oesophagus
- Allison PR, Johnstone AS. The oesophagus lined with gastric mucous membrane. Thorax. 1953;8(2):87-101. — PubMed: Allison & Johnstone 1953 oesophagus lined with gastric mucosa
- Spechler SJ, Souza RF. History, molecular mechanisms, and endoscopic treatment of Barrett’s esophagus. Gastroenterology. 2010;138(3):854-869. — doi:10.1053/j.gastro.2010.01.002
- Code CF, Fyke FE Jr, Schlegel JF. The gastroesophageal sphincter in healthy human beings. Gastroenterologia. 1956;86(3):135-150. (definition of the lower esophageal sphincter) — PubMed: Code 1956 gastroesophageal sphincter
- Johnson LF, DeMeester TR. Twenty-four-hour pH monitoring of the distal esophagus: a quantitative measure of gastroesophageal reflux. American Journal of Gastroenterology. 1974;62(4):325-332. — PubMed: Johnson & DeMeester 24-hour pH monitoring
- Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. American Journal of Gastroenterology. 2006;101(8):1900-1920. — doi:10.1111/j.1572-0241.2006.00630.x
- Brimblecombe RW, Duncan WA, Durant GJ, et al. Cimetidine — a non-thiourea H2-receptor antagonist. Journal of International Medical Research. 1975;3(2):86-92. (development of the first H2 blocker) — PubMed: cimetidine H2-receptor antagonist development
- Lindberg P, Brandstrom A, Wallmark B, et al. Omeprazole: the first proton pump inhibitor. Medicinal Research Reviews. 1990;10(1):1-54. — PubMed 2404184: omeprazole, the first proton pump inhibitor
- Review article: from 1906 to 2006 — a century of major evolution of understanding of gastro-oesophageal reflux disease. Alimentary Pharmacology & Therapeutics. 2006;24(9):1267-1283. — doi:10.1111/j.1365-2036.2006.03122.x
- General PubMed topic search — history of gastroesophageal reflux disease and reflux esophagitis — PubMed: history of GERD and reflux esophagitis
External Authoritative Resources
- NIDDK (NIH) — Acid Reflux (GER & GERD) in Adults
- MedlinePlus — GERD
- PubMed — all research on the history of GERD
Connections
- Gastroenterology
- Gastroesophageal Reflux Disease (GERD) — Main Page
- Peptic Ulcer Disease
- Irritable Bowel Syndrome
- Inflammatory Bowel Disease
- Celiac Disease
- All Conditions