Metabolic Syndrome: History and Discovery
Metabolic syndrome is not a germ that was discovered or a single gene that was found — it is an idea that took shape slowly, as physicians across a century noticed that certain dangerous conditions kept turning up together in the same patients. The story moves in three stages: first the observation that high blood pressure, high blood sugar, and gout tend to cluster (Eskil Kylin, Sweden, 1923) and that upper-body obesity is the dangerous kind (Jean Vague, France, 1947); then the unifying hypothesis that insulin resistance is the common thread linking them, proposed by Gerald Reaven as "Syndrome X" in his 1988 Banting Lecture; and finally the naming and formal criteria — "the deadly quartet," "insulin resistance syndrome," and at last "metabolic syndrome," codified by WHO (1998–1999), the U.S. NCEP ATP III (2001), and the IDF (2005). Throughout, it is worth remembering that whether the syndrome is truly a single "entity" or simply a useful shorthand for shared risk remains genuinely debated.
Table of Contents
- What "Metabolic Syndrome" Means — and Why Its Origin Is Traceable
- The First Clustering: Eskil Kylin, 1923
- The Shape of the Risk: Jean Vague, 1947
- A Precursor Idea: Himsworth and Insulin Insensitivity
- The Unifying Hypothesis: Reaven's "Syndrome X," 1988
- Naming the Cluster: Deadly Quartet to Metabolic Syndrome
- Formal Criteria: WHO, ATP III, and the IDF
- Is It One Disease? The Ongoing Debate
- From Hypothesis to Everyday Clinic
- Research Papers and References
- Connections
- Featured Videos
What "Metabolic Syndrome" Means — and Why Its Origin Is Traceable
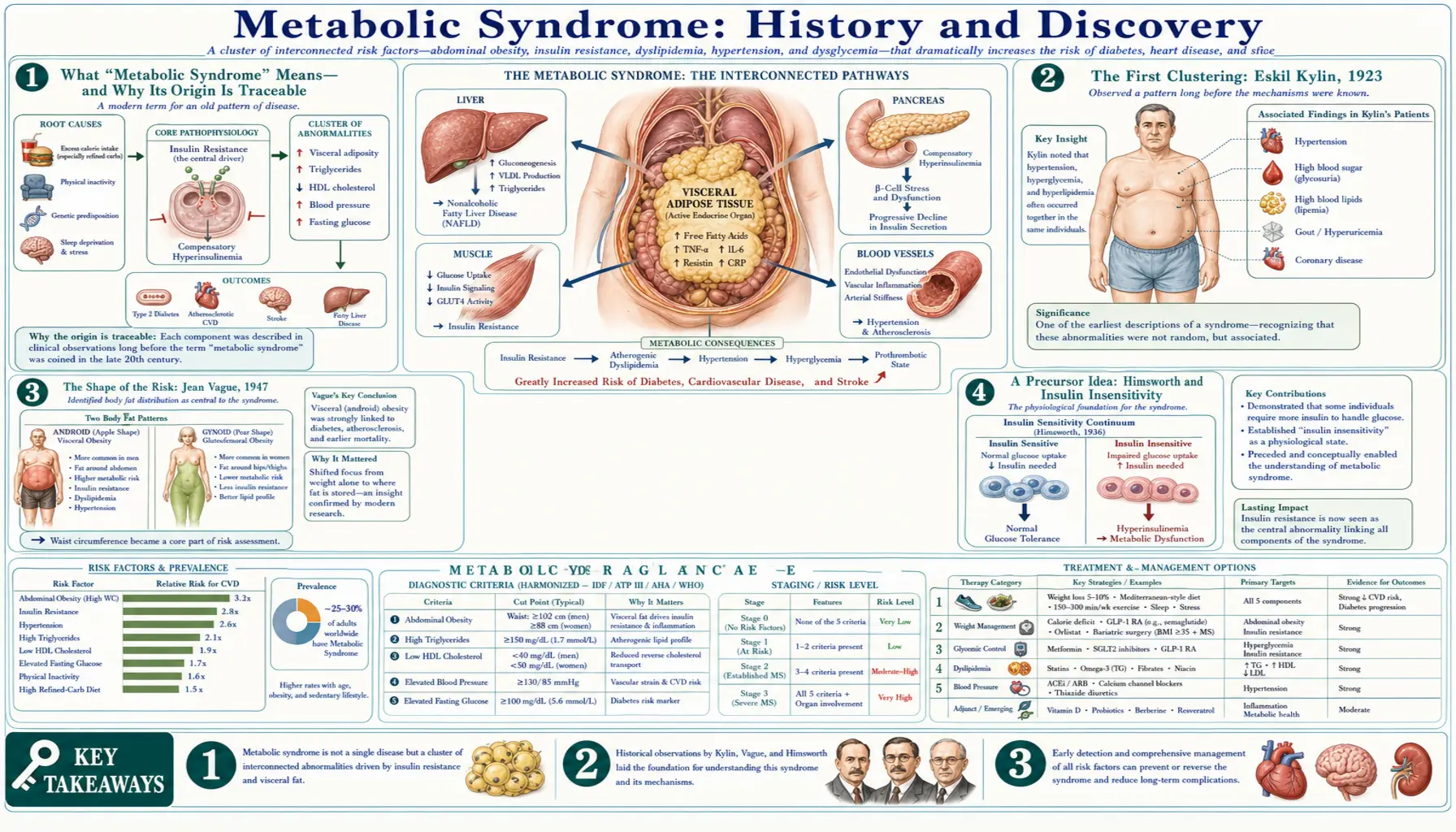
A syndrome, in medicine, is a recognizable pattern of signs and symptoms that occur together — not necessarily one disease with one cause, but a constellation reliable enough to be worth naming. Metabolic syndrome is exactly that: a cluster of cardiometabolic risk factors — abdominal (central) obesity, elevated blood pressure, elevated fasting blood sugar, high triglycerides, and low HDL ("good") cholesterol — that, when several appear in the same person, together raise the risk of type 2 diabetes and cardiovascular disease well beyond what any one factor would predict alone.
Because it is a concept rather than a microbe or a molecule, its history can be traced with unusual clarity: we can point to the papers in which the clustering was first described, the lecture in which a single underlying mechanism was first proposed, and the committee reports that fixed its name and its diagnostic thresholds. This page keeps three things carefully separate, because conflating them is the most common error in popular accounts: the early observation of the cluster (1920s–1940s); the hypothesis that insulin resistance unifies it (1988) — which is, and is here labelled as, a hypothesis; and the later naming and formal criteria (1989–2005).
One honest caution frames everything below. To say a syndrome was "discovered" risks implying more certainty than the science supports. The components were observed; the unifying mechanism was proposed and remains debated; the name and criteria were chosen by committees and have changed more than once. Where a date or a "first" is given here, it reflects the published record and is cross-checked against reputable medical sources — but the larger claim that all these features spring from one root cause is, to this day, an open scientific question rather than settled fact.
The First Clustering: Eskil Kylin, 1923
The earliest formal description usually credited as the seed of the metabolic-syndrome idea belongs to Eskil Kylin (1889–1975), a Swedish physician who began his research career studying arterial hypertension. In 1923 Kylin published an account of a clustering he had observed in his patients: hypertension (high blood pressure), hyperglycemia (high blood sugar), and hyperuricemia — the high uric acid that causes gout. He noticed that these three did not scatter randomly across a population but tended to congregate in the same individuals, suggesting some shared underlying disturbance rather than three unrelated diseases.
Kylin's observation is the headwater of the entire field. He did not have the tools to explain why the three traveled together — the hormone insulin had only just been isolated (1921–1922), and the modern understanding of insulin resistance lay decades ahead — but the simple, durable insight that these conditions cluster is the foundation on which every later formulation was built. His original work was published in German, the dominant language of medicine at the time; English-language reviews of metabolic syndrome routinely cite his 1923 paper as the first description of the cluster, and a Swedish appraisal of his career (catalogued in PubMed) documents his contributions in detail.
It is worth being precise about what Kylin did and did not do. He described an association — a co-occurrence — not a mechanism, and certainly not a named syndrome. Crediting him as the "first to describe metabolic syndrome" is a reasonable shorthand only if one understands it to mean "first to put the cluster of hypertension, hyperglycemia, and gout into the medical literature." That is the accurate, limited claim, and it is the one supported by the sources.
The Shape of the Risk: Jean Vague, 1947
The next decisive contribution came from Jean Vague (1911–2003), a physician in Marseilles, France. In 1947 Vague drew formal attention to something that turned out to be central: it is not merely how much fat a person carries that matters, but where they carry it. He distinguished two patterns of body-fat distribution — which he termed android (upper-body, abdominal, "apple-shaped," more typical of men) and gynoid (lower-body, hip-and-thigh, "pear-shaped," more typical of women) — and argued that it was the android, upper-body pattern that carried the heightened risk of diabetes, atherosclerosis, and gout.
This was a profound reframing. For the first time, obesity's danger was tied specifically to central fat, anticipating by half a century the modern emphasis on waist circumference as a core diagnostic measure of metabolic syndrome. Vague's insight reached the English-speaking world somewhat later; his work became widely available in English in the 1950s, and the English-language paper "Sexual differentiation, a determinant factor of the forms of obesity" is catalogued in PubMed and is frequently cited as the foundational statement of body-fat-distribution risk. Together, Kylin's cluster and Vague's "shape of the risk" supplied the two observational pillars on which the later unifying theory would rest.
As with Kylin, accuracy requires noting the limits. Vague identified a pattern and a risk gradient; he did not propose insulin resistance as the mechanism, and the word "syndrome" in its modern sense was not yet attached. His lasting contribution is the now-universal recognition that android, upper-body obesity is the metabolically dangerous kind — the conceptual ancestor of every waist-measurement threshold in today's criteria.
A Precursor Idea: Himsworth and Insulin Insensitivity
Before insulin resistance could be proposed as the link between the clustered risk factors, the very idea of insulin resistance had to exist. That idea has its own pioneer: the British physician Sir Harold Himsworth (1905–1993). Working in the 1930s, Himsworth performed experiments that led him to distinguish two kinds of diabetic patients — those who were "insulin sensitive" and those who were "insulin insensitive" (what we would now call insulin resistant). He proposed that diabetes could arise not only from a lack of insulin but from the body's inefficient response to it — a strikingly modern notion for its era.
Himsworth's work is the conceptual bridge between the early observers of the cluster and Reaven's later unifying hypothesis. He did not describe metabolic syndrome, and he should not be credited with it; his contribution was the narrower but essential one of establishing that tissues can resist insulin's action. Historians of the field — notably the review pointedly titled "Why Syndrome X? From Harold Himsworth to the Insulin Resistance Syndrome" — trace a direct intellectual line from Himsworth's 1930s insulin-insensitivity experiments to the insulin-resistance-centred theory that would define the syndrome fifty years later.
Including Himsworth here guards against a common oversimplification. The insight that the body can resist insulin was not original to Reaven; what Reaven did was take that older idea and propose it as the shared cause of a whole cluster of cardiovascular risks. Keeping the two contributions distinct — Himsworth's mechanism of insulin resistance, Reaven's use of it to unify the cluster — is the historically honest way to tell the story.
The Unifying Hypothesis: Reaven's "Syndrome X," 1988
The landmark moment — the point at which a loose collection of observations became a coherent theory — was the 1988 Banting Lecture delivered by the Stanford endocrinologist Gerald M. Reaven (1928–2018) to the American Diabetes Association. The Banting Lecture is the association's highest scientific honor, named for Frederick Banting, co-discoverer of insulin. In it, Reaven proposed what he called "Syndrome X": the hypothesis that insulin resistance (and the compensatory high insulin levels it provokes) is the central, shared abnormality that links together a cluster of conditions — impaired glucose tolerance, high blood pressure, elevated triglycerides, and low HDL cholesterol — and that this clustering is what drives cardiovascular disease risk.
This was the conceptual leap. Kylin and Vague had observed that the pieces traveled together; Reaven offered a mechanism for why — a single underlying defect from which the others could plausibly flow. The published lecture ("Role of insulin resistance in human disease," Diabetes, 1988; later reprinted in Nutrition, 1997) became one of the most cited papers in the field and is universally regarded as the founding document of the modern metabolic-syndrome concept. It must be stressed that this was framed, and is correctly understood, as a hypothesis: Reaven advanced insulin resistance as the unifying explanation, and a great deal of subsequent research has tested, supported, complicated, and contested it.
One detail is essential for accuracy and is frequently gotten wrong in popular summaries: Reaven's original 1988 Syndrome X did not include obesity as a defining component. He explicitly built the syndrome around insulin resistance, hyperinsulinemia, glucose intolerance, hypertension, raised triglycerides, and low HDL — and regarded obesity as a contributor to insulin resistance rather than as a core element of the syndrome itself. Central (abdominal) obesity was elevated to a defining criterion only later, by the committees that wrote the formal definitions, and made central by the IDF in 2005. Attributing the "obesity-centred" version to Reaven himself is a genuine historical error.
Naming the Cluster: Deadly Quartet to Metabolic Syndrome
Reaven's "Syndrome X" was a vivid name, but it had a problem: cardiologists were already using "Syndrome X" for an unrelated condition (angina with normal coronary arteries, sometimes called cardiac syndrome X). The years after 1988 therefore saw a small flurry of competing labels for Reaven's cluster, each emphasizing a different facet. In 1989, the American hypertension specialist Norman Kaplan proposed the memorable name "the deadly quartet" in a paper subtitled "upper-body obesity, glucose intolerance, hypertriglyceridemia, and hypertension" — notably folding upper-body (central) obesity back in as one of the four, in the spirit of Vague.
Other names competed for use as well. Because Reaven had placed insulin resistance at the center, the cluster was widely called the "insulin resistance syndrome" — a label many researchers preferred precisely because it named the proposed mechanism rather than a non-committal letter. Less formal terms such as "the metabolic syndrome" had appeared in the German and broader medical literature earlier in the twentieth century in various senses, but it was in this post-1988 period that "metabolic syndrome" gradually won out as the standard English term — broad enough to accommodate the evolving list of components without committing to a single disputed cause.
The lesson of this naming history is that the choice of label was never neutral. "Syndrome X" sidestepped mechanism; "insulin resistance syndrome" asserted it; "the deadly quartet" emphasized danger and re-centred obesity; "metabolic syndrome" was the deliberately ecumenical compromise that survived. None of these names settled the underlying scientific question of whether the cluster is one entity — they simply gave clinicians a shared vocabulary while that question stayed open.
Formal Criteria: WHO, ATP III, and the IDF
A named idea becomes a usable clinical diagnosis only when someone specifies exactly which measurements, at which thresholds, in what combination, count. That work fell to expert committees, and it produced several definitions that do not perfectly agree — a fact that itself reveals how much remained unsettled. The first formal definition came from the World Health Organization (WHO): a working definition appeared in a 1998 consultation document and was finalized in 1999. The WHO definition was insulin-resistance-centred — in keeping with Reaven's theory, it required evidence of insulin resistance (impaired glucose tolerance, impaired fasting glucose, type 2 diabetes, or directly measured impaired glucose uptake) plus additional factors such as obesity, hypertension, dyslipidemia, or microalbuminuria. Its reliance on measurements like insulin sensitivity and urinary microalbumin made it accurate but cumbersome for everyday clinical use.
The definition that made metabolic syndrome a household clinical term arrived in 2001 from the U.S. National Cholesterol Education Program, Adult Treatment Panel III (NCEP ATP III). Its great virtue was simplicity: it used five ordinary measurements — waist circumference, triglycerides, HDL cholesterol, blood pressure, and fasting glucose — and required that any three of the five meet defined thresholds. No special insulin testing was needed, so any clinician with a tape measure, a blood-pressure cuff, and a basic blood panel could apply it. This pragmatic, count-three-of-five design is why the ATP III definition spread so widely and still shapes how most clinicians think about the syndrome.
In 2005 the International Diabetes Federation (IDF) issued a definition that made one consequential change: it placed central (abdominal) obesity at the center, requiring elevated waist circumference as a mandatory criterion (plus any two of the remaining factors), and — importantly — specified ethnicity-specific waist thresholds, recognizing that the same waist measurement carries different risk across populations. That same year, the AHA and NHLBI updated the ATP III criteria; subsequent efforts (a 2009 "harmonized" joint statement) tried to reconcile the competing definitions. The very existence of WHO, ATP III, and IDF criteria that disagree on what is mandatory and where the cut-points lie is the clearest evidence that metabolic syndrome is a convention agreed by committees, not a natural kind with a single objective boundary.
Is It One Disease? The Ongoing Debate
For all its clinical usefulness, the status of metabolic syndrome as a single "entity" has been seriously and repeatedly questioned — and intellectual honesty demands that this be stated plainly rather than buried. The sharpest critique came in 2005, when the American Diabetes Association and the European Association for the Study of Diabetes jointly published a critical appraisal arguing that the syndrome had been imprecisely defined, that its components were inconsistent across definitions, and crucially that the whole did not clearly predict cardiovascular risk better than the sum of its individual parts. Their pointed conclusion was that clinicians should treat each risk factor on its merits and be cautious about labelling patients with a "syndrome" that might not behave as a unified disease.
The core of the debate is whether metabolic syndrome reflects one shared cause — Reaven's insulin resistance, or perhaps central obesity, or some upstream factor — or whether it is simply a statistical co-occurrence of related risk factors that happen to share lifestyle and genetic drivers. Reaven himself, late in his career, expressed reservations about how his idea had been turned into rigid diagnostic checklists, worrying that the formal criteria had drifted from the insulin-resistance mechanism he considered central. A WHO Expert Consultation later revisited the question of whether the concept was a "useful concept or clinical tool," reflecting continued institutional ambivalence.
None of this means the term is worthless. Identifying someone with several clustered cardiometabolic abnormalities is a practical, communicable way to flag elevated risk and prompt action on diet, weight, blood pressure, lipids, and blood sugar together. But a history page must not overstate certainty: metabolic syndrome is a useful clinical construct whose unity remains scientifically contested. That is the accurate, current state of the question — not a closed case, but a working framework whose limitations are openly acknowledged in the literature.
From Hypothesis to Everyday Clinic
Whatever its disputed metaphysics, the metabolic-syndrome concept has had an enormous and largely positive practical effect. It took a set of risk factors that had traditionally been managed in separate silos — the cardiologist watching blood pressure, the lipid specialist watching cholesterol, the diabetologist watching glucose — and reframed them as a connected pattern demanding integrated attention. That reframing helped move prevention upstream, encouraging clinicians to act on a clustering of borderline abnormalities before any one of them crossed the threshold into overt diabetes or a heart attack.
The historical arc also reshaped public-health messaging. Vague's 1947 insight about upper-body fat became the everyday advice to mind one's waistline, not just the bathroom scale. Reaven's insulin-resistance hypothesis drove decades of research into how diet, physical activity, and weight loss improve insulin sensitivity, and underpins the modern emphasis on lifestyle change as first-line therapy. The committee criteria, for all their disagreements, gave epidemiologists a common yardstick to measure how widespread the problem had become — and the answer, across many countries, was "alarmingly so."
The thread running from Kylin's 1923 cluster, through Vague's body-shape risk and Himsworth's insulin insensitivity, to Reaven's unifying lecture and the WHO/ATP III/IDF criteria, is a clean example of how medicine builds a concept: observation first, hypothesis next, naming and operational definition last — and honest, continuing debate throughout. For the everyday reader, the takeaway is simple and empowering. The conditions that make up metabolic syndrome tend to travel together, they share common roots in how the body handles fat and sugar, and — most encouragingly — they respond to many of the same changes in diet, movement, and weight. The detailed mechanisms, diagnosis, and management are covered on the main Metabolic Syndrome page and on the closely related Insulin Resistance page.
Research Papers and References
The references below combine the landmark primary papers in the history of metabolic syndrome with peer-reviewed historical reviews and curated PubMed topic-search links. Where a stable DOI or PMID is available and verified it is given; otherwise a PubMed topic search opens the relevant literature. Each external link opens in a new tab at the National Library of Medicine or the publisher.
- Reaven GM. Banting Lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595-1607. — doi:10.2337/diab.37.12.1595
- Reaven GM. Banting Lecture 1988. Role of insulin resistance in human disease (reprint). Nutrition. 1997;13(1):65 (discussion 64,66). — PubMed PMID: 9058458
- Kaplan NM. The deadly quartet: upper-body obesity, glucose intolerance, hypertriglyceridemia, and hypertension. Archives of Internal Medicine. 1989;149(7):1514-1520. — PubMed PMID: 2662932
- Vague J. Sexual differentiation, a determinant factor of the forms of obesity (1947; English reprint). Obesity Research. 1996;4(2):201-203. — PubMed PMID: 8681056
- Nilsson SE. [Research contributions of Eskil Kylin] (in Swedish). — PubMed PMID: 11813720
- Reaven GM. Why Syndrome X? From Harold Himsworth to the insulin resistance syndrome. Cell Metabolism. 2004;1(1):9-14. — doi:10.1016/j.cmet.2004.01.001
- Krentz AJ. Sir Harold Himsworth and insulin insensitivity 75 years on. Diabetic Medicine. 2011. — doi:10.1111/j.1464-5491.2011.03488.x
- Alberti KGMM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1 (WHO consultation, the original WHO metabolic-syndrome working definition). Diabetic Medicine. 1998;15(7):539-553. — PubMed: WHO 1998/1999 definition
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report (NCEP ATP III). JAMA. 2001;285(19):2486-2497. — doi:10.1001/jama.285.19.2486
- Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome — a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabetic Medicine. 2006;23(5):469-480. — doi:10.1111/j.1464-5491.2006.01858.x
- Kahn R, Buse J, Ferrannini E, Stern M. The metabolic syndrome: time for a critical appraisal. Joint statement from the ADA and the EASD. Diabetes Care. 2005;28(9):2289-2304. — doi:10.2337/diacare.28.9.2289
- Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. The Lancet. 2005;365(9468):1415-1428. — doi:10.1016/S0140-6736(05)66378-7
- History and evolving definitions of the metabolic syndrome (topic search). — PubMed: metabolic syndrome history and definitions
- From Syndrome X to cardiometabolic risk — clinical and public-health implications (topic search). — PubMed: Syndrome X to cardiometabolic risk
External Authoritative Resources
- NHLBI (NIH) — Metabolic Syndrome
- MedlinePlus — Metabolic Syndrome
- PubMed — All research on the history of metabolic syndrome
Connections
- Metabolic Syndrome (main page)
- Insulin Resistance
- Diabetes
- Obesity
- Hypertension
- Reversing Insulin Resistance — how the mechanism Reaven proposed in 1988 is measured and reversed today.
- All Conditions