Folliculitis
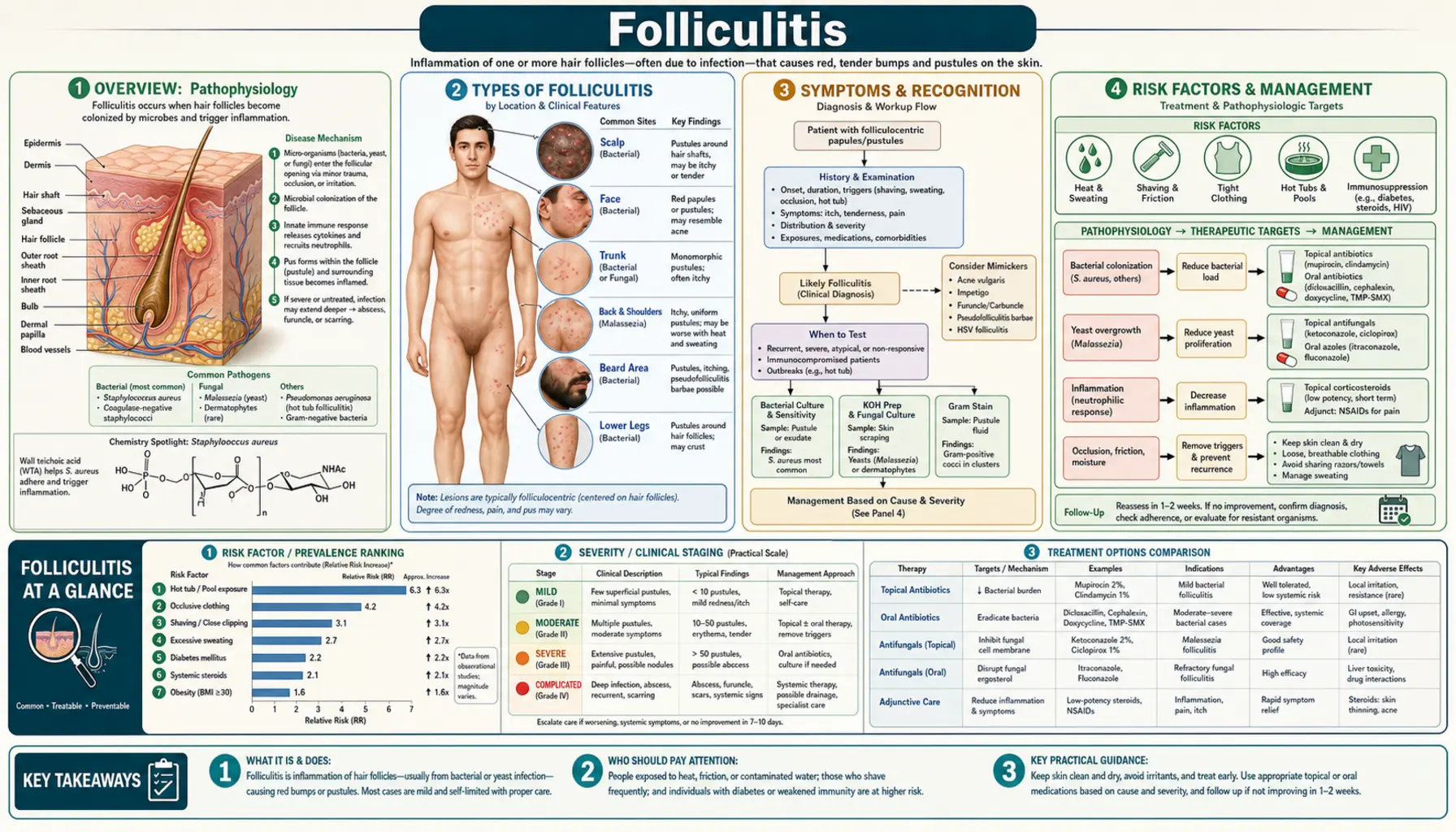
Table of Contents
- Overview
- Types of Folliculitis
- Symptoms and Recognition
- Risk Factors
- Diagnosis
- Treatment: Bacterial Folliculitis
- Treatment: Non-Bacterial Forms
- Prevention
- Natural and Integrative Approaches
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
Overview
Folliculitis is inflammation of one or more hair follicles — the tiny pockets in the skin from which each hair grows. It is one of the most common skin conditions worldwide, estimated to affect more than one billion people at some point in their lives. Folliculitis can occur anywhere hair grows on the body: the scalp, face, neck, chest, back, buttocks, and legs are all frequent sites.
Most cases are caused by bacteria, with Staphylococcus aureus being the most common culprit. However, folliculitis can also be triggered by fungi (most often Malassezia yeast), viruses, parasites, or non-infectious causes such as ingrown hairs and hot-tub exposure. The condition ranges from a mild, self-resolving nuisance — small red bumps that clear up on their own — to deeper, painful infections such as boils and carbuncles that require medical treatment.
Because folliculitis looks similar to several other skin conditions, it is frequently misdiagnosed. Malassezia folliculitis (a fungal form) is routinely mistaken for acne, and treating it with antibiotics actually makes it worse. Knowing which type of folliculitis you have makes all the difference in choosing the right treatment.
Types of Folliculitis
Bacterial Folliculitis
The vast majority of folliculitis cases are bacterial, and Staphylococcus aureus is the organism responsible for most of them.
Superficial folliculitis (Bockhart's impetigo) is the most common form. A small pustule forms right at the follicle opening with the hair shaft visible at its center. The surrounding skin is slightly red but the infection stays shallow and usually clears within 1–2 weeks with basic care.
Deep folliculitis involves the entire hair follicle. When a single follicle becomes deeply infected it forms a furuncle (boil) — a painful, swollen nodule 1–5 cm across with a tender fluctuant center and a central yellowish plug. When several adjacent follicles fuse into one large interconnected infection the result is a carbuncle, which has multiple drainage points, causes significant pain, and often produces fever and general malaise requiring prompt medical attention.
Gram-negative folliculitis is a less obvious form that paradoxically develops after prolonged antibiotic therapy for acne. Long-term antibiotics wipe out the normal skin flora that kept gram-negative bacteria (such as E. coli, Klebsiella, Enterobacter, and Proteus) in check. The result is a pustular flare concentrated around the nose and chin that looks like worsening acne but does not respond to standard acne antibiotics.
Sycosis barbae is a chronic, deep staphylococcal folliculitis confined to the beard area in men. It presents as recurring, tender papules and pustules in the mustache and beard area and can be difficult to eradicate without addressing MRSA carrier status.
Pseudomonas (Hot Tub) Folliculitis
Pseudomonas aeruginosa thrives in warm, improperly chlorinated water — hot tubs, whirlpool baths, water parks, and swimming pools. Exposure to contaminated water allows the bacteria to enter follicles. Symptoms appear 1–2 days after exposure: itchy red bumps and pustules concentrated on the trunk and buttocks (the areas covered by a bathing suit). A concurrent ear infection (swimmer's ear) may develop at the same time.
In healthy people, hot tub folliculitis is self-limiting and resolves without treatment in 1–2 weeks. The key clue is the cluster exposure — if multiple people who shared the same hot tub all break out simultaneously, Pseudomonas is almost certainly the cause.
Fungal (Malassezia) Folliculitis
Malassezia furfur (also called Pityrosporum) is a yeast that normally lives on human skin. Under the right conditions — heat, sweating, occlusive clothing, oily skin, or antibiotic use — it overgrows inside follicles and triggers inflammation.
Malassezia folliculitis presents as uniformly sized itchy pustules on the upper back, chest, and shoulders. This monomorphic appearance — all bumps look exactly alike — is an important distinguishing feature from ordinary acne, which has mixed lesions (blackheads, whiteheads, and inflamed spots of varying sizes). Antibiotics worsen Malassezia folliculitis by killing the bacteria that compete with the yeast, so getting the diagnosis right before starting treatment is critical. If the bumps respond quickly to an antifungal wash, that response itself confirms the diagnosis.
Pseudofolliculitis Barbae (Razor Bumps)
Pseudofolliculitis barbae is not an infection at all — it is a mechanical, inflammatory reaction. After shaving, naturally curly or coily hair shafts re-enter the skin near the follicle opening rather than growing outward. The immune system treats the embedded hair as a foreign body and mounts an inflammatory response, producing painful red bumps and, over time, post-inflammatory hyperpigmentation and scarring.
This condition affects an estimated 45–85% of Black men and up to 30% of Black women who shave, though it can affect anyone with curly hair. The chin, neck, and bikini line are the most commonly affected sites.
Viral Folliculitis
Herpes simplex virus can infect hair follicles, producing clusters of vesicles (blisters) around the mouth or genital area that are sometimes mistaken for bacterial folliculitis. Demodex mites (microscopic skin mites), which play a central role in rosacea, can also cause a folliculitis-like eruption, particularly in immunocompromised individuals.
Symptoms and Recognition
The hallmark of folliculitis in any form is that the bumps are centered on hair follicles. Look for a hair shaft emerging from the center of a bump — this is the single most reliable sign that you are dealing with folliculitis rather than another skin condition.
Superficial folliculitis produces small red papules (bumps) or white-headed pustules at the follicle opening. They are mildly tender or itchy, surrounded by a thin ring of redness, and usually no larger than a few millimeters. Most people notice them on the legs after shaving, on the scalp, or on the back.
Deep folliculitis is more dramatic. A furuncle starts as a firm, tender nodule that grows over 4–7 days into a fluctuant (fluid-filled) swelling. A yellow or white central point eventually forms as pus accumulates. Carbuncles are larger, deeper, and accompanied by systemic signs: fever, chills, and fatigue.
Where on the body the bumps appear is an important clue to the cause:
- Scalp: staphylococcal folliculitis in adults; tinea capitis (ringworm) in children; dissecting cellulitis of the scalp in severe cases
- Face and beard area: sycosis barbae, pseudofolliculitis barbae, viral folliculitis
- Upper back and chest: Malassezia folliculitis (most likely), staphylococcal folliculitis
- Trunk and buttocks: hot tub folliculitis (especially after a cluster exposure)
- Thighs and buttocks: staphylococcal folliculitis from friction and occlusion
- Lower legs: post-shaving folliculitis; gram-negative folliculitis after waxing
Eosinophilic folliculitis is a distinct form seen in people with HIV/AIDS or other immunocompromising conditions, and in newborns. It produces intensely itchy, recurrent eruptions with a high eosinophil count in the blood. A skin biopsy showing eosinophilic infiltrates around the follicle confirms the diagnosis.
Risk Factors
Factors That Raise Bacterial Risk
- Breaks in the skin barrier — cuts, abrasions, insect bites, or eczema allow bacteria to enter follicles
- Friction and occlusion — tight clothing, thigh rubbing, and equipment straps trap heat and moisture
- Shaving, waxing, and plucking — all disrupt the follicle opening temporarily
- Acne — inflamed follicles are already compromised
- Immunosuppression — diabetes, HIV, corticosteroid use, and chemotherapy all impair the skin's ability to fight bacterial invasion
- MRSA carrier status — nasal MRSA carriage is a major source of recurrent skin infections
- Contact sports — wrestling in particular carries a high risk of skin-to-skin bacterial transmission ("wrestler's impetigo")
Factors That Raise Fungal Risk
- Antibiotic use — oral antibiotics reduce bacterial competition and allow yeast to proliferate
- Hot, humid climates and heavy sweating
- Occlusive synthetic fabrics — trap heat and moisture against the skin
- Oily skin — Malassezia feeds on fatty acids in sebum
Factors That Raise Hot Tub Risk
- Using hot tubs, whirlpools, or pools with inadequate chlorination or pH control
- Extended time in the water — longer exposure means more bacterial entry
Factors That Raise Pseudofolliculitis Risk
- Naturally curly or coily hair — the strongest single risk factor
- Shaving very closely or against the grain
- Multi-blade razors — each additional blade cuts the hair below the skin surface, making re-entry more likely
- Tight collars and waistbands — the friction drives hair ends back into the skin
Occupational Risks
- Oil and grease workers — mineral oil blocks follicles mechanically (oil folliculitis)
- Healthcare workers — higher MRSA exposure
Diagnosis
Most folliculitis is diagnosed clinically — a combination of the appearance of the lesions, where they are located, and the patient's history is usually enough to reach the right diagnosis. No testing is needed for a straightforward, first-time, mild case.
Additional testing becomes important when:
- Folliculitis is recurrent or treatment is not working
- MRSA is suspected (recent hospitalization, household contacts with skin infections, known MRSA history)
- The diagnosis is uncertain
- Systemic symptoms (fever, swollen lymph nodes) are present
Tests Used
- Bacterial culture: Swab the contents of a pustule. Tells you exactly which bacteria are present and which antibiotics will work. Essential for suspected MRSA and for treatment failures.
- KOH preparation: A quick microscopy test where the pustule contents are dissolved in potassium hydroxide. In Malassezia folliculitis, yeast buds and short hyphae (the "spaghetti and meatballs" pattern) are visible under the microscope. Highly specific when positive.
- Fungal culture: More sensitive than KOH but takes days to weeks to grow. Used when KOH is negative but fungal infection is still suspected.
- Wood's lamp examination: A UV light that makes Malassezia fluoresce pale yellow-green. Useful in a clinic setting for quick screening.
- Skin biopsy: Punch biopsy with histopathology is the most definitive test. Used when the diagnosis remains uncertain after simpler tests, or when eosinophilic folliculitis, demodex infestation, or a non-infectious cause is suspected.
- Blood tests: A complete blood count (CBC) is helpful for deep infections with systemic symptoms. HIV serology should be offered to anyone with eosinophilic folliculitis or recurrent severe infections without an obvious cause.
Conditions That Can Look Like Folliculitis
- Acne vulgaris: Acne has comedones (blackheads and whiteheads), which folliculitis does not. Acne is also more concentrated on the face and back.
- Keratosis pilaris: Rough, "chicken skin" bumps on the upper arms and thighs. No pustules, no infection — just keratin plugging the follicle opening.
- Eczema: Intense itch, scale, and weeping without a follicular pattern.
- Miliaria (heat rash): Tiny vesicles caused by blocked sweat ducts, not follicles. Appears in heat, no central hair.
- Contact dermatitis: Rash confined to the area of contact with an irritant or allergen; no follicular clustering.
Treatment: Bacterial Folliculitis
Mild, Localized Cases
Most superficial bacterial folliculitis clears up with basic measures:
- Warm compresses applied 3–4 times daily for 15–20 minutes soothe discomfort and promote natural drainage of pustules.
- Topical mupirocin 2% ointment (Bactroban) applied three times daily for 7–10 days is effective for localized staphylococcal folliculitis and for MRSA on the skin surface.
- Topical clindamycin 1% lotion or gel twice daily is an alternative first-line topical antibiotic.
- Benzoyl peroxide wash (5–10%) used daily reduces S. aureus colonization of the skin surface and helps prevent recurrence. It does not cause antibiotic resistance.
- Gentle exfoliation with a soft washcloth removes dead skin cells that can block follicle openings.
- Non-occlusive, fragrance-free skincare products avoid further blocking follicles.
Moderate Cases (Spreading, Deeper, or Recurrent)
When folliculitis is widespread, involves deeper tissue, or keeps coming back, oral antibiotics are needed:
- Cephalexin 500 mg four times daily for 7–10 days is the standard first-line oral antibiotic for staphylococcal folliculitis when MRSA is not suspected.
- Dicloxacillin 500 mg four times daily is an alternative with excellent staphylococcal coverage.
MRSA-Suspected Folliculitis
Methicillin-resistant Staphylococcus aureus (MRSA) does not respond to cephalexin or dicloxacillin. If you have been to a hospital recently, have household contacts with skin infections, or your infection is not responding to standard antibiotics, MRSA should be considered:
- Trimethoprim-sulfamethoxazole (TMP-SMX, Bactrim) 1–2 double-strength tablets twice daily for 7–10 days — highly effective against community-acquired MRSA
- Doxycycline 100 mg twice daily for 7–10 days
- Clindamycin 300 mg three times daily (local resistance rates vary — a culture-based sensitivity test helps guide this choice)
Managing a Furuncle (Boil)
Warm compresses speed up the process of a boil coming to a head (pointing). Once the boil is soft and fluctuant, incision and drainage (I&D) by a clinician is the definitive treatment — it relieves pain immediately and promotes healing far faster than antibiotics alone.
After I&D in an otherwise healthy person, antibiotics are usually not needed. Antibiotics are added when the person is immunocompromised, has diabetes, has a fever, shows signs of surrounding skin infection (cellulitis), or the boil is in a high-risk location (face, genitalia).
MRSA Decolonization for Recurrent Staph Infections
If you keep getting staph folliculitis or boils, you may be carrying MRSA in your nose or on your skin without knowing it. Decolonization breaks the cycle:
- Nasal mupirocin 2% ointment applied inside both nostrils twice daily for 5 days eliminates nasal MRSA carriage, the most common reservoir for recurrent skin infections.
- Chlorhexidine 4% body wash used daily for 5–14 days reduces skin surface MRSA colonization.
- Household contacts should be treated at the same time — re-colonization from a family member is a frequent reason decolonization fails.
- Wash and dry all bedding, towels, and clothing that contact affected skin. MRSA can survive on fabric for days.
Treatment: Non-Bacterial Forms
Malassezia (Fungal) Folliculitis
The key insight here is that antifungal treatment — not antibiotics — is required. Antibiotics actively worsen this condition.
- Topical ketoconazole 2% shampoo applied to the chest and back daily for 4 weeks, left on for 5 minutes before rinsing, is the standard first-line treatment. A rapid response (itching improves within 1–2 weeks) is itself diagnostic.
- Selenium sulfide 2.5% shampoo used similarly is a cost-effective alternative.
- Topical ciclopirox gel or cream applied twice daily works against Malassezia and is available by prescription.
- Oral itraconazole 200 mg daily for 5–7 days is reserved for more severe or treatment-resistant cases.
- Maintenance therapy with weekly ketoconazole wash prevents recurrence in susceptible individuals, especially in hot weather or after antibiotic courses.
Pseudomonas (Hot Tub) Folliculitis
In healthy people this almost always clears up on its own within 1–2 weeks without any treatment. Reassurance and avoiding further hot tub exposure are the main recommendations.
Antibiotics (ciprofloxacin 500 mg twice daily for 7–10 days) are used only when symptoms persist beyond two weeks or the person is immunocompromised.
Prevention is the real solution: maintain hot tub free chlorine at 1–3 ppm and pH at 7.2–7.8. Test the water before entering any shared hot tub. Shock with a higher-dose chlorine treatment weekly.
Pseudofolliculitis Barbae (Razor Bumps)
This condition is mechanical, not infectious, so antibiotics and antifungals have no role. The goal is to stop the hair from re-entering the skin:
- Stop shaving temporarily for 2–4 weeks to allow existing ingrown hairs to grow out and inflammation to subside. Even a few days of stubble makes a difference.
- Single-blade razors — multi-blade razors pull the hair beyond the skin surface before cutting, depositing the cut end below skin level where it can re-enter. A single blade cuts at skin level only.
- Shave with the grain, not against it. Shaving against the grain creates a sharper, angled cut end that penetrates skin more easily.
- Chemical depilatories (products containing calcium thioglycolate or benzoyl benzoate) dissolve hair at skin level rather than cutting it, eliminating the sharp-edged stub that causes re-entry. Patch test first — these products can irritate sensitive skin.
- Topical tretinoin 0.025–0.05% cream applied nightly speeds up skin cell turnover and helps prevent the skin from growing over re-entering hairs.
- Topical eflornithine (Vaniqa) cream slows hair regrowth, reducing shaving frequency and the risk of re-entry.
- Glycolic acid exfoliants (5–8%) gently loosen the skin surface, freeing trapped hairs before they cause inflammation.
- Laser hair removal is the most effective long-term solution. The Nd:YAG 1064nm laser is safe for all skin types including dark skin tones (where pulsed dye lasers and some IPL devices are not). Multiple sessions (typically 6–8) are needed for permanent results, and the upfront cost pays off against a lifetime of razor and treatment costs.
Eosinophilic Folliculitis
This rare form requires a specialist approach:
- Permethrin 5% cream when Demodex mites are suspected as a contributing factor
- Antihistamines for symptomatic itch relief
- Narrowband UVB phototherapy reduces the eosinophilic inflammation
- Isotretinoin in severe, refractory cases
- Antiretroviral therapy for HIV-positive patients — treating the underlying immune dysfunction is the most important step
Prevention
Daily Skin Hygiene
- Wash daily with a gentle, non-comedogenic cleanser — avoid harsh soaps that strip the skin's natural protective oils.
- Shower promptly after exercise, swimming, or any activity that causes heavy sweating. S. aureus counts on the skin surface rise significantly within 30 minutes of starting exercise.
- Use non-occlusive, fragrance-free moisturizers. Heavy creams and oils can block follicles.
Clothing and Physical Activity
- Wear breathable, moisture-wicking fabrics (100% cotton is ideal for underwear and base layers).
- Avoid tight synthetic fabrics in warm weather — they trap heat and moisture against the skin.
- Disinfect shared exercise equipment before and after use. Gym equipment harbors S. aureus and MRSA.
- Launder workout clothes after every use. Re-wearing sweaty clothing re-inoculates the skin with bacteria.
Shaving Best Practices
- Soften hair with warm water for at least 2–3 minutes before shaving.
- Use a sharp blade — dull blades drag and tear rather than cut cleanly.
- Shave with the grain of hair growth.
- People with curly or coily hair should consider single-blade razors, electric shavers (which do not cut as close), or hair removal alternatives.
- Replace blades regularly — a single-use disposable should not be used more than 3–5 times.
Hot Tub and Pool Safety
- If you own a hot tub, test the water chemistry at least twice a week. Maintain free chlorine at 1–3 ppm and pH at 7.2–7.8. Shock with higher chlorine weekly.
- At shared facilities (gyms, water parks, spas), dip a chlorine test strip before entering. If strips are not available, a faint chlorine smell is a reasonable sign that the water is treated — no smell at all from water that has many users is a warning sign.
- Shower immediately after leaving any shared water facility.
Preventing MRSA Spread
- Never share razors, towels, washcloths, or clothing with others, even family members.
- Cover all open wounds, cuts, and abrasions with clean bandages.
- Treat skin infections promptly — do not wait and see if a boil resolves on its own.
- If someone in your household has recurrent staph infections, discuss nasal decolonization with a healthcare provider for all household members.
Diet and Immune Support
- Zinc is essential for skin barrier function, wound healing, and immune defense against bacterial invasion. Adequate dietary zinc (from meat, shellfish, legumes, seeds) or supplementation supports resistance to folliculitis.
- Vitamin C supports collagen synthesis and immune function, both critical for skin integrity.
- Adequate protein provides the amino acids needed for skin repair and antibody production.
- High-glycemic diets (refined sugar, white bread, soft drinks) raise levels of insulin-like growth factor 1 (IGF-1), which increases sebum production and promotes follicular inflammation. Reducing sugar and refined carbohydrates benefits both acne and folliculitis.
- Well-controlled blood sugar in people with diabetes significantly reduces the risk of skin infections — poorly controlled diabetes impairs neutrophil function and slows wound healing.
Natural and Integrative Approaches
Mild folliculitis often self-resolves. Moderate or severe cases need medical treatment. The approaches below are evidence-informed adjuncts, not replacements for prescription antibiotics or antifungals when those are indicated.
Tea Tree Oil
Melaleuca alternifolia oil has well-documented antibacterial activity against S. aureus, including some MRSA strains. A concentration of 5% topical tea tree oil gel has been studied in randomized controlled trials and shown comparable efficacy to benzoyl peroxide for inflammatory lesions. Apply diluted tea tree oil (5% in a carrier oil or gel) 2–3 times daily. Never apply undiluted tea tree oil directly to skin — it causes chemical burns at full strength. Keep away from eyes.
Manuka Honey
Manuka honey from New Zealand contains high concentrations of methylglyoxal (MGO), which gives it potent antibacterial activity including against MRSA. Applied topically to folliculitis lesions or as an occlusive wound dressing on boils, manuka honey creates a moist healing environment while actively inhibiting bacterial growth. Look for honey with a high MGO or UMF (Unique Manuka Factor) rating — higher numbers mean more antibacterial activity.
Colloidal Oatmeal
Finely ground oatmeal has FDA-approved status as a skin protectant. Its avenanthramides inhibit NF-kB-mediated inflammation, reducing redness and itch. Add 1 cup to a lukewarm bath and soak for 15–20 minutes, or apply a colloidal oatmeal cream directly to itchy folliculitis lesions. Particularly helpful for widespread, itchy cases like hot tub folliculitis.
Apple Cider Vinegar (Diluted)
Undiluted acetic acid from apple cider vinegar has in vitro antibacterial activity and lowers skin surface pH (which inhibits bacterial colonization). Practical application: dilute 1 part ACV with 1 part water and apply with a cotton ball to affected areas. Do not use on broken, open, or severely inflamed skin — the acidity will sting and delay healing. The evidence base is limited to in vitro studies; use as an adjunct only.
Neem Oil
Azadirachta indica (neem) has demonstrated antibacterial and antifungal properties in laboratory studies, including activity against S. aureus and Malassezia species. Traditional Ayurvedic medicine has used neem preparations for skin infections for centuries. Apply diluted neem oil (a few drops in a carrier oil) to affected areas. Clinical trial evidence in humans remains limited, but the safety profile is good for topical use.
Aloe Vera
Fresh aloe vera gel contains compounds including acemannan and aloin that inhibit prostaglandin production and reduce inflammation. Applied topically, it soothes redness, reduces itch, and maintains skin hydration — all useful adjuncts to active folliculitis treatment. Use pure gel (without added alcohol or artificial fragrance) and apply 2–3 times daily.
Turmeric (Internal and Topical)
Curcumin, the active compound in turmeric, inhibits S. aureus biofilm formation in vitro — biofilm is the protective matrix that makes folliculitis harder to treat and more prone to recurrence. Curcumin also inhibits NF-kB, reducing production of inflammatory cytokines. Oral curcumin (500–1000 mg daily, with black pepper extract for absorption) complements topical treatment. A paste of turmeric powder mixed with a small amount of coconut oil applied to individual pustules is a traditional remedy with plausible biological rationale.
Probiotics
Emerging evidence suggests that the skin microbiome — the community of beneficial bacteria living on skin — protects against S. aureus colonization. Oral probiotics, particularly Lactobacillus strains, may help restore this balance. Probiotics also support gut barrier integrity, which is relevant to the systemic inflammatory component of recurrent skin infections. Evidence is early but the safety profile of standard probiotic supplements is excellent.
Zinc
Zinc deficiency impairs neutrophil function, keratinocyte differentiation, and the skin's ability to mount an antibacterial defense. Topical zinc pyrithione (the active ingredient in many dandruff shampoos) also has direct activity against Malassezia species, making it a dual-purpose adjunct for Malassezia folliculitis when used as a body wash. Oral zinc supplementation (25–30 mg as zinc picolinate or bisglycinate daily) supports skin healing from within.
Key Research Papers
- Laureano et al. 2017: Folliculitis: A Comprehensive Review With a Focus on Its Types, Risk Factors, and Treatment. Dermatol Ther (Heidelb). Search PubMed
- Craft N 2004: Superficial cutaneous infections and pyodermas. JAMA. Search PubMed
- Kaplan SL et al. 2012: Randomized trial of "bleach baths" plus routine hygienic measures vs. routine hygienic measures alone for prevention of recurrent infections. Clin Infect Dis. Search PubMed
- Luelmo-Aguilar J, Sánchez-Regaña M 2005: Folliculitis: recognition and management. Int J Dermatol. Search PubMed
- Ahdout J et al. 2012: Erythematous follicular papules and pustules during immunosuppressive therapy. Dermatology. Search PubMed
- Levy PJ et al. 1998: Hot tub folliculitis due to Pseudomonas aeruginosa: case report and review of the literature. Cutis. Search PubMed
- Moehrl P et al. 2017: Eosinophilic folliculitis — an overview. JAMA Dermatol. Search PubMed
- Bassett IB et al. 1990: A comparative study of tea-tree oil versus benzoyl peroxide in the treatment of acne. Med J Aust. PMID: 2145499
- McNamara WF et al. 2007: A comparison of methods for obtaining cultures from children with suspected methicillin-resistant Staphylococcus aureus skin infections. Ann Emerg Med. Search PubMed
- Stulberg DL et al. 2002: Common bacterial skin infections. Am Fam Physician. Search PubMed
PubMed Topic Searches
Curated PubMed searches on folliculitis. Each link opens a live query so you always see the most current studies.
- PubMed: Folliculitis staphylococcal treatment
- PubMed: Malassezia folliculitis
- PubMed: Hot tub Pseudomonas folliculitis
- PubMed: Pseudofolliculitis barbae razor bumps
- PubMed: MRSA decolonization
- PubMed: Furuncle and carbuncle treatment
- PubMed: Eosinophilic folliculitis HIV
- PubMed: Tea tree oil Staphylococcus
- PubMed: Laser hair removal pseudofolliculitis
- PubMed: Gram-negative folliculitis
- PubMed: Zinc skin immunity
- PubMed: Manuka honey MRSA
Connections
- Dermatology
- Acne
- Hidradenitis Suppurativa
- Fungal Infections
- Impetigo
- Erysipelas
- Cellulitis
- Seborrheic Dermatitis
- Rosacea
- Zinc
- Vitamin C
- Turmeric
- Neem