Alopecia: History and Discovery
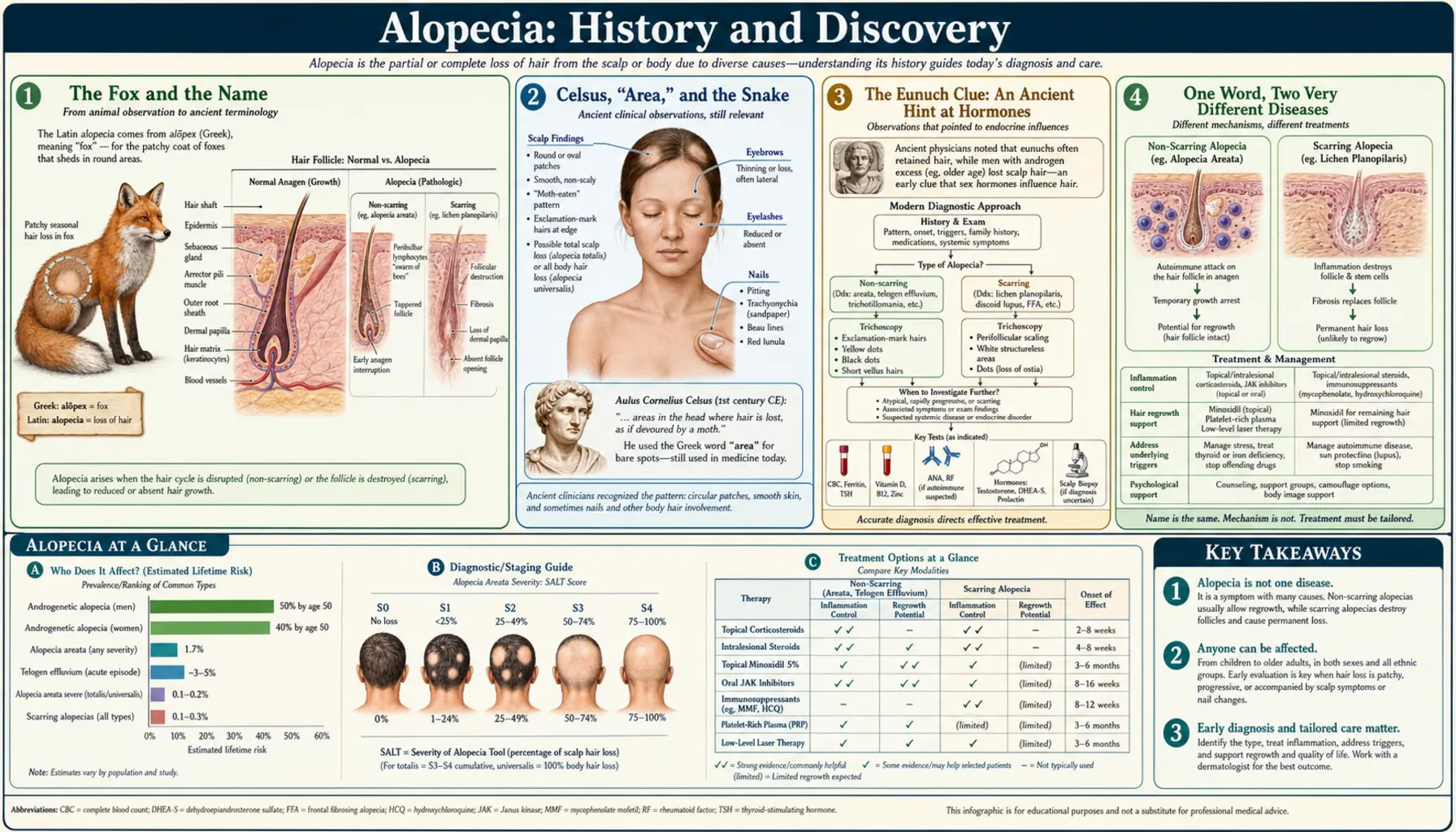
The word alopecia simply means “hair loss,” and its story is really three stories braided together. The name itself comes from the Greek for “fox” — a nod to the mangy fox shedding its coat in patches. Roman and Greek physicians first wrote down the patterns of hair loss two thousand years ago, and even noticed that castrated men do not go bald. But only in the twentieth and twenty-first centuries did medicine learn why hair falls out: that pattern baldness is driven by a hormone, and that alopecia areata is the immune system mistakenly attacking the hair follicle — an insight that led, in 2022, to the first pill ever approved to regrow that lost hair.
Table of Contents
- The Fox and the Name
- Celsus, “Area,” and the Snake
- The Eunuch Clue: An Ancient Hint at Hormones
- One Word, Two Very Different Diseases
- Hamilton, Androgens, and Pattern Baldness
- DHT, Minoxidil, and Finasteride
- Alopecia Areata Revealed as Autoimmune
- The JAK Revolution: First Drugs to Regrow Hair
- Research Papers and References
- Connections
- Featured Videos
The Fox and the Name
The medical word alopecia is one of the oldest disease names still in everyday use, and it carries a small zoological joke inside it. It descends from the ancient Greek alopex (ὦλωποξ), meaning fox. The link is the fox's coat: a fox suffering from mange — a parasitic skin disease — loses its fur in ragged, patchy bald spots. To ancient observers, a person with rounded, scattered patches of missing hair looked rather like a mangy fox, and the Greek term alopekia came to mean exactly that pattern of patchy hair loss. The word passed through Medieval Latin as alopecia and entered English by roughly the fourteenth century, where it has remained the umbrella medical term for hair loss of any cause ever since.
It is worth pausing on what the name does and does not tell us. The Greeks who coined alopex-based terminology were describing an appearance — the look of patchy baldness — not a cause. They had no concept of hormones, immune cells, or genetics. The fox metaphor is a clinical observation frozen into language: hair loss could be named in vivid detail long before anyone could explain a single step of why it happened. That gap between accurate description and true understanding is the central theme of this entire history.
A second naming thread still confuses people today. Alopecia is the general medical word for hair loss, but it is also embedded in the name of one specific disease, alopecia areata — literally “hair loss in patches/areas.” So “alopecia” can mean either the broad category or, in casual speech, that one autoimmune condition. Keeping the two senses straight matters, because the broad category includes very different problems with completely different causes and treatments.
Celsus, “Area,” and the Snake
The first detailed written descriptions of patchy hair loss come from the Roman encyclopaedist Aulus Cornelius Celsus, whose medical work De Medicina dates to roughly the first century CE (commonly cited around 30–47 CE). In Book VI, Celsus laid out what is essentially the earliest surviving clinical classification of hair loss. He used the Latin word area as the general name for the bald places where hair sheds — the source of the modern term alopecia areata — and within that category he distinguished different patterns by their shape.
The pattern that most struck him he called ophiasis, from the Greek for snake (ophis). Celsus described it as a band of baldness, a couple of finger-widths across, that begins at the back of the head and creeps forward along both sides toward the ears and forehead, its two advancing ends meeting like the coils of a serpent winding around the head. Any dermatologist today would recognize this immediately: ophiasis is still the exact word used in 2026 for the band-like pattern of alopecia areata that runs around the lower hairline, and it is known to be more stubborn to treat than scattered patches. A clinical term has survived, essentially unchanged in meaning, for two thousand years.
Celsus described these patterns with real accuracy, but his explanations and treatments belonged firmly to his era: he attributed hair loss to imbalances and offered remedies such as scarifying (scratching) the bald skin and applying caustic preparations to provoke regrowth — ancient medicine at its strengths and limits, superb at naming a pattern but powerless to explain it. The 2020 review by Broadley and colleagues, “A ‘hair-raising’ history of alopecia areata,” traces this descriptive lineage from Celsus forward in detail.
The Eunuch Clue: An Ancient Hint at Hormones
One of the most remarkable observations in the entire history of medicine appears in the Hippocratic Corpus, the body of writings associated with Hippocrates and his followers in the fifth and fourth centuries BCE. The Hippocratic writers noticed a simple but profound fact: eunuchs — castrated men — do not go bald. The often-quoted line holds that eunuchs are subject neither to gout nor to baldness. Aristotle, writing somewhat later, was likewise fascinated by why eunuchs neither lost the hair of their head nor grew the body and chest hair of other men.
This was, in effect, an early empirical glimpse of the link between the male reproductive organs and male-pattern baldness — the connection that we now explain through hormones called androgens. The ancient writers had stumbled onto a genuine cause-and-effect relationship by pure observation: remove the testes before puberty, and pattern baldness does not develop. They could see the correlation with perfect clarity. What they could not do — what no one could do for more than two thousand years — was explain it. The concepts required, such as testosterone and its potent derivative dihydrotestosterone, would not exist until the twentieth century.
The historical poignancy is hard to overstate. As the discovery histories note, this striking eunuch observation lay essentially unexploited for roughly twenty-five centuries before anyone followed it to its biological conclusion. The clue sat in the medical literature the whole time; it could not be cashed in until science had the tools to understand hormones. When the link was finally proven in the 1940s, it was — fittingly — by studying castrated men, exactly the population the Hippocratic writers had pointed to.
One Word, Two Very Different Diseases
Before going further, it is essential to separate two conditions that the single word “alopecia” can blur together, because their histories, causes, and modern treatments diverge completely. Confusing them is one of the most common sources of misinformation about hair loss.
The first is androgenetic alopecia — ordinary male-pattern and female-pattern hair loss, the receding hairline and thinning crown familiar to most families. It is extremely common, increases with age, runs in families, and is driven by a hormone (dihydrotestosterone, or DHT) acting on genetically sensitive follicles. It is not an immune attack and not, in the usual sense, a “disease” of inflammation; the follicles gradually miniaturize and produce finer, shorter hairs. This is the strand the ancient eunuch observation belongs to, and the strand that Hamilton, minoxidil, and finasteride belong to.
The second is alopecia areata — the patchy, sometimes total hair loss that Celsus described as area and ophiasis. It can strike at any age, often suddenly, and can range from a single coin-sized bald spot to complete loss of all scalp hair (alopecia totalis) or all body hair (alopecia universalis). Crucially, it is an autoimmune disease: the body's own immune cells mistakenly attack the hair follicles. This is the strand that the twentieth-century immunologists and the twenty-first-century JAK-inhibitor drugs belong to. The follicle is usually not destroyed but switched off, which is why regrowth is possible. Keeping these two diseases distinct is the single most important idea on this page.
Hamilton, Androgens, and Pattern Baldness
The ancient eunuch clue was finally redeemed by the American anatomist James B. Hamilton. In a landmark 1942 paper in the American Journal of Anatomy, titled “Male hormone stimulation is prerequisite and an incitant in common baldness,” Hamilton demonstrated experimentally what the Hippocratics had merely observed: that androgens are required for male-pattern baldness to develop. Studying men with testicular insufficiency and men who had been castrated, he showed that those lacking testicular androgens did not go bald — even when they had the family history that would normally predict it — and that giving testosterone to such men could trigger balding in those genetically predisposed.
Hamilton distilled this into a rule that still stands: male-pattern baldness depends on the interaction of three factors — androgens, a genetic predisposition, and age. No androgens, no pattern baldness, regardless of genes; but androgens alone are not enough without the inherited susceptibility. (It is worth noting honestly that Hamilton's subjects came in part from a Kansas state institution during an era of coercive sterilization — an ethically troubling context that modern readers should not gloss over even while recognizing the scientific result.) Hamilton went on, in a much-cited 1951 paper in the Annals of the New York Academy of Sciences, to classify the stages and patterns of balding.
That classification became the foundation of the Hamilton–Norwood scale, the standard grading system for male-pattern hair loss. Hamilton's original scheme was revised and expanded by O'Tar Norwood in the 1970s into the seven-stage scale dermatologists and hair-transplant surgeons use today — which is why it carries both men's names. With Hamilton's work, the twenty-five-century-old eunuch observation finally had a mechanism: androgens, acting on susceptible follicles, drive pattern baldness.
DHT, Minoxidil, and Finasteride
Hamilton proved that androgens drive pattern baldness; later work identified the specific culprit as dihydrotestosterone (DHT), a more potent androgen made from testosterone by an enzyme called 5-alpha-reductase. DHT acts on genetically sensitive scalp follicles, causing them to shrink (miniaturize) over successive growth cycles until they produce only fine, barely visible hairs. This mechanistic understanding — testosterone → (5-alpha-reductase) → DHT → follicle miniaturization — is what made it possible to design drugs that actually target the cause of pattern baldness rather than merely cover it up.
The two mainstay treatments arrived by very different routes. Minoxidil was an accident of pharmacology: developed in the 1970s as an oral drug for severe high blood pressure (brand name Loniten), it produced a striking side effect — unwanted hair growth (hypertrichosis) all over the body. Researchers reformulated it as a topical scalp solution, and in 1988 the FDA approved topical minoxidil (Rogaine) as the first drug shown to regrow hair. Exactly how it works is still not fully settled, but it is thought to prolong the follicle's growth phase and improve its blood supply.
Finasteride took the rational, mechanism-based route. It is a 5-alpha-reductase inhibitor: it blocks the enzyme that makes DHT, lowering scalp and blood DHT and thereby slowing or halting follicle miniaturization. First approved at a higher dose for enlarged prostate (as Proscar, 1992), a 1 mg dose was approved by the FDA in December 1997 as Propecia for male-pattern hair loss — the first oral drug proven to treat it in most men. Minoxidil and finasteride remain, decades later, the two best-established treatments for androgenetic alopecia — one discovered by luck, the other engineered straight from the DHT mechanism that Hamilton's androgen insight had opened up.
Alopecia Areata Revealed as Autoimmune
The other great strand of the story — alopecia areata — took a different path to understanding. For centuries it was variously blamed on nerves, infections, or local skin faults. The modern breakthrough was the recognition, consolidated over the twentieth century, that alopecia areata is an autoimmune disease: the immune system mistakes the hair follicle for a threat and attacks it. The hallmark microscopic finding — a swarm of immune cells clustered around the hair bulb, often likened to a “swarm of bees” — pointed clearly to an immune assault, and the disease's well-known tendency to occur alongside other autoimmune conditions (such as thyroid disease and vitiligo) reinforced the picture.
A central organizing idea is the concept of the hair follicle's immune privilege. The growing (anagen) hair bulb normally hides itself from the immune system, partly by switching off the molecular “identity tags” (MHC class I) that immune cells inspect — a protective cloak similar to that enjoyed by the eye and a few other sites. The leading model of alopecia areata, proposed by Paus and colleagues beginning in 1993, holds that this immune privilege collapses: the follicle's disguise fails, hidden follicle proteins are suddenly exposed, and cytotoxic CD8+ T cells move in to attack. It is important to flag this honestly as a working model — very well supported and now central to treatment thinking, but a framework that is still being tested and refined rather than a closed case, and the precise initial trigger (genes plus some environmental stressor) is not fully known.
What makes alopecia areata fundamentally different from pattern baldness — and more hopeful — is that the follicle is generally not destroyed, only switched off and held in a resting state by the immune attack. Call off the attack, and the follicle can wake up and grow hair again. That single fact is why, once scientists understood the precise immune signals driving the assault, it became possible to imagine a drug that could reverse the disease and restore lost hair — something never achievable for the miniaturized follicles of advanced pattern baldness.
The JAK Revolution: First Drugs to Regrow Hair
The decisive turn came in 2014. A team led by Angela Christiano and colleagues at Columbia University published a landmark paper in Nature Medicine — “Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition” — that did two things at once. First, it pinned down the specific immune cells (CD8+NKG2D+ cytotoxic T cells) and the signaling pathway, the JAK-STAT pathway carrying inflammatory cytokines like interferon-gamma and IL-15, that drive the follicle attack. Second, and dramatically, it showed that drugs blocking that pathway — JAK inhibitors — could halt the attack and regrow hair, both in mice and in a first few human patients treated with oral ruxolitinib. For a disease with no reliably effective systemic treatment, this was a genuine turning point.
The clinical payoff arrived in June 2022, when the FDA approved baricitinib (Olumiant), an oral JAK inhibitor, for severe alopecia areata in adults. It was the first systemic medicine ever approved specifically to treat alopecia areata — the first time medicine could offer a pill that, for many patients, regrows hair lost to the disease. In the pivotal trials, a substantial share of patients with extensive loss achieved 80% or more scalp coverage after several months of treatment. After roughly two thousand years of describing the “fox-mange” patches and the snake-like ophiasis, physicians finally had a treatment aimed at the actual cause.
The breakthrough opened a door rather than closing the book. In June 2023 the FDA approved a second JAK inhibitor, ritlecitinib (Litfulo) — notably, the first treatment approved for adolescents (age 12 and up) as well as adults — and in 2024 a third, deuruxolitinib (Leqselvi), for adults. These drugs are not cures; the disease can return when treatment stops, they require monitoring, and they do not help everyone. But the arc is unmistakable: from Celsus naming the patterns he could only describe, through the eunuch clue that waited twenty-five centuries, through Hamilton's hormones and the DHT-targeted drugs for pattern baldness, to an autoimmune mechanism decoded and, at last, drugs that can switch a stalled follicle back on. Alopecia is one of medicine's clearest examples of the long road from accurate description to true understanding to real treatment.
Research Papers and References
The references below combine peer-reviewed histories and landmark studies of alopecia with curated PubMed topic-search links. Where a confident DOI or PMID exists it is given; otherwise a PubMed topic search is provided. The ancient primary sources named in the article — Celsus's De Medicina and the Hippocratic and Aristotelian writings — are cited as historical texts rather than as modern papers. Each external link opens in a new tab.
- Broadley D, McElwee KJ. A “hair-raising” history of alopecia areata. Experimental Dermatology. 2020;29(3):208-222. — doi:10.1111/exd.14073 (PMID: 31960494)
- Hamilton JB. Male hormone stimulation is prerequisite and an incitant in common baldness. American Journal of Anatomy. 1942;71(3):451-480. — doi:10.1002/aja.1000710306
- Hamilton JB. Patterned loss of hair in man: types and incidence. Annals of the New York Academy of Sciences. 1951;53(3):708-728. — doi:10.1111/j.1749-6632.1951.tb31971.x
- Xu XX, et al. (Christiano AM, lab). Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nature Medicine. 2014;20(9):1043-1049. — doi:10.1038/nm.3645 (PMID: 25129481)
- Ayob N, et al. Androgens, hair loss and eugenics: a tale of discovery and American social history. Experimental Dermatology. 2015;24(7):485-486. — doi:10.1111/exd.12702
- Bertolini M, et al. (Paus R). The role of hair follicle immune privilege collapse in alopecia areata: status and perspectives. — PubMed (PMID: 24326544)
- Olumiant (baricitinib): an insight into the FDA-approved systemic treatment for alopecia areata. — PMC9422172
- Celsus, etymology of alopecia, and the history of hair-loss terminology — PubMed: alopecia history, etymology, Celsus, ophiasis
- Hippocrates, eunuchs, androgens, and the discovery of the androgen–baldness link — PubMed: androgenetic alopecia history, eunuchs, androgens
- Finasteride, 5-alpha-reductase, and dihydrotestosterone in androgenetic alopecia — PubMed: finasteride, 5-alpha-reductase, DHT, androgenetic alopecia
- Minoxidil: from antihypertensive to topical hair-regrowth treatment — PubMed: minoxidil hair growth history, hypertrichosis
- Hamilton–Norwood scale and the classification of male-pattern baldness — PubMed: Hamilton–Norwood scale, classification
- Alopecia areata as a tissue-specific autoimmune disease of the hair follicle — PubMed: alopecia areata autoimmune, immune privilege
- JAK inhibitors for alopecia areata — baricitinib, ritlecitinib, deuruxolitinib — PubMed: JAK inhibitors for alopecia areata
External Authoritative Resources
- NIAMS (NIH) — Alopecia Areata
- National Alopecia Areata Foundation (NAAF)
- PubMed — All research on the history of alopecia
Connections
- Dermatology
- Alopecia (main article)
- All Conditions
- Psoriasis
- Vitiligo
- Eczema
- Fungal Infections
- Acne
- Hair Loss — the general symptom this history is about, with its full range of causes.