Valvular Heart Disease: History and Discovery
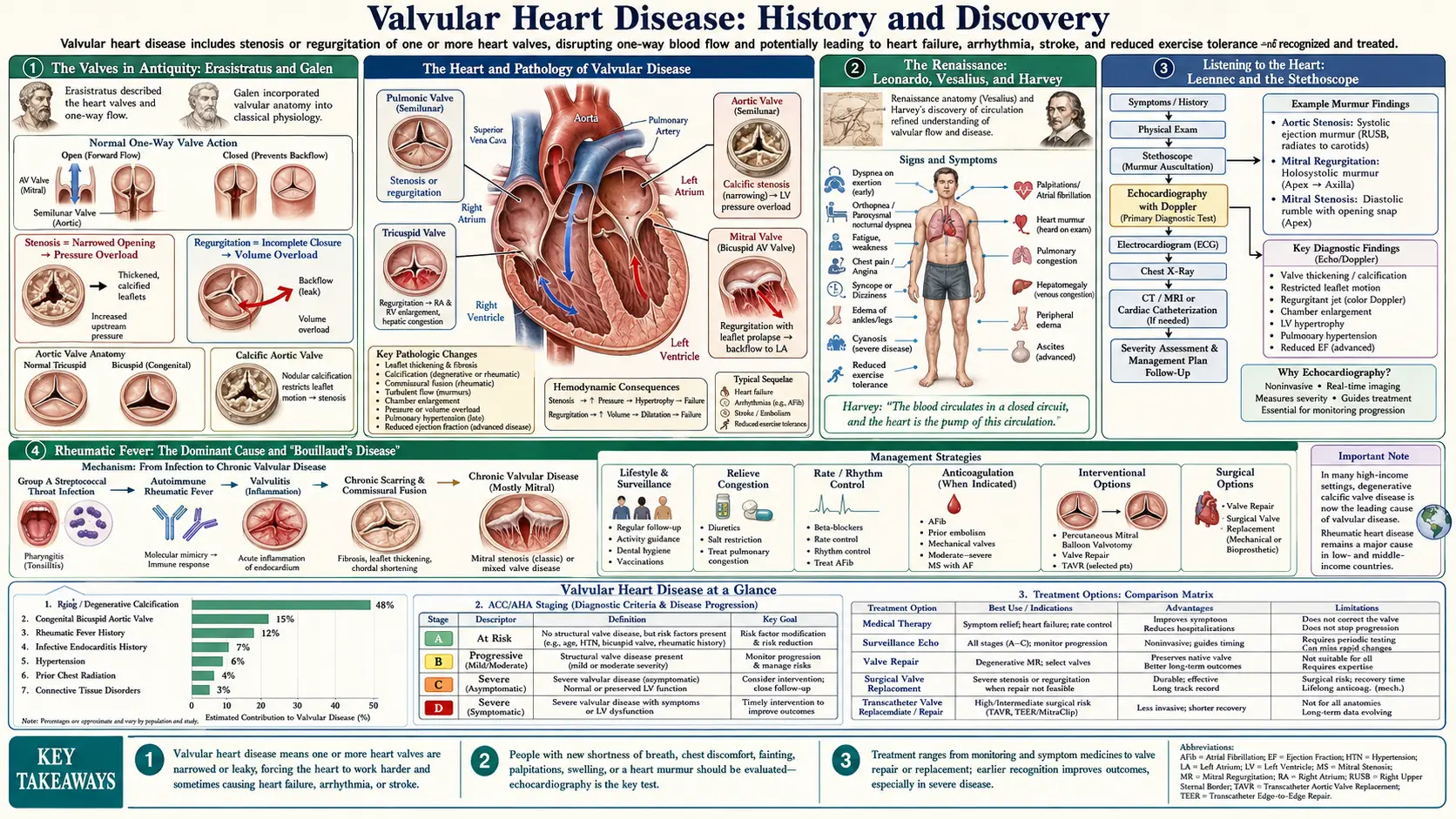
The four valves of the human heart were understood as one-way gates in antiquity, drawn by Renaissance hands, and finally heard at the bedside through Laennec's stethoscope in 1819. For most of recorded history the great destroyer of these valves was rheumatic fever — a delayed immune reaction to a common strep throat — whose link to the heart was traced by Pitcairn, Wells, and above all Bouillaud, after whom acute rheumatic carditis is still called "Bouillaud's disease." The nineteenth century named the physical signs (Corrigan's collapsing pulse of aortic regurgitation, 1832; the Austin Flint murmur, 1862); the twentieth century learned to open, replace, and finally implant a new valve through a catheter. This is the story of how a leaking or narrowed valve went from a death sentence to a routine repair — and of why that triumph is still unevenly shared across the world.
Table of Contents
- The Valves in Antiquity: Erasistratus and Galen
- The Renaissance: Leonardo, Vesalius, and Harvey
- Listening to the Heart: Laennec and the Stethoscope
- Rheumatic Fever: The Dominant Cause and "Bouillaud's Disease"
- The Great Eponyms: Corrigan's Pulse and the Austin Flint Murmur
- The Dawn of Valve Surgery: Cutler, Bailey, and Harken
- The Artificial Valve: Starr-Edwards and Beyond
- The Catheter Revolution: Cribier and TAVR
- A Tale of Two Worlds: The Uneven Decline of Rheumatic Disease
- Research Papers and References
- Connections
- Featured Videos
The Valves in Antiquity: Erasistratus and Galen
The idea that the heart contains valves that allow blood to move in one direction only is remarkably old. In Alexandria in the early third century BCE, the Greek anatomist Erasistratus dissected the heart and recognized that the membranous flaps guarding the chambers act as mechanical valves: once material has left the heart it cannot return the same way, and once it has entered it cannot flow back out. He is credited with distinguishing the structures at the entrances of the ventricles — the three-cusped and two-cusped (tricuspid and bicuspid) valves — and with grasping, centuries before the circulation was understood, that the heart works as a pump whose gates enforce a single direction of flow.
Five hundred years later, Galen of Pergamon (c. 129–216 CE), the most influential physician of the Roman world, inherited and systematized this anatomy from Herophilus and Erasistratus. Galen described the heart's valves and their function in detail, though he embedded them in a now-discarded physiology in which blood was thought to ebb and flow and to pass through invisible pores in the wall between the ventricles. Notably, Galen attributed the naming of the tricuspid valve not to Erasistratus himself but to one of his followers — a small reminder that crediting a discovery to a single person is often a simplification of a longer, more communal process.
What antiquity got right was the mechanical insight: the valves are one-way doors. What it could not yet grasp was the closed loop of circulation that gives those doors their purpose. That second half of the picture would wait nearly two millennia, and the valves themselves — described but not yet truly understood — would be redrawn by the artists and anatomists of the Renaissance.
The Renaissance: Leonardo, Vesalius, and Harvey
The first person to study the heart valves with something approaching modern curiosity was not a physician but an artist-engineer. Leonardo da Vinci (1452–1519) dissected hearts and devoted several pages of his notebooks to the aortic valve. To learn how it closed, he built a glass model of the aortic root and pumped through it a mixture of water and grass seeds, watching the little vortices that swirled in the pouches behind the cusps — the structures now called the sinuses of Valsalva. Leonardo correctly reasoned that these eddies help the valve close, an insight modern fluid-dynamics studies have confirmed. Because he never published, his discoveries had no influence in his own time; they are credited only in retrospect.
The science of anatomy proper begins with Andreas Vesalius, whose De Humani Corporis Fabrica (1543) replaced Galen's often animal-based descriptions with careful human dissection and depicted the cardiac valves with new accuracy. Decades later, in 1628, the English physician William Harvey published De Motu Cordis and demonstrated that blood circulates in a closed loop driven by the heart — finally giving the one-way valves their true reason for being. (Harvey's mentor in Padua, Hieronymus Fabricius, had described the valves of the veins in 1603, a clue Harvey used to build his argument.) Only once circulation was understood could a leaking or narrowed valve be recognized for what it is: a fault in a pump.
These names are given here as historical figures and their landmark works rather than as modern citations. Together they completed the anatomical and physiological foundation — valve structure, valve function, and the circulation those valves serve — on which all later diagnosis and surgery would rest.
Listening to the Heart: Laennec and the Stethoscope
For thousands of years a physician could see and feel the body but could not reliably hear the heart at work. That changed in Paris in 1816, when the French physician René Théophile Hyacinthe Laennec (1781–1826), reluctant to press his ear to a young woman's chest, rolled a sheaf of paper into a tube and discovered he could hear her heartbeat more clearly than ever. From that improvisation he developed a simple wooden cylinder — the first stethoscope — and the technique he called mediate auscultation (listening through an instrument), as opposed to pressing the ear directly to the chest.
In August 1819 Laennec published his great treatise De l'Auscultation Médiate (On Mediate Auscultation), a work so influential it was called the "New Testament of Medicine." In it he catalogued the sounds of the chest — coining terms still used today such as bruit, rales, and egophony — and described the abnormal sounds, the murmurs, produced by diseased heart valves. For the first time, a narrowed or leaking valve produced a sign that could be detected, described, and compared at the living bedside.
This was the hinge on which valvular diagnosis turned. Before Laennec, valve disease was largely a finding at autopsy; after him, the murmur became the central clue, and the nineteenth century became a golden age of bedside cardiology in which physicians learned to read a patient's valves through a tube of wood. The eponymous signs that followed — Corrigan's pulse, the Austin Flint murmur, and many others — are all children of the listening culture Laennec created.
Rheumatic Fever: The Dominant Cause and "Bouillaud's Disease"
For most of recorded medical history, the single greatest cause of valvular heart disease was not aging or birth defects but acute rheumatic fever — a delayed, immune-mediated illness that can follow an untreated throat infection with group A Streptococcus ("strep throat"). In a susceptible person the body's antibodies against the bacterium cross-react with its own tissues, inflaming the joints, skin, brain, and — most dangerously — the heart. Repeated or severe attacks scar the valves, especially the mitral and aortic, leaving them thickened, fused, and either narrowed (stenotic) or leaking (regurgitant) for life. This long-term scarring is called rheumatic heart disease.
The connection between rheumatism and the heart was pieced together in the late eighteenth and early nineteenth centuries. British physicians including David Pitcairn, William Charles Wells, and others (Edward Jenner among them) noted that patients with acute rheumatism often developed heart trouble. The definitive synthesis came from the French physician Jean-Baptiste Bouillaud (1796–1881), who in his 1836 work on acute articular rheumatism established what he called a "law of coincidence" between rheumatic fever and inflammation of the heart's lining and valves. Bouillaud coined the very words endocardium and endocarditis, and to this day acute rheumatic carditis is still called "Bouillaud's disease" in the French medical tradition.
It is worth stressing the chain of causation, because it is the key to the entire story: a common sore throat, left untreated, can in some people trigger an immune attack that, attack by attack, destroys a heart valve over years. Understanding that chain is what eventually made the disease preventable — a simple course of penicillin for strep throat, and long-term penicillin to prevent recurrences, can stop the valve damage before it starts. That insight, and the antibiotics that made it actionable, are the reason rheumatic valve disease has nearly vanished from wealthy countries, as the final section describes.
The Great Eponyms: Corrigan's Pulse and the Austin Flint Murmur
The nineteenth-century bedside produced a gallery of physical signs that let a clinician diagnose a specific leaking or narrowed valve by hand and ear alone. The most famous belongs to the Irish physician Sir Dominic John Corrigan (1802–1880). In 1832, writing in the Edinburgh Medical and Surgical Journal, Corrigan described the dramatic, visibly bounding-then-collapsing pulse of severe aortic regurgitation — the arteries of the neck and arms snapping taut with each beat and then suddenly emptying, because blood leaks back through the failed aortic valve between beats. Though Corrigan described it as a sign of "permanent patency of the mouth of the aorta," the finding became known as the "Corrigan's pulse" (or, after Sir Thomas Watson's vivid comparison to a Victorian water-hammer toy, the "water-hammer pulse").
Three decades later, the American physician Austin Flint (1812–1886) added a subtler clue. In 1862, in his writing on cardiac murmurs, Flint described a low-pitched, rumbling murmur at the apex of the heart in patients with severe aortic regurgitation — a sound that closely mimics the murmur of mitral stenosis even though the mitral valve itself is structurally normal. The Austin Flint murmur is thought to arise because the powerful jet of blood leaking back from the aorta interferes with the opening of the mitral valve, but the exact mechanism remains debated to this day; that uncertainty should be treated as an open question, not a settled fact.
These eponyms matter beyond mere naming. In an era with no imaging, signs like Corrigan's pulse and the Austin Flint murmur were the diagnosis — they told the physician which valve had failed and how badly, and they remain teaching landmarks today even though echocardiography has largely replaced them in practice. They are the high-water mark of a purely clinical cardiology, the art of reading the heart from the outside, just before technology began to let physicians look and then to intervene inside.
The Dawn of Valve Surgery: Cutler, Bailey, and Harken
Operating on a beating heart was long considered reckless, even impossible. The first to try to mechanically relieve a scarred valve was the American surgeon Elliott Carr Cutler, who in 1923 at the Peter Bent Brigham Hospital in Boston, working with the cardiologist Samuel Levine, used a thin knife passed into the heart to split open the fused, rheumatically narrowed mitral valve of a dying twelve-year-old girl. She survived — the world's first successful heart-valve operation — but Cutler's subsequent cases carried a mortality near ninety percent, and he abandoned the technique by 1928. For two decades, valve surgery was regarded as a dead end.
The breakthrough came in 1948, and it came independently from more than one surgeon. On 10 June 1948, Charles P. Bailey in Philadelphia performed a successful closed mitral commissurotomy — reaching a finger or instrument into the beating heart to split the fused valve leaflets — and within days Dwight E. Harken in Boston did the same. (Harken, who had earned his nerve removing shrapnel from soldiers' hearts during the Second World War, refined the approach to spare the valve's delicate leaflets.) Russell Brock in London and Horace Smithy in South Carolina achieved comparable successes in the same period. Crediting a single inventor here would be false: closed mitral commissurotomy was a near-simultaneous, multi-center achievement.
This generation proved that the human heart could be operated on and survive. Their closed operations were soon superseded by open-heart surgery once the heart-lung machine (developed by John Gibbon and first used successfully in 1953) allowed surgeons to stop the heart, open it, and work on the valves under direct vision. With the chamber now safely open, the obvious next ambition was no longer merely to widen a stuck valve but to replace a destroyed one entirely.
The Artificial Valve: Starr-Edwards and Beyond
The first durable, mass-produced artificial heart valve was the Starr-Edwards ball-and-cage valve, the product of an unlikely partnership in Oregon between the young cardiac surgeon Albert Starr and the retired hydraulics engineer Miles Lowell Edwards. After abandoning attempts to copy the natural leaflet shape, they settled on a deceptively simple design: a small silicone-rubber ball trapped in a metal cage. When the heart pushed blood forward the ball lifted to let it pass; when blood tried to flow backward the ball dropped against a ring and sealed the opening — a one-way valve made of a ball in a cup. In 1960, Starr implanted it in the mitral position in a patient who went on to live an active life for roughly a decade. It was the first artificial valve produced and used on a large scale, and tens of thousands were implanted worldwide.
The Starr-Edwards valve solved the central problem — a failed valve could now be removed and replaced — but it created new ones, chiefly the lifelong need for blood-thinning drugs to prevent clots from forming on the metal and the destruction of red blood cells by the moving ball. The decades that followed were a long refinement: tilting-disc valves (such as the Björk-Shiley) and then low-profile bileaflet mechanical valves (the St. Jude Medical valve, introduced in 1977, became the workhorse) offered better flow, while bioprosthetic valves made from treated pig or cow tissue (pioneered commercially by Edwards' own company and by Alain Carpentier's glutaraldehyde-fixation work) avoided lifelong anticoagulation at the cost of shorter durability.
A parallel idea was to use the patient's own living tissue: in 1967 the South African surgeon Donald Ross described moving the patient's healthy pulmonary valve into the aortic position (the "Ross procedure") and replacing the pulmonary valve with a graft. By the late twentieth century a surgeon could choose among mechanical, animal-tissue, and human-tissue valves — a rich menu unimaginable to Cutler's generation. Yet every option still required open-heart surgery, with its chest incision and heart-lung bypass — too great a risk for many of the frail, elderly patients in whom valve disease is most common. That barrier set the stage for the last revolution.
The Catheter Revolution: Cribier and TAVR
The boldest idea in modern valve treatment was to replace a valve without opening the chest at all — threading a collapsed artificial valve up through an artery on the tip of a catheter and expanding it inside the diseased valve, where it pushes the old leaflets aside and takes over. For years this was dismissed as impossible: surely a valve crimped onto a balloon could never anchor securely in the high-pressure aorta. The French cardiologist Alain Cribier (1945–2024), who had already performed the first balloon aortic valvuloplasty in 1986, refused to accept that it could not be done.
On 16 April 2002, at the Charles Nicolle University Hospital in Rouen, France, Cribier performed the world's first transcatheter aortic valve replacement — known as TAVR or TAVI — on a 57-year-old man with severe aortic stenosis who was dying in cardiogenic shock and had been turned down for surgery. The catheter-delivered valve restored his circulation, and he recovered within days. It was a single desperate case, performed because nothing else could save the patient, but it proved the principle on which an entire field would be built.
In the two decades since, TAVR has moved from a last resort for inoperable patients to a mainstream treatment, supported by large randomized trials (the PARTNER and CoreValve programs) that progressively extended it from high-risk to intermediate- and then low-risk patients with aortic stenosis. For an elderly person with a calcified aortic valve, a procedure that once meant a sternotomy and weeks of recovery can now be an overnight stay. Cribier's 2002 case stands beside Cutler's 1923 operation and Starr's 1960 valve as one of the true turning points in the history of valvular heart disease.
A Tale of Two Worlds: The Uneven Decline of Rheumatic Disease
The history above is largely a story of triumph — but it is a triumph unevenly shared. In wealthy countries, the dominant cause of valve disease for centuries, rheumatic fever, has all but disappeared. Antibiotics to treat strep throat and to prevent rheumatic recurrences, combined with better housing, less crowding, and improved nutrition, caused rheumatic heart disease to virtually vanish from high-income settings by the late twentieth century. In those countries, valve disease today is largely a problem of aging — calcific narrowing of the aortic valve and degeneration of the mitral valve — which is precisely the population TAVR and modern repair were designed to serve.
Across much of the rest of the world, the older story has never ended. Rheumatic heart disease still affects on the order of 40 to 55 million people globally, the overwhelming majority in low- and middle-income countries and among disadvantaged communities — including Indigenous populations — within wealthy ones. It remains the most common acquired heart disease in children and young adults worldwide, striking people in the prime of life with a condition that penicillin could have prevented for pennies. The cruel irony is that the disease is both preventable and, where it occurs, hardest to treat: the children who develop it are least likely to have access to the valve surgery and transcatheter technology that the same era of medicine has perfected.
This is the honest shape of the history of valvular heart disease. The science is extraordinary — from Erasistratus' one-way gates to a replacement valve delivered by catheter in a single afternoon. But the burden of the disease now tracks the fault lines of global inequality as much as biology. The unfinished work is not only better valves; it is delivering the simple, century-old prevention — treating strep throat — to every child who needs it. Until that gap closes, the triumphant half of this story and the tragic half will continue to be lived on different continents at the same time.
Research Papers and References
The references below combine peer-reviewed historical and clinical reviews (with DOIs or PubMed/PMC identifiers where confidently verified) with curated PubMed topic-search links into the history of valve anatomy, auscultation, rheumatic heart disease, and valve surgery. Historical primary works named in the article — Galen's anatomical writings, Vesalius's De Humani Corporis Fabrica (1543), Harvey's De Motu Cordis (1628), Laennec's De l'Auscultation Médiate (1819), Corrigan's 1832 paper, Bouillaud's 1836 work, and Flint's 1862 writings — are cited as historical sources rather than as modern journal articles. Each link opens at the publisher or at PubMed (National Library of Medicine) in a new tab.
- Roguin A. Rene Theophile Hyacinthe Laënnec (1781–1826): the man behind the stethoscope. Clinical Medicine & Research. 2006;4(3):230–235. — PMC1570491
- Robicsek F. Leonardo da Vinci and the sinuses of Valsalva. The Annals of Thoracic Surgery. 1991;52(2):328–335. — doi:10.1016/0003-4975(91)91371-2
- Cohn LH. Fifty years of open-heart surgery. Circulation. 2003;107(17):2168–2170. — doi:10.1161/01.CIR.0000071746.50876.E2
- Cohn LH, Soltesz EG. The evolution of mitral valve surgery: 1902–2002. The American Journal of Cardiology / historical reviews of Cutler, Bailey, and Harken — PubMed: Bailey and Harken, the dawn of modern mitral valve surgery
- Gonzalez-Lavin L. The first successful surgical treatment of mitral stenosis: the 70th anniversary of Elliot Cutler's mitral commissurotomy. The Annals of Thoracic Surgery. 1993;56(5):1198–1202. — PubMed: 8239828
- Matthews AM. The development of the Starr-Edwards heart valve. Texas Heart Institute Journal. 1998;25(4):282–293. — PMC325572
- Cribier A. The development of transcatheter aortic valve replacement (TAVR). Comptes Rendus Biologies / historical first-person account — PubMed: Cribier, development of TAVR
- Cribier A, Eltchaninoff H, Bash A, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation. 2002;106(24):3006–3008. — doi:10.1161/01.CIR.0000047200.36165.B8
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. New England Journal of Medicine. 2017;377(8):713–722. — doi:10.1056/NEJMoa1603693
- Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nature Reviews Disease Primers. 2016;2:15084. — doi:10.1038/nrdp.2015.84
- Flint and Corrigan eponyms — aortic regurgitation physical signs in historical context — PubMed: Corrigan's pulse and Austin Flint murmur, historical
- Bouillaud, rheumatic fever, and the history of endocarditis — PubMed: Bouillaud and the history of rheumatic carditis
- Erasistratus, Galen, and the ancient understanding of the cardiac valves — PubMed: Erasistratus and Galen on the heart valves
- History of prosthetic and transcatheter heart-valve development — PubMed: history of prosthetic heart valves
External Authoritative Resources
- American Heart Association — Heart Valve Problems and Disease
- NHLBI (NIH) — Heart Valve Diseases
- PubMed — History of valvular heart disease
Connections
- Cardiology
- Valvular Heart Disease
- Endocarditis
- Heart Failure
- Arrhythmia
- Atrial Fibrillation
- Cardiomyopathy
- All Conditions