Peripheral Artery Disease: History and Discovery
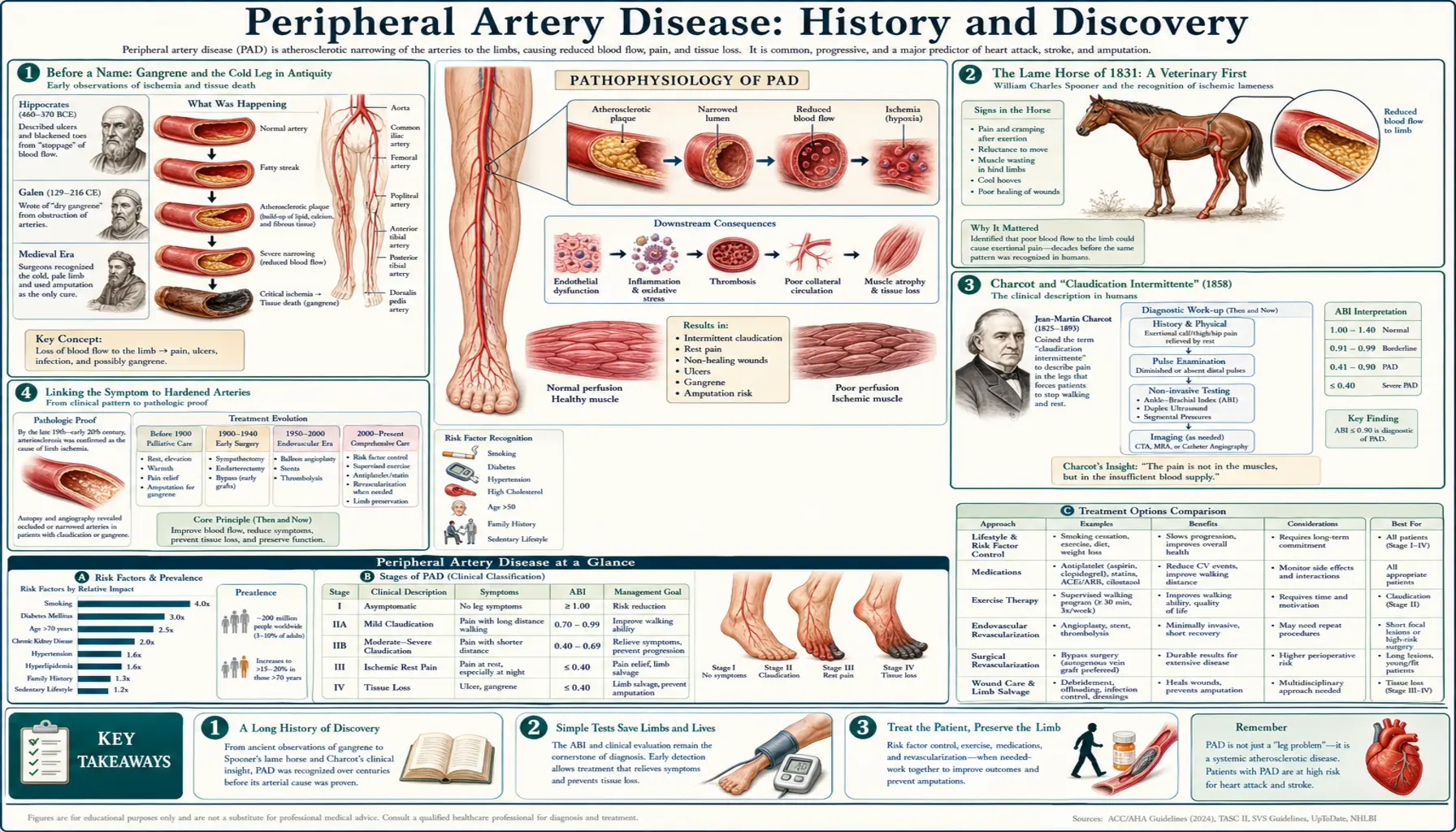
Peripheral artery disease (PAD) is the slow, atherosclerotic narrowing of the arteries that carry blood to the limbs — most often the legs. Its signature symptom is intermittent claudication: a cramping, aching tightness in the calf, thigh, or buttock that comes on with walking and eases within minutes of rest. The story of how this everyday complaint was recognized, named, traced to hardened arteries, and finally treated runs from a lame Parisian carriage-horse in 1831, through the French neurologist Jean-Martin Charcot's 1858 description of "claudication intermittente," to the surgeons and radiologists of the twentieth century who learned to image, bypass, scrape, and balloon-open the blocked vessel. This page tells that history with care for who described what, and when — distinguishing the naming of the symptom from the eponymous syndromes and the treatments that followed.
Table of Contents
- Before a Name: Gangrene and the Cold Leg in Antiquity
- The Lame Horse of 1831: A Veterinary First
- Charcot and "Claudication Intermittente" (1858)
- Linking the Symptom to Hardened Arteries
- Buerger's Disease: A Distinct Related Entity (1908)
- Leriche and the Aortoiliac Syndrome (c. 1940)
- Seeing and Measuring the Blockage: Arteriography and the ABI
- The Surgical Era: Endarterectomy and Bypass
- Dotter, Grüntzig, and the Endovascular Revolution
- Research Papers and References
- Connections
- Featured Videos
Before a Name: Gangrene and the Cold Leg in Antiquity
Long before anyone understood that arteries could silently fur up and choke off the blood supply to a limb, physicians recognized its end result. The dreaded black, dead tissue of gangrene — the limb that grows cold, pale, painful, and finally rots — appears in the writings attributed to Hippocrates and in the Roman encyclopedist Celsus. What they lacked was any way to connect a living person's cramping, claudicating leg with the hardened, blocked vessel found later at autopsy. For most of recorded history, the cold, pulseless, gangrenous limb was treated as it presented — with amputation, cautery, or resignation — not as the final chapter of a long arterial disease.
The conceptual leap required two things classical and medieval medicine lacked: a clear picture of the circulation, and the habit of comparing a patient's symptoms in life with the diseased artery found after death. The first arrived with William Harvey's demonstration of the circulation of the blood in 1628. The second — the systematic correlation of symptoms with autopsy findings — matured only in the eighteenth and nineteenth centuries, above all in the great Paris hospitals where the modern understanding of PAD would take shape. These are well-established landmarks named here as historical context, not as claims about who "discovered" PAD.
The Lame Horse of 1831: A Veterinary First
One of the more surprising facts in the history of vascular medicine is that intermittent claudication of arterial origin was first clearly described not in a person but in a horse. In 1831, the French veterinary surgeon Jean-François Bouley (often called Bouley jeune, "the younger") described a carriage-horse in the streets of Paris that would begin to limp after being driven a certain distance, recover with rest, and then limp again — and he connected this on-and-off lameness to disease of the arteries supplying the limb. The veterinary anatomist Goubaux is associated with the same line of observation. This veterinary description is well attested across modern historical reviews and is the genuine "first" for arterial intermittent claudication as a recognized clinical pattern.
This matters for two reasons. First, it is the literal origin of the term that would later define human PAD: when Charcot named the human syndrome, he explicitly borrowed the word "claudication" and the concept from this veterinary literature. Second, it is a clean early example of the on-walking/off-resting rhythm that is the diagnostic heart of claudication — the working muscle outruns its narrowed blood supply, pain forces a halt, rest repays the small oxygen debt, and the cycle repeats. Because the horse came first, the condition is sometimes historically styled the Bouley–Charcot claudication, crediting both the veterinary observer and the physician who carried the idea to human medicine.
Charcot and "Claudication Intermittente" (1858)
The figure most responsible for placing intermittent claudication in human medicine is Jean-Martin Charcot (1825–1893), the towering Paris neurologist of the Salpêtrière. In 1858, Charcot gave the first detailed account of intermittent claudication in a human patient, presenting it to the Société de Biologie; the work was published in the Gazette médicale de Paris in 1859. He named the condition "claudication intermittente" — intermittent limping — drawing the term from the Latin claudicare, "to limp" (the root also of the English "claudication" and, distantly, of the name of the lame emperor Claudius). Charcot consciously adopted the name from the veterinary descriptions of the limping horse discussed above.
Charcot's contribution was not merely to label the symptom but to interpret it correctly. He recognized that the walking-induced leg pain reflected an inadequate arterial blood supply to the exercising muscle — that the limb's circulation was sufficient at rest but failed under the increased demand of exertion. In doing so he tied the everyday complaint to disease of the arteries, setting the symptom on the path to being understood as the herald of what we now call peripheral artery disease. This is the load-bearing fact of the page: Charcot, 1858, named and clinically defined intermittent claudication and linked it to arterial insufficiency.
A point of historical honesty is worth making here. Charcot named and explained the symptom; he did not "discover" atherosclerosis, nor did he coin the modern disease label "peripheral artery disease," which is a twentieth-century umbrella term. The condition's understanding developed cumulatively across the nineteenth and twentieth centuries, with pathologists, surgeons, and physiologists each adding a layer. Charcot's 1858 description is the keystone of the clinical story — the moment the limping leg acquired a name and a correct mechanism — but it sits within a much longer collaborative effort.
Linking the Symptom to Hardened Arteries
Recognizing that the cramping leg signaled poor arterial flow was one step; understanding why the artery had narrowed was another, and it came from the pathologists. Across the eighteenth and nineteenth centuries, anatomists described arteries stiffened, thickened, and clogged with yellowish, gruel-like deposits and chalky calcification — the lesion that the German pathologist Felix Marchand would, in the early twentieth century, name atherosclerosis (from the Greek athērōma, "porridge" or "gruel," plus sklērosis, "hardening"), capturing both the soft, fatty core and the hard, fibrous cap of the mature plaque. PAD came to be understood as this same systemic disease of arteries, expressed in the vessels of the limbs.
This reframing was profound. It meant that intermittent claudication was not a local quirk of the leg but a window onto a body-wide process: the person whose calf cramps after two blocks very often has the same plaque building in the coronary arteries of the heart and the carotid arteries to the brain. The modern recognition that PAD travels with coronary artery disease and stroke risk — that a low ankle pressure predicts heart attacks, not just sore legs — is the direct descendant of this nineteenth-century insight that one disease, atherosclerosis, lies beneath them all. The companion article on Atherosclerosis traces the plaque itself in detail.
It is also worth noting that not every blocked limb artery is atherosclerotic. Clinicians of the era had to learn to distinguish the slow, plaque-driven narrowing of classic PAD from sudden arterial embolism (a clot lodging abruptly), from vasospastic conditions such as Raynaud's phenomenon, and from the inflammatory vessel disease described next. Sorting these apart — the chronic from the acute, the atherosclerotic from the inflammatory — was a major achievement of nineteenth- and early-twentieth-century vascular medicine.
Buerger's Disease: A Distinct Related Entity (1908)
Among the conditions that had to be separated from ordinary atherosclerotic PAD is a striking inflammatory disease of the small and medium arteries (and veins) of the limbs, strongly tied to tobacco. It was first sketched by the Austrian surgeon Felix von Winiwarter in 1879, who described a "presenile spontaneous gangrene" in a young man's foot that did not fit the usual picture of arteriosclerosis. The decisive account came in 1908, when the American physician Leo Buerger (1879–1943), working in New York, published a detailed clinical and pathological study in the American Journal of the Medical Sciences and gave the disease its enduring scientific name, thromboangiitis obliterans — literally, inflammation-with-clot that obliterates the vessel.
Buerger drew his pathology from eleven amputated limbs and described the condition's hallmarks so precisely that, as later commentators noted, little of substance has been added in the century since: onset in young people (typically men under 40), heavy cigarette use, painful ischemia of the hands and feet with progression to ulceration and gangrene, migratory superficial thrombophlebitis, and a striking sparing of the larger central arteries. Because it produces claudication and limb-threatening ischemia, Buerger's disease sits beside PAD in the differential diagnosis — but it is a separate entity: inflammatory rather than atherosclerotic, affecting younger smokers, and managed above all by absolute, lifelong tobacco cessation rather than by the plaque-directed strategies used for atherosclerotic PAD. Including it here marks the boundary of what "peripheral artery disease" does and does not mean.
Leriche and the Aortoiliac Syndrome (c. 1940)
If Charcot owns the symptom, the great French surgeon René Leriche (1879–1955) owns one of the most important eponymous syndromes of PAD. Leriche described the clinical picture produced when atherosclerosis blocks the lowest part of the aorta and its division into the iliac arteries — the very top of the leg's arterial tree. The condition, formally crystallized in his writing around 1940 and ever since called Leriche syndrome (aortoiliac occlusive disease), is defined by a classic triad: claudication felt high up in the buttocks, hips, and thighs; weak or absent femoral pulses in the groin; and erectile dysfunction in men, all flowing from the same blockage at the aortic fork.
Leriche's importance went beyond naming a pattern. He argued, against the surgical caution of his day, that this was a mechanical problem of a blocked pipe that might one day be relieved surgically — a vision realized by his own pupils. (Historians note that scattered earlier descriptions of aortic-bifurcation occlusion exist, with Robert Graham sometimes credited as early as 1813; the full clinical syndrome is nonetheless Leriche's.) Leriche also championed the broader idea that the diseased, occluded artery and its associated pain could be approached surgically, and he trained the surgeons who turned that idea into operations. One of them, Jean Kunlin, would perform the first modern bypass; Leriche's own work on the sympathetic nervous system and on what he called the surgery of pain rounds out a career that did much to create vascular surgery as a discipline.
Seeing and Measuring the Blockage: Arteriography and the ABI
Treating a blocked artery requires first finding it, and the twentieth century delivered two complementary tools: a way to photograph the arteries, and a way to measure the pressure they could deliver. The imaging breakthrough was arteriography (angiography) — injecting a radio-opaque contrast agent so the arteries cast a shadow on an X-ray. Building on António Egas Moniz's cerebral angiography of 1927, the Portuguese physician Reynaldo dos Santos performed the first translumbar aortography in Lisbon in 1929, injecting contrast directly into the aorta to reveal the abdominal and limb arteries. For the first time, a surgeon could see the map of a patient's blockage before operating, rather than discovering it with a knife.
The pressure-measurement breakthrough was the ankle-brachial index (ABI), which remains the everyday bedside test for PAD. Its core idea — comparing the blood pressure at the ankle with that in the arm — was described by Travis Winsor in 1950 in a paper on "the influence of arterial disease on the systolic blood pressure gradients of the extremity," and the ratio is still sometimes called the Winsor index. (An earlier related pressure-index concept is attributed to Nauman around 1930.) In a healthy person, ankle pressure equals or exceeds arm pressure, giving a ratio near or above 1.0; when plaque narrows the leg arteries, ankle pressure falls and the ratio drops — below about 0.90 is diagnostic of PAD, and the lower it goes, the more severe the disease. Cheap, painless, and quantitative, the ABI turned PAD from something inferred from a story and a faint pulse into something measured with a blood-pressure cuff and a handheld Doppler.
These two advances — the picture and the number — transformed diagnosis. Arteriography (and later its gentler descendants: ultrasound Doppler, CT angiography, and MR angiography) showed surgeons exactly where and how long the blockage was, while the ABI gave a fast, repeatable severity score trackable over time in any clinic. Together they made the modern, staged management of PAD possible.
The Surgical Era: Endarterectomy and Bypass
With the artery now visible on film, surgeons devised two fundamentally different ways to restore flow: clean the blocked pipe out, or route around it. The first approach, endarterectomy (more fully, thromboendarterectomy), means opening the artery and peeling out the obstructing plaque-and-clot core, leaving the cleaned vessel to carry blood again. Its modern birth is credited to the Portuguese surgeon João Cid dos Santos — son of the arteriography pioneer Reynaldo dos Santos — who performed the first successful thromboendarterectomy in 1946 (publishing his work on "the disobliteration of old arterial thromboses" in 1947), aided by the then-new anticoagulant heparin that kept the cleaned vessel from immediately re-clotting.
The second approach, bypass grafting, leaves the blockage in place and builds a detour around it. The landmark operation is the femoropopliteal bypass, first performed by Jean Kunlin — a pupil of Leriche in Strasbourg — on 3 June 1948. Kunlin used a length of the patient's own saphenous vein to carry blood from the femoral artery in the groin, around a long thigh blockage, down to the popliteal artery behind the knee. Crucially, he sewed the graft end-to-side rather than cutting the native artery in two, preserving collateral branches and anchoring the join in healthier vessel — a refinement that helped the operation succeed where earlier attempts had failed. The femoropopliteal vein bypass became, and largely remains, a workhorse of limb salvage in severe PAD.
For the blockage at the very top — Leriche's aortoiliac syndrome — surgeons developed aortobifemoral bypass, in which a synthetic graft carries blood from the aorta to both groins, directly answering the problem Leriche had described decades earlier. Together, endarterectomy and bypass gave vascular surgeons a genuine, durable answer to severe claudication, rest pain, and threatened limbs, and for forty years they were the definitive treatments for serious PAD. They remain essential today for the most extensive disease, even as less-invasive techniques have taken over many cases.
Dotter, Grüntzig, and the Endovascular Revolution
The most far-reaching change in PAD treatment was the realization that a blocked artery might be reopened from inside, through a needle-puncture rather than a surgical incision. The pioneer was the American interventional radiologist Charles Dotter, who — with his trainee Melvin Judkins — performed the first deliberate percutaneous transluminal angioplasty on 16 January 1964. The patient, Laura Shaw, was an 83-year-old woman with a painful, threatened leg and gangrenous toes who had refused amputation; Dotter threaded progressively larger catheters across a tight narrowing in her superficial femoral artery (a leg vessel), widened it, and restored flow. This is the load-bearing date of the endovascular story: Dotter and Judkins, 1964, opened a peripheral artery from within for the first time on purpose.
Dotter's coaxial-dilator technique drew skepticism in the United States — he was nicknamed "Crazy Charlie" — but it caught fire in Europe, where the Swiss-trained German cardiologist Andreas Grüntzig took the crucial next step. Grüntzig replaced the rigid dilators with a balloon on the catheter tip: inflated at the blockage, it crushed and stretched the plaque outward, then deflated to be withdrawn. He performed his first peripheral (femoral) balloon angioplasty on 12 February 1974 and the first iliac-artery dilation weeks later. Grüntzig then carried the same balloon idea to the heart, performing the first coronary balloon angioplasty on a conscious patient on 16 September 1977 in Zürich — the procedure that launched modern interventional cardiology. The same technology thus revolutionized the treatment of both the legs and the heart.
From Grüntzig's balloon flowed the entire modern endovascular toolkit: bare-metal and drug-eluting stents that scaffold the artery open, drug-coated balloons, atherectomy devices that shave or drill out hard plaque, and dedicated systems for the small arteries below the knee. For a great many people with PAD today, the blockage is treated in an angiography suite through a tiny groin or wrist puncture, with the patient awake and home within a day — the direct legacy of a horse in 1831, a name coined in 1858, and a refused amputation in 1964. Practical, present-day management — walking programs, risk-factor control, medications, and when to choose surgery versus stenting — is covered on the main Peripheral Artery Disease page.
Research Papers and References
The references below combine peer-reviewed historical reviews with curated PubMed topic-search links into the original and secondary literature on the history of intermittent claudication, Leriche syndrome, Buerger's disease, and the development of vascular imaging, surgery, and angioplasty. Historical primary texts (Charcot's 1858–1859 reports, Buerger's 1908 paper, Leriche's writings, and Cid dos Santos's 1947 publication) are named in the article as historical sources. Each link opens in a new tab; where a stable DOI or PubMed record is cited it is given directly, otherwise a PubMed topic search is provided.
- Shamsuddin AHM, et al. (historical review). Charcot and claudicatio intermittens — a footnote to the history of vascular surgery. PubMed record — PubMed: PMID 11639435
- Did Jean-Martin Charcot Contribute to Stroke? (Charcot, claudication, and vascular neurology). European Neurology. — doi:10.1159/000315032
- Olin JW. Thromboangiitis Obliterans (Buerger's Disease). New England Journal of Medicine. 2000;343(12):864-869. — doi:10.1056/NEJM200009213431207
- Buerger's Disease: Thromboangiitis Obliterans 100 Years After the Initial Description. American Journal of the Medical Sciences. — PubMed: Buerger's disease 100 years on
- Tan SY, Hu M. René Leriche (1879–1955): innovator of vascular surgery. Singapore Medical Journal / PMC. — PMC4415095
- Barker WF (and others). Alexis Carrel, Rene Leriche, Jean Kunlin, and the history of bypass surgery. Journal of Vascular Surgery. 2011. — doi:10.1016/j.jvs.2011.06.110
- Friedman SG, et al. Jean Kunlin and the first femoropopliteal bypass (1948) — history of vascular reconstruction. — PubMed: Kunlin femoropopliteal bypass history
- Cid dos Santos and the origin of thromboendarterectomy (1946–1947). — PubMed: dos Santos endarterectomy history
- Friedman SG. Charles Dotter: the father of intervention (first transluminal angioplasty, 1964). PMC. — PMC101126
- King SB 3rd. Balloon Angioplasty — The Legacy of Andreas Grüntzig, M.D. (1939–1985). Frontiers in Cardiovascular Medicine. 2014;1:15. — doi:10.3389/fcvm.2014.00015
- Aboyans V, et al. Measurement and Interpretation of the Ankle-Brachial Index (history and method; Winsor 1950). Circulation. 2012;126(24):2890-2909. — doi:10.1161/CIR.0b013e318276fbcb
- Reynaldo dos Santos and the first translumbar aortography (1929) — history of vascular imaging. — PubMed: dos Santos aortography history
- Origin and history of the term intermittent claudication (Bouley, Charcot, arteriosclerosis). — PubMed: intermittent claudication history
- History of peripheral arterial disease — diagnosis, surgery, and endovascular treatment. — PubMed: peripheral artery disease history
External Authoritative Resources
- NHLBI (NIH) — Peripheral Artery Disease
- PubMed — PAD and intermittent claudication, history
- American Heart Association — Ankle-Brachial Index statement
Connections
- Cardiology
- Peripheral Artery Disease (main page)
- Atherosclerosis
- Aortic Aneurysm
- Coronary Artery Disease
- Stroke
- Diabetes
- All Conditions