Hypertension: History and Discovery
Hypertension — persistently high blood pressure — has no single inventor or discoverer. There is no one person, no single year, and no lone "eureka" moment behind it. It is instead a cumulative discovery, assembled over nearly three centuries by many different people working in different countries: a clergyman who first measured the force of blood, a physician who tied it to diseased kidneys, doctors who learned to read it from a pulse and then from a stethoscope, an engineer-physician who built the arm cuff, and finally the epidemiologists and trialists who proved that high pressure is dangerous and that treating it saves lives. This page traces those real milestones honestly — separating the story of how we learned to measure blood pressure from the story of how we came to understand high blood pressure as a disease — and it is careful to call a verified fact a fact and a historical idea an idea.
Table of Contents
- A Disease With No Single Inventor
- Stephen Hales Measures the Pressure (1733)
- Richard Bright and the Kidney Link (1836)
- Mahomed and High Pressure as Its Own Disease
- Riva-Rocci and the Arm Cuff (1896)
- Korotkoff and the Sounds (1905)
- "Essential Hypertension" and the Framingham Era
- Proving That Treatment Works (the VA Trials)
- Modern Understanding
- Research Papers and References
- Connections
- Featured Videos
A Disease With No Single Inventor
It is tempting to ask "who discovered high blood pressure?" and expect a name and a date, the way we say Fleming discovered penicillin. But hypertension does not have that kind of origin story, and it would be dishonest to invent one. High blood pressure is invisible and silent; you cannot see it, feel it, or point to it the way you can a broken bone or a rash. Before anyone could call it a disease, humanity first had to learn that blood travels under pressure at all, then build instruments to measure that pressure, then gather enough people's readings over enough years to learn that a high number quietly shortens lives. Each of those steps took different people, decades apart.
So the honest answer is that hypertension was discovered cumulatively, by a long relay of investigators handing the problem from one generation to the next. It is useful to keep two threads separate as the story unfolds. One thread is about measurement — the slow invention of ways to put a number on blood pressure, from a frightening glass tube in a horse's artery to the soft cuff on your arm today. The other thread is about the disease concept — the gradual realization that some people's pressure is chronically too high, that this harms the heart, brain, kidneys, and arteries, and that lowering it prevents that harm. The two threads are braided together but they are not the same, and confusing them is the source of most of the myths about who "found" hypertension.
This page follows both threads in roughly the order they happened. Where a name, year, or "first" is well documented we state it plainly. Where the historical record is genuinely uncertain — for example, the exact year a term was coined, or whether a given doctor was truly "first" — we say so, rather than smoothing it over. The goal is an accurate map of how an invisible killer slowly became one of the most measured, most studied, and most treatable conditions in all of medicine.
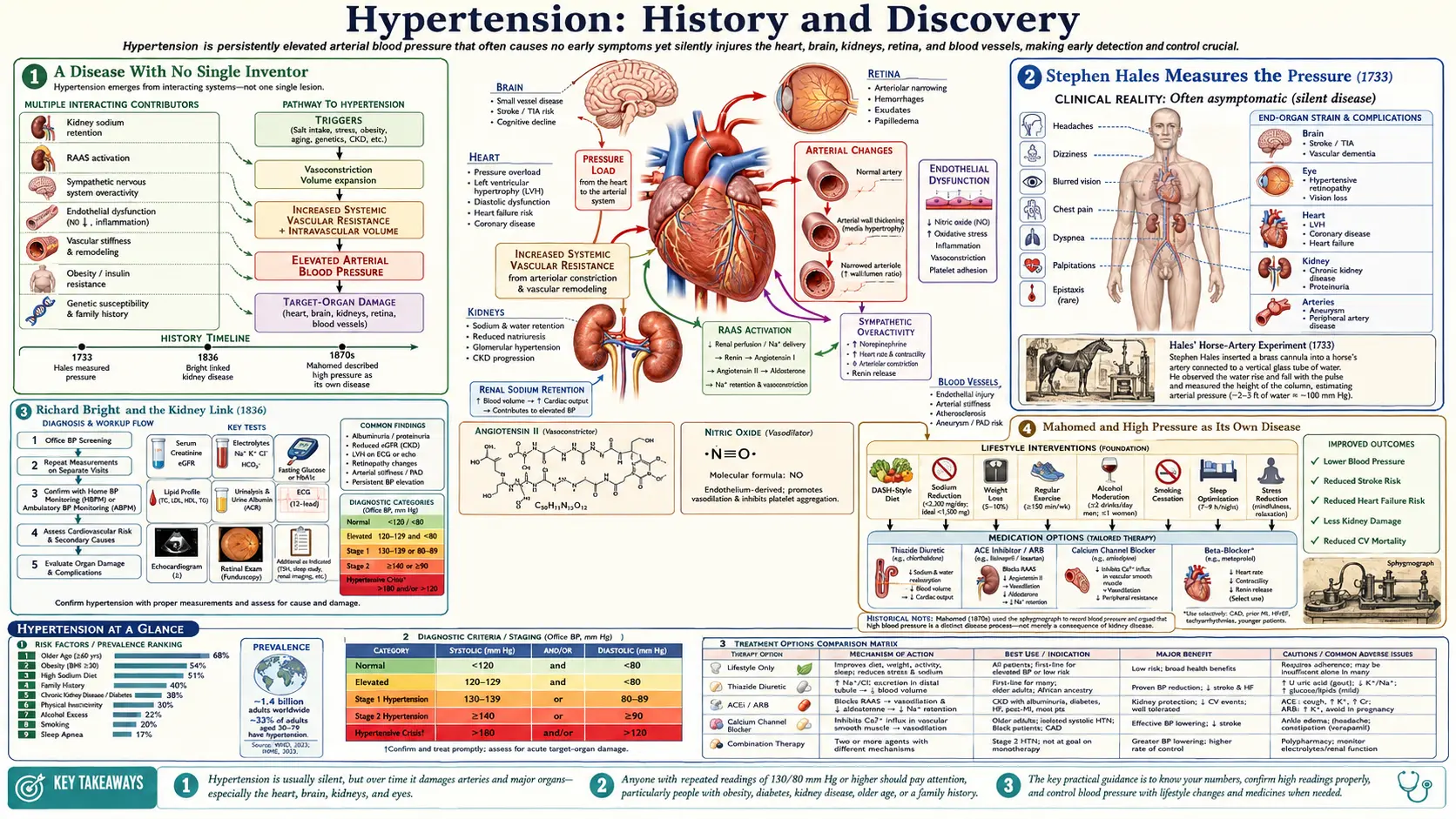
Stephen Hales Measures the Pressure (1733)
The measurement thread begins, remarkably, with an English country clergyman. The Reverend Stephen Hales (1677–1761), a curate at Teddington and a gifted amateur scientist, performed in 1733 what is generally credited as the first direct measurement of arterial blood pressure. The subject was not a human being but a horse. Hales tied down a living horse, opened an artery in its leg (and in other experiments the neck), and connected it by a brass pipe to a tall vertical glass tube. The blood rose in the tube to a height of roughly eight to nine feet above the heart — and, crucially, it bobbed up and down with each heartbeat. He published the work in the second volume of his Haemastaticks (1733).
It is hard to overstate how important this crude, even disturbing, experiment was. Before Hales, the "force" of the blood was a vague, almost mystical idea. Hales proved that blood pressure is a real, physical, measurable quantity — a column of fluid pushing with a force you could read off a ruler. He had turned an abstraction into a number. (These early experiments on conscious animals would be considered unacceptable today; they are recounted here as a matter of historical record, not as an endorsement.) For his broader contributions to physiology and chemistry Hales was elected a Fellow of the Royal Society and later awarded its Copley Medal.
But Hales's method had an obvious problem: you cannot measure a person's blood pressure by opening their artery and watching blood climb a nine-foot tube. His technique was a landmark in understanding that pressure exists and can be measured, yet it was wholly impractical for living patients. For more than a century and a half afterward, the central challenge of the measurement thread would be this: how do you read the pressure inside an artery without cutting into it? That problem would not be solved until 1896.
Richard Bright and the Kidney Link (1836)
While the measurement thread stalled, the disease thread took its first great step — and it came not from blood pressure at all, but from the kidneys. The English physician Richard Bright (1789–1858), working at Guy's Hospital in London, was a meticulous observer who paired careful bedside study of his patients with equally careful examination of their bodies after death. In a series of reports culminating around 1836, Bright described a group of patients with diseased, hardened kidneys, swelling (dropsy), and albumin (protein) in the urine. This cluster became known as "Bright's disease" — for a long period a catch-all term for serious chronic kidney disease.
Bright's pivotal insight, for our story, was a connection he noticed at autopsy: many of these patients with diseased kidneys also had enlarged, thickened hearts — what we now call left ventricular hypertrophy. He recorded a hard, full, bounding pulse in such patients. Bright reasoned that something about the diseased kidney was driving the heart to enlarge. He did not have a blood-pressure instrument and did not use the word "hypertension"; what he saw and described were the consequences of sustained high pressure — a strained, overworked heart — long before that pressure could be measured in the living.
This was the first durable scientific clue that the heart, the arteries, and the kidneys are bound together in a single problem. The link Bright drew between kidney disease and an enlarged heart launched a debate that ran for the rest of the nineteenth century and well into the twentieth: which comes first, the diseased kidney or the high pressure? That "chicken-or-egg" question — the relationship between the kidney and blood pressure — remains a central and active theme in hypertension research to this day. Bright did not discover hypertension, but he was the first to glimpse the damage it does and to tie that damage to disease elsewhere in the body.
Mahomed and High Pressure as Its Own Disease
The next major figure in the disease thread is one of the most remarkable and least celebrated names in this history: Frederick Akbar Mahomed (1849–1884). A British physician of Anglo-Indian descent, Mahomed worked at Guy's Hospital (Bright's old institution) and died tragically young, of typhoid fever, at just 35. In his short career he transformed how doctors thought about high pressure. He worked with the sphygmograph — an instrument that traced the pulse wave onto smoked paper. Mahomed did not invent it, but he improved it, made it more portable and quantitative, and used it brilliantly to study the shape of the pulse as an indirect window onto arterial pressure.
Mahomed's landmark contribution was to argue that high arterial pressure could exist as a problem in its own right, in people who were otherwise apparently healthy and who did not have the protein in their urine that signaled Bright's kidney disease. In a report often dated to 1874 he described raised blood pressure in a person without evidence of kidney disease; in further work later in the 1870s he characterized otherwise-healthy individuals with persistently high pressure. He even framed a "pre-albuminuric" stage — high pressure present before any albumin appears in the urine — and his Cambridge medical thesis addressed chronic Bright's disease without albuminuria. (The precise year sometimes cited for his "first description" varies between sources, around 1874 to 1877; we note this rather than pick one falsely.)
This was a genuine conceptual breakthrough. Bright had tied a strained heart to a diseased kidney; Mahomed effectively separated high blood pressure from kidney disease, suggesting that the raised pressure itself — the increased tension in the arteries — was the primary disorder, with organ damage following. In doing so he anticipated, by decades, the modern idea of "essential" or primary hypertension: high pressure with no identifiable underlying cause. Yet there was still a fundamental limitation. The sphygmograph showed the shape of the pulse, not an actual pressure number. Doctors could infer "high tension" from a tracing, but they still could not say a patient's pressure was, for instance, 180. For that, the measurement thread had to catch up.
Riva-Rocci and the Arm Cuff (1896)
In 1896 the century-old problem Hales had left unsolved was finally cracked. The Italian physician Scipione Riva-Rocci (1863–1937) introduced the practical, cuff-based mercury sphygmomanometer — the direct ancestor of every blood-pressure device used since. His design was elegant and, for its time, almost improvised: an inflatable rubber cuff (he used bicycle inner tubing) wrapped around the upper arm, connected to a column of mercury that showed the pressure in millimetres (mmHg). The cuff was inflated until it squeezed the brachial artery shut and the pulse at the wrist vanished; the mercury reading at that moment of disappearance gave the systolic pressure — the peak pressure as the heart beats. He published it as Un nuovo sfigmomanometro in 1896.
This is the moment, more than any other, when high blood pressure could finally become a routine medical entity. For the first time, an ordinary doctor could put a real, repeatable number on a living patient's blood pressure — quickly, painlessly, and without cutting anyone open. Hales's nine-foot tube of blood had become a small mercury column on a tabletop. The famous physician William Osler adopted the device, and it spread internationally. The unit we still write today — mmHg, millimetres of mercury — is a direct inheritance from Riva-Rocci's mercury column.
One important piece, however, was still missing. The Riva-Rocci method, read by feeling for the wrist pulse, captured only the systolic (top) number. It could not reliably give the diastolic pressure — the lower pressure between beats, when the heart relaxes — which we now know matters greatly for cardiovascular risk. Capturing both numbers, the familiar "120 over 80," required one more discovery, and it came from an unexpected place: a battlefield surgeon listening through a stethoscope.
Korotkoff and the Sounds (1905)
In 1905, a Russian military surgeon named Nikolai Sergeyevich Korotkoff (1874–1920) completed the measurement that doctors still perform today. Korotkoff had served as a field surgeon in the Russo-Japanese War, where he gained deep experience listening to blood flow in damaged limbs. Working at the Imperial Military Medical Academy in St. Petersburg, he combined Riva-Rocci's cuff with a simple stethoscope placed over the artery just below the cuff — and discovered that the flow of blood through the squeezed artery makes a sequence of sounds.
His insight, reported in a famously brief note of only a few hundred words to the Academy in 1905, was precise and decisive. As the cuff is slowly deflated, the first tapping sound you hear marks the moment blood first spurts through — that is the systolic pressure. As deflation continues, the sounds change and then disappear entirely; that point of silence marks the diastolic pressure. For the first time, a clinician could obtain both the top and bottom numbers, non-invasively, with nothing more than a cuff, a mercury gauge, and a stethoscope. These pulses are still called the Korotkoff sounds, and the auscultatory (listening) method he described remains the worldwide reference standard against which automated machines are validated.
With Korotkoff's 1905 contribution, the long measurement thread that began with Hales's horse in 1733 was essentially complete. Within a span of about a decade — Riva-Rocci's cuff in 1896, Korotkoff's sounds in 1905 — blood pressure had gone from a quantity only obtainable by impaling an artery to a quick, painless, two-number bedside reading. Now that doctors could finally measure blood pressure accurately and routinely in millions of ordinary people, the remaining questions all belonged to the disease thread: what counts as "too high," why does it happen, what does it do to the body over time, and can lowering it actually help? The twentieth century would answer those questions.
"Essential Hypertension" and the Framingham Era
Once pressure could be measured in everyone, a puzzle came into focus. In most patients with persistently high readings, doctors could find no obvious cause — no diseased kidney, no tumour, nothing. The German physician Eberhard Frank is credited with coining the term "essentielle Hypertonie" (essential hypertension), generally dated to about 1911, to name exactly this category: high blood pressure that exists on its own, with no identifiable secondary cause. (Sources sometimes confuse Eberhard Frank with the physiologist Otto Frank; the term for cause-unknown high pressure is attributed to Eberhard Frank. We flag this name-confusion honestly.) Ironically, the word "essential" reflected an incorrect early belief — that the high pressure was "essential," meaning necessary, to push blood through stiffened arteries. We now know it is not necessary at all but harmful; the misleading name simply stuck. Today "essential" (or "primary") hypertension accounts for the great majority of all cases.
For the first half of the twentieth century, a dangerous complacency lingered: many physicians still believed that rising blood pressure was a normal, even useful, part of aging, not to be disturbed. (President Franklin Roosevelt's severe, essentially untreated hypertension and his death from a stroke in 1945 is the era's most famous illustration of how little could be done.) The decisive blow to that complacency came from a single town in Massachusetts. The Framingham Heart Study, which enrolled its first participants in 1948 under the U.S. Public Health Service and then the National Heart Institute, followed thousands of ordinary residents for decades, tracking who developed heart attacks and strokes and why.
Framingham's findings were revolutionary precisely because they were based on long-term, real-world data rather than opinion. The study demonstrated, clearly and statistically, that high blood pressure is a powerful, independent risk factor for heart attack, stroke, heart failure, and early death — and that the risk was real even when the elevation seemed mild. Framingham helped popularize the very phrase "risk factor" in medicine. It overturned the old idea that hypertension was a benign companion of old age and recast it as a measurable, dangerous, and — the next chapter would show — modifiable threat. But knowing high pressure is dangerous is not the same as proving that lowering it helps. That final, life-saving proof was still to come.
Proving That Treatment Works (the VA Trials)
By the 1950s and 1960s, doctors finally had drugs that could lower blood pressure. But a hard, honest question remained unanswered: did lowering the number actually save lives, or merely change a reading on a gauge? Treating millions of symptom-free people with drugs that had side effects was not justifiable on a hunch. What was needed was rigorous proof — and it arrived through one of the landmark experiments in the history of medicine: the Veterans Administration (VA) Cooperative Study on Antihypertensive Agents, largely designed and led by Dr. Edward D. Freis.
The VA trials were among the first large randomized, double-blind, placebo-controlled studies ever conducted for a cardiovascular condition — the gold-standard design in which neither patients nor doctors know who gets the real drug versus a dummy pill, removing bias. The results were so stark they could not be ignored. In the first report (1967), men with severe hypertension (diastolic 115–129 mmHg) given active treatment suffered dramatically fewer strokes, heart failures, and other catastrophes than those on placebo — the difference was so large that part of the trial had to be stopped early, because it was no longer ethical to leave the placebo group untreated. A second report (1970) extended the benefit to milder, moderate hypertension (diastolic 90–114 mmHg).
This was the proof that changed everything. For the first time it was established, beyond reasonable doubt, that treating high blood pressure prevents strokes, heart failure, and death — that the silent number on the cuff was not just a marker of risk but a target worth lowering. The VA findings, reinforced by later large trials, launched the public-health era of hypertension: nationwide screening programs, the push to find and treat the "silent" millions who felt perfectly well, and the steady decline in stroke deaths across the developed world in the decades that followed. The relay that began with a clergyman, a horse, and a glass tube had finally reached its purpose — not just measuring the pressure, and not just naming the danger, but actually saving lives.
Modern Understanding
The modern picture of hypertension is the inheritance of every milestone above, and it confirms that no single person could ever have "discovered" it — because high blood pressure turns out to be not one disease but the common end point of many overlapping causes. Today we recognize that for most people (essential or primary hypertension) the cause is multifactorial: genetics, age, body weight, dietary sodium and potassium balance, the kidneys' handling of salt and water, the renin-angiotensin-aldosterone hormone system, the stiffness of the arteries, and the nervous system all contribute. A smaller share of cases (secondary hypertension) trace to a specific identifiable cause — certain kidney, adrenal, or hormonal disorders, or some medications — the very distinction Mahomed and Frank first groped toward more than a century ago.
Two practical threads from this history are still being refined today. The first is how we measure: Riva-Rocci's cuff and Korotkoff's sounds are now mostly performed by validated automated oscillometric devices, supplemented by home monitoring and 24-hour ambulatory monitoring that capture the pressure across real life rather than in one anxious office visit. The second is what counts as too high: the exact numerical thresholds that define hypertension, and the targets we treat to, have been progressively lowered and refined as more trial evidence accumulates — an ongoing, evidence-driven conversation among major guideline bodies, not a settled or one-time decree. (For current diagnostic numbers, treatment targets, and management, see the main Hypertension article rather than this historical page.)
What ties the whole story together is a single, hopeful arc. An invisible, silent condition that for most of human history could be neither seen nor measured nor treated has become one of the most measurable, best-studied, and most effectively treatable threats to human health — and the gains have been enormous, measured in millions of strokes and heart attacks prevented. That progress belongs to no one inventor. It belongs to Hales and Bright and Mahomed and Riva-Rocci and Korotkoff and Frank, to the volunteers of Framingham and the veterans of the VA trials, and to the countless researchers and clinicians who carried the problem forward, step by patient step, until an unmeasurable mystery became a number you can check on your own arm.
Research Papers and References
The references below combine peer-reviewed historical reviews of hypertension with curated PubMed topic-search links into the primary literature on each milestone. Where a stable DOI or PubMed record is available it is linked directly; broader themes link to a PubMed topic search. Each link opens at its source (National Library of Medicine / journal publisher) in a new tab. Historical primary works (Hales's Haemastaticks, Bright's Reports of Medical Cases, Riva-Rocci's and Korotkoff's original papers) are named in the article as historical sources.
- Esunge PM. From blood pressure to hypertension: the history of research. Journal of the Royal Society of Medicine. 1991;84(10):621. — Search PubMed
- Booth J. A short history of blood pressure measurement. Proceedings of the Royal Society of Medicine. 1977;70(11):793-799. — doi:10.1177/003591577707001112
- Saklayen MG, Deshpande NV. Timeline of history of hypertension treatment. Frontiers in Cardiovascular Medicine. 2016;3:3. — doi:10.3389/fcvm.2016.00003
- Postel-Vinay N (ed.). Historical milestones in hypertension research — PubMed topic search. PubMed: history of hypertension milestones
- Stephen Hales and the first measurement of blood pressure (1733) — PubMed topic search. PubMed: Stephen Hales blood pressure history
- Cameron JS, Hicks J. Frederick Akbar Mahomed and his role in the description of hypertension at Guy's Hospital. Kidney International. 1996;49(5):1488-1506. — doi:10.1038/ki.1996.209
- Richard Bright, Bright's disease, cardiac hypertrophy and the kidney (1836) — PubMed topic search. PubMed: Richard Bright cardiac hypertrophy kidney
- Roguin A. Scipione Riva-Rocci and the men behind the mercury sphygmomanometer. International Journal of Clinical Practice. 2006;60(1):73-79. — doi:10.1111/j.1742-1241.2005.00738.x
- Paskalev D, Kircheva A, Krivoshiev S. A centenary of auscultatory blood pressure measurement: a tribute to Nikolai Korotkoff. Kidney & Blood Pressure Research. 2005;28(4):259-263. — doi:10.1159/000090084
- "Essential hypertension," Eberhard Frank, and the history of the term (c. 1911) — PubMed topic search. PubMed: essential hypertension history of the term
- Kannel WB. Blood pressure as a cardiovascular risk factor: prevention and treatment (Framingham Heart Study). JAMA. 1996;275(20):1571-1576. — doi:10.1001/jama.1996.03530440051036
- Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. The Lancet. 2014;383(9921):999-1008. — doi:10.1016/S0140-6736(13)61752-3
- Veterans Administration Cooperative Study Group on Antihypertensive Agents. Effects of treatment on morbidity in hypertension (results in diastolic 115–129 mmHg). JAMA. 1967;202(11):1028-1034. — doi:10.1001/jama.1967.03130240070013
- Veterans Administration Cooperative Study Group on Antihypertensive Agents. Effects of treatment on morbidity in hypertension, II (diastolic 90–114 mmHg). JAMA. 1970;213(7):1143-1152. — doi:10.1001/jama.1970.03170330025003
External Authoritative Resources
Connections
- Cardiology
- Hypertension (main article)
- All Conditions
- Cardiovascular Disease
- Stroke
- Magnesium
- Potassium