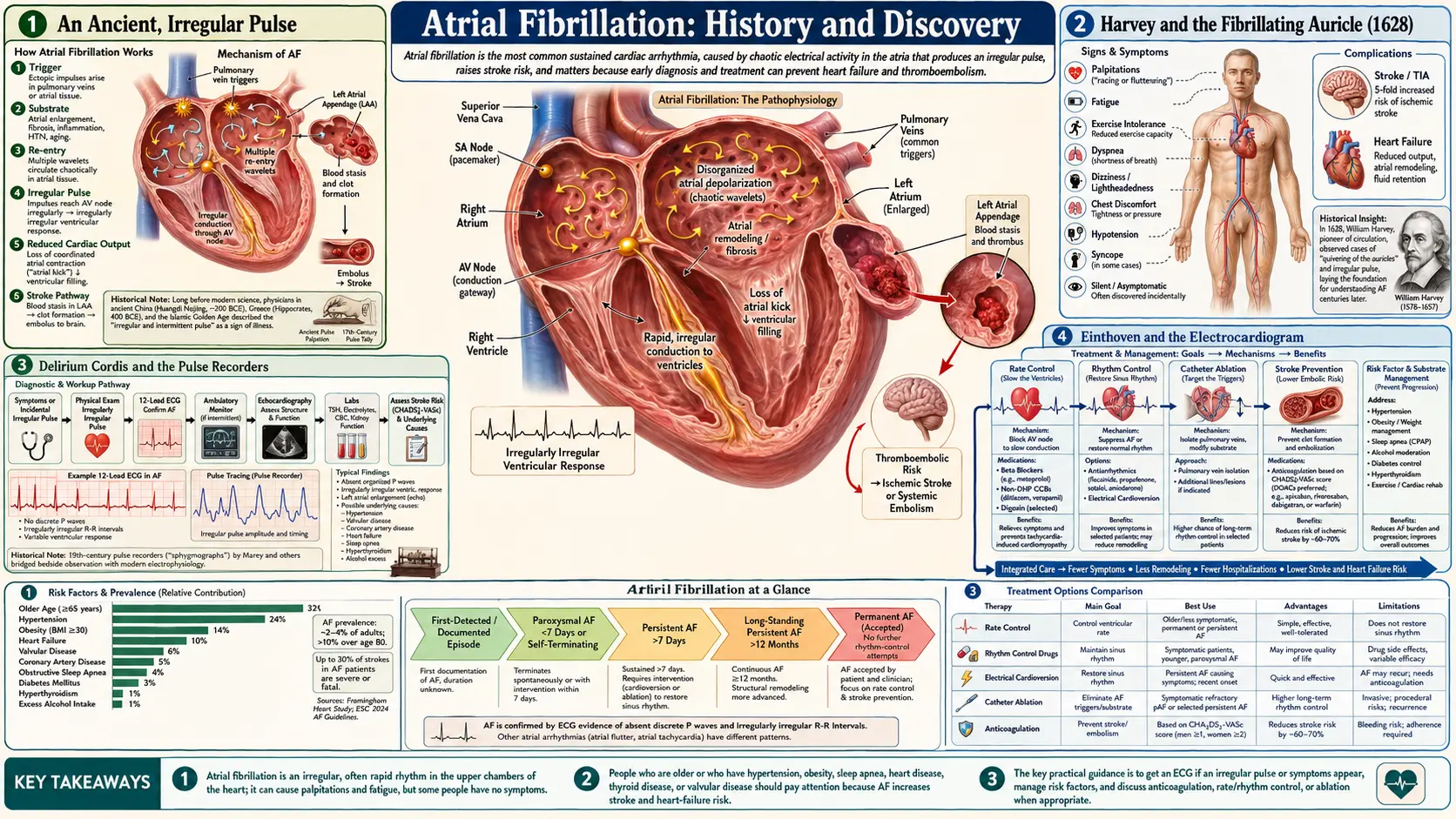
Atrial Fibrillation: History and Discovery
The story of atrial fibrillation is really two stories that took more than two thousand years to join. The first is the ancient, repeated observation that a heartbeat can be wildly, chaotically irregular — a “rebellious” or “delirious” pulse felt at the wrist by physicians in China, Greece, and Europe long before anyone knew what caused it. The second is the modern understanding of where that chaos comes from: the fibrillating upper chambers of the heart, the atria, made visible only when Willem Einthoven’s string-galvanometer electrocardiogram (1901–1903) finally let doctors see the heart’s electrical signals. Between roughly 1906 and 1910, Sir James Mackenzie, Arthur Cushny, and Sir Thomas Lewis — together with Karel Rothberger and Heinrich Winterberg in Vienna — proved that the irregular pulse and atrial fibrillation were one and the same. This page traces that long convergence, and then the century of treatment that followed: digitalis, anticoagulation, the link to stroke, and the 1998 discovery by Michel Haïssaguerre that misfiring cells in the pulmonary veins trigger the arrhythmia — the insight behind modern catheter ablation. Throughout, observation is distinguished from explanation, and where a claim is a hypothesis it is named as one.
Table of Contents
- An Ancient, Irregular Pulse
- Harvey and the Fibrillating Auricle (1628)
- Delirium Cordis and the Pulse Recorders
- Einthoven and the Electrocardiogram
- Mackenzie, Cushny, Lewis: Naming the Arrhythmia
- Competing Theories of the Mechanism
- The Stroke Link and the Age of Anticoagulation
- Pulmonary Veins and the Ablation Era (1998–)
- A Disease Concept, Two Millennia in the Making
- Research Papers and References
- Connections
- Featured Videos
An Ancient, Irregular Pulse
Long before the heart’s electrical activity could be recorded, physicians read the body by feeling the pulse, and the strange, utterly irregular pulse that we now associate with atrial fibrillation did not escape them. The pulse-diagnosis tradition of classical Chinese medicine, codified in the Huang Di Nei Jing (the Yellow Emperor’s Inner Classic, compiled over the Warring States to Han periods), is often cited as containing one of the earliest written descriptions of a chaotically irregular, “intermittent” pulse and its grim prognosis. That attribution should be read with care: the text describes irregular and weak pulses in general prognostic terms, and the precise dating of its layers is debated by historians, so it is best understood as an ancient observation of an irregular pulse rather than a description of the arrhythmia as we define it today.
Greek and later European medicine likewise recorded irregular and “disorderly” pulses, and across these traditions the message was consistent: a heartbeat with no discernible pattern was abnormal and often a sign of serious disease. What none of these observers could know was the source of the irregularity. Feeling the wrist tells you that the rhythm is chaotic; it cannot tell you whether the chaos begins in the upper chambers, the lower chambers, or the heart’s conduction system. For most of recorded history the irregular pulse was therefore a sign without a seat — a vivid, reproducible finding in search of an explanation that the tools of the day simply could not supply.
This is the central thread of the whole history. The clinical phenomenon — an irregular pulse, palpitations, breathlessness, sometimes sudden collapse — was familiar for millennia. The understanding of it, that these symptoms arise from fibrillation of the atria, is barely more than a century old. Keeping that distinction in view is what separates honest history from anachronism.
Harvey and the Fibrillating Auricle (1628)
The first step from the wrist toward the heart itself came from William Harvey. In his landmark 1628 treatise Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus (“An Anatomical Exercise on the Motion of the Heart and Blood in Living Beings”) — the work that established the circulation of the blood — Harvey also recorded a small but historically important observation. Watching the hearts of dying animals in open-chest experiments, he noticed that as the animal expired, the auricles (the atria, the heart’s upper chambers) were the last part to keep moving, and that just before death the right atrium and its appendage quivered with a feeble, ineffective, twitching motion rather than a clean contraction.
Modern cardiologists generally regard this as the first description of fibrillation of the atria in any species — Harvey was, in effect, looking directly at atrial fibrillation, even though neither he nor anyone for the next 280 years connected this dying flutter in an animal’s chest with the irregular pulse felt in living patients. It is worth being precise about what Harvey did and did not do: he observed a fibrillating auricle in animals at the point of death; he did not identify it as the cause of a clinical arrhythmia, and he had no way to record or measure it.
Harvey’s achievement here was to relocate the question. The irregular pulse was no longer purely an abstraction felt at the wrist; there was now a visible, physical event in the heart muscle that might one day be linked to it. But that link required a tool capable of recording the heart’s rhythm from outside the body — and that tool was still nearly three centuries away.
Delirium Cordis and the Pulse Recorders
Through the eighteenth and nineteenth centuries, the irregular pulse acquired evocative clinical names. Clinicians spoke of pulsus irregularis perpetuus (the perpetually irregular pulse), of “rebellious” palpitations, and — most memorably — of delirium cordis, “the delirium of the heart.” The German physician Carl Wilhelm Hermann Nothnagel is widely credited with applying the term delirium cordis to this completely irregular pulse around 1876. The eighteenth-century physician Jean-Baptiste de Sénac had already linked persistent palpitations to disease of the heart (and particularly to the mitral valve), and Robert Adams and others in the nineteenth century associated the irregular pulse with mitral stenosis. These were sharp clinical correlations, but the underlying rhythm disturbance still had no agreed mechanism.
The decisive enabling technology of this era was the device that could turn a pulse into a permanent tracing. The sphygmograph, refined by Étienne-Jules Marey in the 1860s, drew the arterial pulse as an ink line on paper. Building on this, the Scottish general practitioner James Mackenzie (later Sir James Mackenzie), working in Burnley, England, developed an ink-writing polygraph that recorded the arterial pulse and the jugular venous pulse simultaneously. This dual recording was crucial: the jugular venous tracing reflects events in the right atrium, so it offered an indirect window onto what the atria were doing. Mackenzie made the key observation that in patients whose rhythm became irregular, the venous “a” wave — the deflection produced by atrial contraction — disappeared. The atria, he reasoned, had stopped contributing an effective coordinated beat.
Mackenzie initially interpreted this as a relatively benign loss of atrial activity and used terms such as “nodal rhythm” to describe it. The interpretation was incomplete, but the recording was not: he had captured, on paper, the mechanical signature of the failing atrium. The stage was now set for a tool that could record not the pulse, but the heart’s electricity directly.
Einthoven and the Electrocardiogram
The breakthrough that turned the irregular pulse from a mystery into a diagnosis was the electrocardiogram. The Dutch physiologist Willem Einthoven (1860–1927), working at the University of Leiden, invented the string galvanometer, an instrument sensitive enough to record the tiny electrical currents generated by the beating heart. Einthoven published a preliminary report of the instrument in 1901 and a fuller description, with electrocardiographic tracings, in 1903; by 1905 the first clinical recordings were being transmitted by cable from the hospital to his laboratory. For developing the technique he was awarded the Nobel Prize in Physiology or Medicine in 1924. The letters he assigned to the waves of the tracing — P, Q, R, S, T — are still used by every cardiologist and nurse today.
The significance for atrial fibrillation was immediate and profound. For the first time, the activity of the atria and the ventricles could be seen separately, as distinct electrical events, on a single record. A normal tracing shows an orderly P wave (atrial activation) before each QRS complex (ventricular activation). In atrial fibrillation the organized P waves vanish, replaced by a rapid, irregular, undulating baseline, while the QRS complexes march out at irregular intervals. Einthoven himself published an electrocardiogram showing this picture — what we now recognize as atrial fibrillation — in 1906, illustrating the “irregular” tracing among the abnormal rhythms his new instrument could capture.
It is important to credit this accurately: Einthoven’s gift was the instrument and the demonstration that the heart’s electrical signals could be recorded and classified. The work of proving that this particular irregular tracing was the centuries-old delirium cordis — that the chaotic baseline meant the atria were fibrillating, and that this explained the irregular pulse — was carried out by the clinicians who put the string galvanometer to work at the bedside.
Mackenzie, Cushny, Lewis: Naming the Arrhythmia
The crucial hypothesis — that delirium cordis was caused by fibrillation of the atria — came from the pharmacologist Arthur Robertson Cushny. Studying the hearts of dogs, Cushny was struck by the close resemblance between experimentally induced auricular fibrillation in the animal and the extreme, perpetual irregularity seen clinically as delirium cordis in patients. In 1906, with his colleague Charles Edmunds, he published a careful case report of a woman whose pulse tracings exactly paralleled those of dogs in atrial fibrillation, concluding that the irregularity arose from disordered activity of the atrium rather than a defect in the ventricle. This is generally regarded as the first clinical proposal that what would later be called atrial fibrillation underlay the irregular human pulse — but at this stage it remained a well-argued hypothesis, built on mechanical pulse tracings, not yet confirmed by electrocardiography.
That confirmation came within a few years, and it came from several hands at once. In 1909, the English physician Thomas Lewis (later Sir Thomas Lewis), working with Einthoven’s string galvanometer, and — independently — Karel Frederik Rothberger and Heinrich Winterberg in Vienna, demonstrated electrocardiographically that the clinical condition of pulsus irregularis perpetuus / delirium cordis was indeed atrial (then “auricular”) fibrillation. Lewis recorded electrocardiograms in patients and in animals and matched the fibrillatory waves to the irregular pulse, and over 1909–1910 he is credited with firmly establishing, on the electrocardiogram, that the irregular pulse and atrial fibrillation were the same entity. James Mackenzie’s earlier polygraph observations — the lost “a” wave — were now explained: the atria were not beating coordinately because they were fibrillating.
Within roughly four years, then, a centuries-old clinical sign had been given a definitive mechanism. Cushny supplied the hypothesis from animal physiology (1906); Lewis, with Rothberger and Winterberg, supplied the electrocardiographic proof (1909–1910); and Mackenzie’s recordings provided the bridge from the bedside pulse to the failing atrium. The convergence of these workers around 1909 is rightly seen as the moment atrial fibrillation became a defined disease rather than a puzzling symptom.
Competing Theories of the Mechanism
Identifying that the atria fibrillate did not, by itself, explain why the muscle behaves so chaotically, and through the twentieth century rival theories competed. One influential idea, associated with the experimental work of George Ralph Mines and Walter Garrey in the 1910s and developed further by later investigators, held that fibrillation is sustained by re-entry — waves of electrical activation circling continuously through the atrial tissue rather than dying out. A related refinement, the “multiple wavelet” hypothesis articulated by Gordon Moe in the late 1950s and early 1960s, proposed that fibrillation consists of many small, wandering wavelets of activation coexisting and constantly reforming across the atria. A competing view emphasized rapidly firing ectopic foci — localized patches of tissue discharging at very high rates.
These were genuine scientific hypotheses, debated for decades, and for much of that time the evidence did not decisively favor one over another; elements of each turned out to matter. The honest historical summary is that, until the very end of the century, atrial fibrillation was understood to be a self-sustaining electrical disorder of the atria whose precise drivers remained contested. That uncertainty had a practical consequence: with no agreed trigger to target, treatment was aimed at the consequences of the arrhythmia — slowing the racing ventricle and, later, preventing the clots it caused — rather than at curing it.
The oldest specific therapy belongs here. Digitalis, the foxglove-derived remedy described by the English physician William Withering in his 1785 An Account of the Foxglove, was used for “dropsy” (the swelling of heart failure) long before anyone understood rhythm; in the twentieth century it found a rational place in atrial fibrillation because it slows conduction through the atrioventricular node and thereby calms a dangerously fast ventricular rate. It is a striking example of an empirical folk-derived drug acquiring, a century and a half later, a mechanistic justification.
The Stroke Link and the Age of Anticoagulation
The most consequential modern insight about atrial fibrillation is not how to stop it but how dangerous it is when left alone: it markedly raises the risk of stroke. When the atria fibrillate instead of contracting, blood stagnates — especially in a pouch off the left atrium called the left atrial appendage — and stagnant blood clots. A fragment of that clot can travel to the brain and cause an ischemic stroke. Atrial fibrillation is now recognized as one of the leading causes of stroke, and these strokes tend to be larger and more disabling than average. (The mechanism, prevention, and treatment of these strokes are covered in depth on the dedicated Stroke page.)
The remedy was an anticoagulant. Warfarin traces to the work of Karl Paul Link’s laboratory at the University of Wisconsin in the 1940s, which isolated the anticoagulant compound responsible for a cattle-bleeding disease caused by spoiled sweet clover; the drug entered clinical use in the 1950s. For decades, however, there was no rigorous proof that giving warfarin to patients with atrial fibrillation actually prevented strokes — it was plausible but unproven, and the drug’s bleeding risk made the question urgent. That proof arrived in the late 1980s and early 1990s through a cluster of randomized controlled trials — among them AFASAK (Denmark, 1989) and the Stroke Prevention in Atrial Fibrillation (SPAF) studies — which together showed that adjusted-dose warfarin reduced strokes in non-valvular atrial fibrillation by roughly two-thirds. This was a turning point: prevention of the arrhythmia’s deadliest complication was now evidence-based.
Two later developments refined this further. Risk-scoring schemes — the CHADS₂ score (2001) and its successor CHA₂DS₂-VASc (2010) — were devised to estimate an individual patient’s stroke risk and so to decide who genuinely benefits from anticoagulation. And in the 2010s the direct oral anticoagulants (DOACs, such as dabigatran, rivaroxaban, apixaban, and edoxaban) were shown in large trials to work at least as well as warfarin with a lower risk of the most feared bleeding and without the need for routine blood-level monitoring, largely displacing warfarin as first-line therapy for most patients. The throughline of this section is that the great therapeutic advance against atrial fibrillation was, for many years, not curing it but defusing it.
Pulmonary Veins and the Ablation Era (1998–)
The possibility of curing atrial fibrillation, rather than merely controlling its rate and consequences, opened in 1998. The French cardiac electrophysiologist Michel Haïssaguerre and his colleagues in Bordeaux published a landmark study in the New England Journal of Medicine reporting that, in many patients, the arrhythmia is repeatedly triggered by bursts of rapid electrical activity arising from a specific and unexpected location: the muscular sleeves surrounding the pulmonary veins, the vessels that return oxygenated blood from the lungs to the left atrium. Ectopic beats firing from inside these veins were shown to initiate atrial fibrillation — and crucially, ablating (destroying) those firing sites could abolish the arrhythmia in some patients.
This finding reframed atrial fibrillation. Where the disorder had been seen mainly as a diffuse, self-sustaining electrical storm across the whole atrium, Haïssaguerre’s work identified discrete, treatable triggers. It became the foundation of pulmonary vein isolation (PVI): a catheter-based procedure in which thin wires are threaded through a vein into the heart and used to create rings of scar around the pulmonary veins, electrically walling off the trigger sites so their misfiring can no longer reach and ignite the atrium. PVI, originally delivered with radiofrequency heat and later also with cryoablation (freezing) and, more recently, pulsed-field ablation, is now the cornerstone of catheter treatment for atrial fibrillation and one of the most commonly performed cardiac electrophysiology procedures in the world.
The ablation era did not erase what came before; rate control with drugs such as digitalis and beta-blockers, rhythm control with antiarrhythmic medication, electrical cardioversion, and above all anticoagulation to prevent stroke all remain central. But it added something genuinely new — a mechanism-targeted, potentially curative intervention — and it did so by answering, at last, the question Harvey’s fibrillating auricle and the ancient irregular pulse had always posed: not just that the atria misbehave, but where the misbehavior begins.
A Disease Concept, Two Millennia in the Making
Few common diseases have a history that so cleanly separates observation from understanding. The irregular pulse was felt and feared for at least two thousand years; the named clinical entity of delirium cordis is a few centuries old; the proof that it is atrial fibrillation is barely more than a hundred years old; and the discovery of how to trigger, prevent, and even cure it belongs almost entirely to the last few decades. The arc runs from the fingertips on the wrist, to Marey’s and Mackenzie’s ink tracings, to Einthoven’s string galvanometer, to a catheter inside the left atrium.
The lesson embedded in this history is one of intellectual humility. For most of the past, skilled physicians could describe atrial fibrillation precisely and could not explain it at all — and several of the confident explanations they did offer (paralysis of the auricle, a purely ventricular fault, a benign “nodal” rhythm) were wrong. Progress came not from cleverer guessing but from better instruments: the device that recorded the venous pulse, the device that recorded the heart’s electricity, the catheter that could reach inside the chamber itself. Each new tool turned a hypothesis into a measurement.
That same trajectory now continues. Today’s research into the genetics of atrial fibrillation, into atrial scarring and remodeling, into wearable and implantable monitors that catch the arrhythmia before it causes a stroke, and into ever more precise ablation is the direct descendant of a question first raised at a patient’s wrist in antiquity. For the practical, present-day picture — symptoms, diagnosis, rate and rhythm control, anticoagulation, and ablation as they are used now — see the main Atrial Fibrillation article.
Research Papers and References
The references below combine landmark peer-reviewed papers with curated historical reviews and PubMed topic-search links into the history and discovery of atrial fibrillation. Historical primary texts — the Huang Di Nei Jing, Harvey’s De Motu Cordis (1628), and Withering’s Account of the Foxglove (1785) — are named in the article as historical sources rather than as modern citations. Links open at the publisher, DOI, or PubMed (National Library of Medicine) in a new tab.
- Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. New England Journal of Medicine. 1998;339(10):659–666. — doi:10.1056/NEJM199809033391003
- Flegel KM. From delirium cordis to atrial fibrillation: historical development of a disease concept. Annals of Internal Medicine. 1995;122(11):867–873. — doi:10.7326/0003-4819-122-11-199506010-00010
- Silverman ME. From rebellious palpitations to the discovery of auricular fibrillation: contributions of Mackenzie, Lewis and Einthoven. American Journal of Cardiology. 1994;73(5):384–389. — doi:10.1016/0002-9149(94)90013-2
- Fye WB. Tracing atrial fibrillation — 100 years. New England Journal of Medicine. 2006;355(14):1412–1414. — doi:10.1056/NEJMp068169
- McMichael J. History of atrial fibrillation 1628–1819: Harvey – de Senac – Laënnec. British Heart Journal. 1982;48(3):193–197. — doi:10.1136/hrt.48.3.193
- Stroke Prevention in Atrial Fibrillation Study (SPAF). Final results. Circulation. 1991;84(2):527–539. — doi:10.1161/01.CIR.84.2.527
- One hundred years of atrial fibrillation (historical review). Indian Pacing and Electrophysiology Journal / PMC. — PMC: One hundred years of atrial fibrillation
- History of atrial fibrillation (comprehensive historical review). PMC. — PMC: History of Atrial Fibrillation
- Einthoven W and the string galvanometer / first electrocardiograph (centennial reviews) — PubMed: Einthoven string galvanometer history
- Cushny AR — auricular fibrillation and delirium cordis (historical) — PubMed: Cushny auricular fibrillation history
- Thomas Lewis and the electrocardiographic identification of auricular fibrillation — PubMed: Thomas Lewis auricular fibrillation 1909
- Multiple-wavelet and re-entry hypotheses of atrial fibrillation (Moe; Mines; Garrey) — PubMed: atrial fibrillation wavelet and re-entry mechanisms
- Warfarin and anticoagulation for stroke prevention in atrial fibrillation (AFASAK, SPAF, meta-analyses) — PubMed: warfarin atrial fibrillation stroke prevention
- Pulmonary vein isolation and catheter ablation for atrial fibrillation — PubMed: pulmonary vein isolation catheter ablation
External Authoritative Resources
- NHLBI (National Heart, Lung, and Blood Institute) — Atrial Fibrillation
- American Heart Association journals — Atrial Fibrillation
- PubMed — Atrial fibrillation history and discovery
Connections
- Cardiology
- Atrial Fibrillation (main article)
- Arrhythmia
- Stroke
- Heart Failure
- Cardiomyopathy
- Hypertension
- All Conditions