Aortic Dissection
Aortic dissection is one of medicine's most dramatic emergencies — a catastrophic tear in the inner lining of the aorta that allows blood to surge into the aortic wall itself, splitting it apart. Without rapid recognition and treatment, it is frequently fatal within hours. Yet many patients survive and go on to live full lives with proper ongoing care. Understanding this condition — how it develops, how it presents, and how it is treated — can literally save your life or the life of someone near you.
Table of Contents
- What Is Aortic Dissection?
- Classification: Stanford and DeBakey Systems
- Who Is at Risk? Epidemiology and Risk Factors
- How It Feels: Symptoms and Clinical Presentation
- Diagnosis: Imaging and Laboratory Workup
- Treatment: Type A Emergency Surgery and Type B Medical Management
- Complications and Prognosis
- Living After Aortic Dissection: Long-Term Management
- Research Papers
- Featured Videos
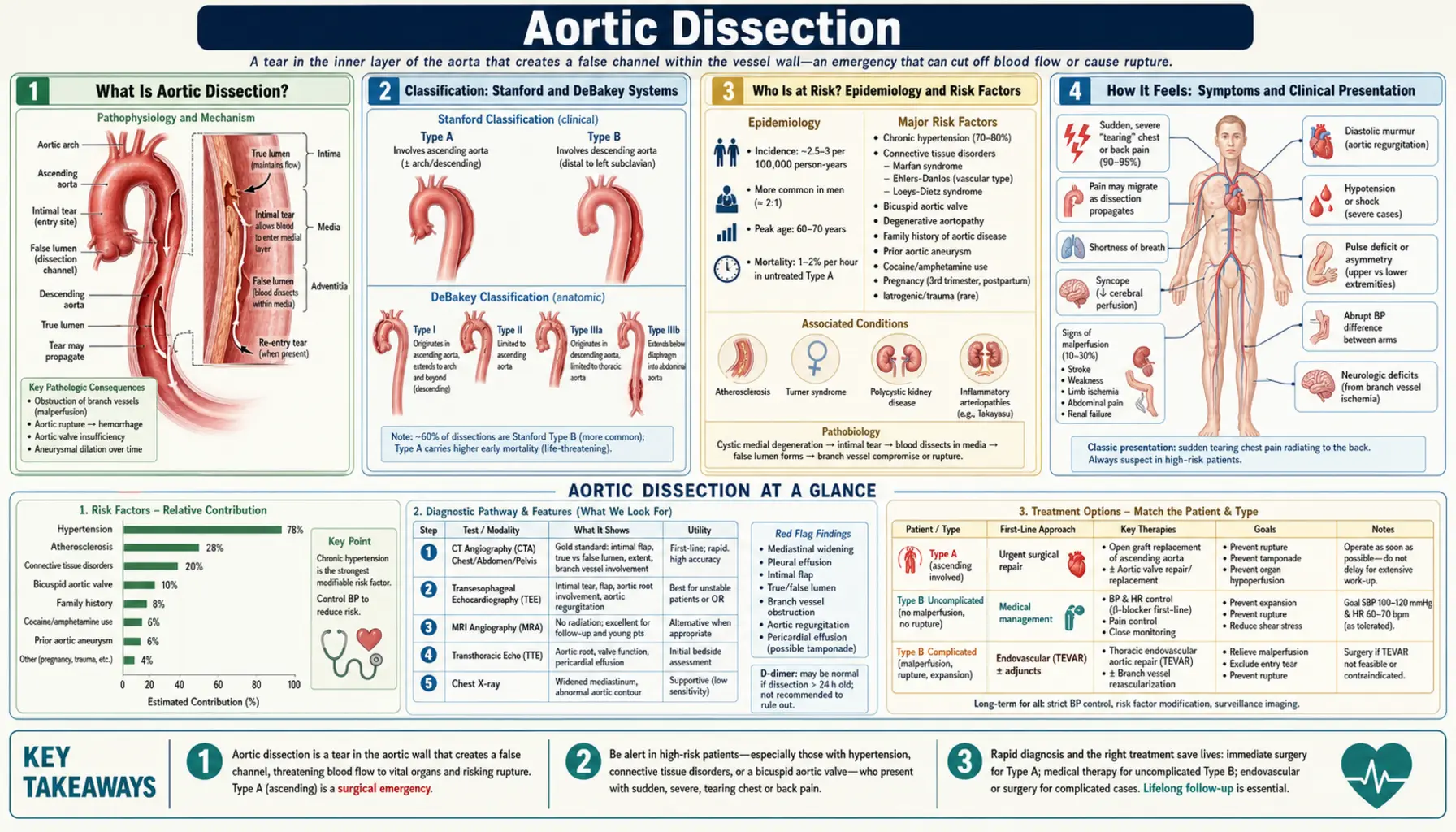
What Is Aortic Dissection?
The aorta is the body's largest artery — a thick-walled tube roughly the diameter of a garden hose that carries oxygenated blood from the heart to every organ and limb. Its wall has three layers: an inner intima, a middle media (the muscular, elastic layer that gives the aorta its strength), and an outer adventitia.
In an aortic dissection, a tear develops in the intima. High-pressure arterial blood then forces its way into the media, separating the layers and carving out a second channel — the false lumen — running parallel to the true lumen. This false lumen can propagate rapidly along the length of the aorta in either direction, obstructing branch arteries as it travels.
The underlying tissue defect is called cystic medial degeneration: the smooth muscle cells of the media die off, the elastic fibers fragment, and a ground-glass substance (ground substance) accumulates in the gaps. This leaves the aortic wall mechanically weakened and vulnerable to splitting under the relentless pulsatile stress of the heartbeat.
Aortic dissection belongs to a group of related emergencies called acute aortic syndrome, which also includes intramural hematoma (bleeding within the wall without an intimal tear) and penetrating aortic ulcer (an atherosclerotic plaque that erodes through the intima). All three carry similar urgency.
The condition earns its nickname "The Great Masquerader" because its symptoms can mimic heart attack, stroke, pulmonary embolism, and many other conditions. This diagnostic challenge makes awareness critically important: any sudden, severe, tearing chest or back pain — especially if it is maximal at the very moment of onset — demands immediate emergency evaluation.
Back to Table of ContentsClassification: Stanford and DeBakey Systems
Cardiologists and cardiac surgeons use two overlapping classification systems to describe where the dissection involves the aorta. The distinction matters enormously because it determines treatment — emergency surgery versus initial medical management.
Stanford Classification (the system used in everyday clinical practice)
Stanford Type A involves the ascending aorta — the portion of the aorta that rises from the heart, regardless of where the initial tear actually originated. If the ascending aorta is involved in any way, the dissection is Type A. This is the most dangerous form. Blood flowing into the false lumen can:
- Compress the coronary arteries, causing heart attack
- Rupture backward into the pericardial sac, causing cardiac tamponade
- Destroy the aortic valve, causing acute severe aortic regurgitation
- Propagate into the carotid arteries, causing stroke
Type A dissection is a surgical emergency. Without immediate operative repair, mortality rises at approximately 1–2% per hour in the first 24–48 hours. The goal is to get the patient to the operating room within hours of diagnosis.
Stanford Type B involves only the descending thoracic aorta — the portion that curves downward past the left subclavian artery. The ascending aorta is not affected. Uncomplicated Type B dissection is initially managed with aggressive blood pressure control rather than surgery, though certain high-risk situations require endovascular or open surgical intervention.
DeBakey Classification (anatomically more precise)
- DeBakey Type I: Tear in the ascending aorta; dissection extends through the arch and into the descending aorta. (Corresponds to Stanford A, extensive.)
- DeBakey Type II: Tear confined to the ascending aorta only, not extending beyond the arch. (Corresponds to Stanford A, limited.)
- DeBakey Type III: Tear originates in the descending aorta distal to the left subclavian artery. (Corresponds to Stanford B.)
In practice, most hospitals and guidelines use the Stanford system because the single decisive question — "Is the ascending aorta involved?" — determines the immediate management pathway.
Back to Table of ContentsWho Is at Risk? Epidemiology and Risk Factors
Aortic dissection affects approximately 3 people per 100,000 per year in the United States, with roughly 10,000–15,000 cases annually. Men are affected about twice as often as women. The peak incidence occurs between ages 60 and 70 years, though certain underlying conditions cause dissection at much younger ages.
Hypertension — The Most Important Risk Factor
Chronically elevated blood pressure is present in 70–80% of all aortic dissection patients. Sustained hypertension batters the aortic wall with relentless pulsatile stress, driving cystic medial degeneration over decades. Even blood pressure that is merely "borderline high" over many years significantly increases risk. This is why lifelong aggressive blood pressure control is the most important preventive measure — and the cornerstone of long-term post-dissection management.
Bicuspid Aortic Valve
The aortic valve normally has three leaflets. About 1–2% of the population is born with only two (bicuspid), and this congenital abnormality is associated with inherent weakness of the ascending aortic wall — cystic medial necrosis develops independently of blood pressure. Bicuspid aortic valve accounts for 5–10% of dissections and typically presents a decade or two earlier than hypertensive dissection, with patients in their 40s and 50s.
Connective Tissue Disorders
- Marfan syndrome (FBN1 gene; fibrillin-1 protein abnormality): Fibrillin is a scaffolding protein that gives elastic tissue its structural integrity. Without it, the aortic wall dilates and dissects, often at relatively small aortic diameters. Dissection can occur in patients as young as their 20s and 30s.
- Loeys-Dietz syndrome (TGFBR1 or TGFBR2 gene mutations): An aggressive aortopathy that dissects at even smaller aortic diameters than Marfan syndrome. Requires earlier prophylactic repair thresholds.
- Vascular Ehlers-Danlos syndrome (COL3A1 gene; type III collagen deficiency): Primarily affects medium-sized arteries with a predisposition to spontaneous rupture rather than dissection, but can involve the aorta.
Other Important Risk Factors
- Cocaine and methamphetamine use: These stimulants cause acute, dramatic surges in blood pressure that can trigger dissection in otherwise normal aortas — an important cause in younger patients.
- Pregnancy: The third trimester and peripartum period carry elevated dissection risk, driven by hormonal changes that soften medial connective tissue combined with the marked increase in cardiac output during pregnancy.
- Prior aortic surgery or instrumentation: Existing surgical suture lines and instrumented aortic segments are vulnerable to dissection.
- Aortic aneurysm: A dilated aorta already has medial degeneration; the risk of dissection rises with increasing aortic diameter.
- Family history: A first-degree relative with aortic dissection or aneurysm significantly elevates personal risk.
- Turner syndrome (45,X karyotype): Associated with bicuspid aortic valve and aortic coarctation, both of which promote aortopathy.
How It Feels: Symptoms and Clinical Presentation
Aortic dissection earns its reputation as "The Great Masquerader" because it mimics so many other conditions. Knowing what it truly feels like — and how it differs from, say, a heart attack — can be the difference between life and death.
The Cardinal Symptom: Sudden Tearing Pain
The hallmark of aortic dissection is sudden, severe pain that is maximal at the very moment it begins — unlike angina or heart attack pain, which typically builds gradually. Patients often describe it as "the worst pain of my life," with a tearing, ripping, or stabbing quality that feels as though something is being violently split apart inside the chest.
- Type A dissection: Pain is typically in the anterior chest or substernal region.
- Type B dissection: Pain classically radiates to the interscapular back (between the shoulder blades).
- Migrating pain: As the dissection propagates along the aorta, the pain moves — a classic and diagnostically important feature that distinguishes it from most other causes of chest pain.
Pulse Deficit and Blood Pressure Asymmetry
When the dissection extends into the brachiocephalic or subclavian arteries, it can compress or occlude flow to one arm. A blood pressure difference greater than 20 mmHg between the two arms — or a pulse that is absent or weaker on one side — is a highly specific finding that should immediately raise suspicion for dissection.
Aortic Regurgitation
In Stanford Type A dissection, the false lumen can undermine the structural supports of the aortic valve, causing it to become incompetent. Acute severe aortic regurgitation develops in 50–70% of Type A cases, producing a decrescendo diastolic murmur audible at the left sternal border. When severe, this floods the left ventricle with blood it cannot accommodate, causing acute pulmonary edema with flash-onset breathlessness.
Cardiac Tamponade
The false lumen can rupture backward through the adventitia into the pericardial sac, filling it with blood. This is hemopericardium leading to cardiac tamponade — the external pressure of blood in the pericardium squeezes the heart so it cannot fill. Beck's triad (hypotension + distended neck veins + muffled heart sounds) and pulsus paradoxus (blood pressure drops more than 10 mmHg with inspiration) are the classic signs. This complication carries very high mortality.
Syncope
Approximately 10% of patients lose consciousness at or near the time of pain onset. The mechanism may be vasovagal (pain-triggered), cardiac tamponade, or sudden hypotension from aortic rupture. Syncope with chest pain is a particularly alarming combination.
Neurological Complications
- Stroke: Extension of dissection into the carotid arteries causes cerebral ischemia — hemiplegia, aphasia, facial droop.
- Spinal cord ischemia: Occlusion of intercostal arteries (which feed the anterior spinal artery) can cause sudden paraplegia or paraparesis, particularly in Type B dissection.
- Horner syndrome: Compression of the stellate ganglion by the expanding false lumen causes ptosis (drooping eyelid), miosis (small pupil), and anhidrosis on one side of the face.
- Hoarse voice: Compression of the recurrent laryngeal nerve as it loops under the aortic arch.
Visceral Ischemia
When the false lumen extends into abdominal branch arteries, catastrophic organ ischemia follows:
- Mesenteric ischemia: Occlusion of the superior mesenteric artery (SMA) causes severe abdominal pain and bowel ischemia. This is the most feared abdominal complication — bowel necrosis carries extremely high mortality and demands emergent surgical or endovascular intervention.
- Renal failure: Bilateral renal artery involvement causes oliguria and acute kidney injury.
- Limb ischemia: Iliac or femoral artery occlusion causes a cold, pulseless, painful leg.
Diagnosis: Imaging and Laboratory Workup
Rapid, accurate diagnosis is essential — every minute counts in Type A dissection. The workup begins with a high index of clinical suspicion followed by targeted imaging.
CT Angiography of the Aorta — The Definitive First-Line Test
ECG-gated CT angiography of the chest, abdomen, and pelvis is the definitive diagnostic test for aortic dissection in stable patients. It is fast, widely available, and provides a complete roadmap of the dissection. Key findings include:
- Double lumen with intimal flap: The pathognomonic finding — two distinct channels separated by a thin curving flap of intima. Seeing this on CT is diagnostic.
- True vs. false lumen distinction: The false lumen is typically larger, may contain thrombus, shows "cobweb" artifacts from strands of incomplete media, and has an outer convex wall. The true lumen is the smaller, more circular channel.
- Entry tear location: Where the intima first tore, and any re-entry tears.
- Branch vessel involvement: Whether coronary ostia, carotid, mesenteric, renal, or iliac arteries are affected by the false lumen.
- Aortic diameter: At multiple levels to plan surgical or endovascular repair.
- Pericardial effusion: Suggesting hemopericardium and impending tamponade.
Chest X-Ray
A chest X-ray is obtained rapidly in the emergency room but is neither sensitive nor specific. Suspicious findings include a widened mediastinum (greater than 8 cm), the "calcium sign" (aortic calcification displaced more than 10 mm inward from the outer aortic wall), and left pleural effusion (hemothorax from aortic leakage). Critically: a normal chest X-ray does not exclude aortic dissection — up to 20% of dissections have a normal CXR.
Transesophageal Echocardiography (TEE)
TEE provides exceptional sensitivity (98%) for Type A dissection and can be performed at the bedside in hemodynamically unstable patients who cannot safely go to the CT scanner. The probe is positioned in the esophagus (which runs directly behind the aorta), giving near-perfect visualization of the ascending and descending aorta, the intimal flap, aortic valve function, and pericardial effusion. TEE is the preferred tool for evaluation in the operating room immediately before surgery.
MRI
MRI provides superb anatomical detail without radiation and is the preferred modality for long-term follow-up imaging. However, the scan takes 30–60 minutes, making it impractical in the acute emergency setting. It is used primarily for surveillance imaging after the acute phase.
D-Dimer
A D-dimer level below 500 ng/mL measured within 24 hours of symptom onset effectively rules out acute aortic syndrome in patients with a low pre-test probability — this is the basis of the ADD-RS (Aortic Dissection Detection Risk Score) decision rule. D-dimer is most useful when the clinical probability is low and CT is being considered; in high-probability cases, CT should not wait for D-dimer results.
ECG
An ECG is obtained to evaluate for concurrent myocardial infarction (which can occur when the dissection extends into the coronary ostia) and to exclude other causes of chest pain. The ECG may be entirely normal in aortic dissection, which itself is diagnostically informative — severe chest pain with a normal ECG raises the probability of dissection over STEMI.
Back to Table of ContentsTreatment: Type A Emergency Surgery and Type B Medical Management
The single most important decision in managing aortic dissection is: Type A or Type B? The answer determines an entirely different management pathway.
Type A Dissection — Immediate Surgical Emergency
Stanford Type A dissection demands immediate transfer to the operating room. Before and during transport, the priority is blood pressure control to slow the dissection's progression:
- Target: Systolic blood pressure 100–120 mmHg and heart rate below 60 beats per minute
- Anti-impulse therapy: The treatment goal is to reduce both blood pressure AND the rate of pressure rise with each heartbeat (dP/dt). IV beta-blockers (labetalol, esmolol) achieve both. Caution: Isolated vasodilators (nitroprusside alone) without beta-blockade cause reflex tachycardia that increases dP/dt and can paradoxically accelerate dissection propagation.
- Pain control: IV opioids reduce sympathetic drive and lower blood pressure
Surgery involves open replacement of the ascending aorta with a synthetic graft. Depending on involvement of the aortic arch or valve, the procedure may also include:
- Aortic valve repair or replacement
- Coronary artery reimplantation (if ostia are involved)
- Hemi-arch or total arch replacement with hypothermic circulatory arrest (HCA) — the patient's body temperature is cooled to 18–20°C and the heart-lung machine is temporarily stopped to allow surgery on the arch without blood flow
At experienced aortic centers, 30-day surgical mortality is 10–15%. Without surgery, mortality at 48 hours approaches 50%.
Type B Dissection — Anti-Impulse Medical Therapy
Uncomplicated Type B dissection (no malperfusion, no rapidly expanding false lumen, no refractory pain) is initially managed with intensive medical therapy:
- IV labetalol (first choice — combined alpha and beta blockade) or IV esmolol (titratable, short-acting beta-blocker) to achieve SBP <120 mmHg and HR <60 bpm
- IV nitroprusside added if targets not reached with beta-blockade alone
- Transition to oral therapy (metoprolol + amlodipine + ACE inhibitor or ARB) once stable
- Target lifelong BP <130/80 mmHg
Complicated Type B dissection — defined by any of the following: branch artery malperfusion (mesenteric, renal, or limb ischemia), refractory or recurrent pain, rapidly expanding false lumen, or aortic diameter ≥5.5 cm — requires intervention:
- TEVAR (Thoracic Endovascular Aortic Repair): A catheter-delivered stent graft is deployed in the descending thoracic aorta, covering the entry tear. This redirects blood from the false lumen back into the true lumen, decompressing the false lumen and reversing malperfusion of branch vessels. TEVAR has largely replaced open surgery for complicated Type B dissection because it avoids the physiological stress of a major open thoracic operation.
- The INSTEAD-XL trial (PMID 24126856) demonstrated that TEVAR plus medical therapy led to significantly improved aorta-related survival and reduced disease progression in uncomplicated Type B dissection at 5-year follow-up compared with medical therapy alone — shifting practice toward earlier endovascular treatment in select patients.
Complications and Prognosis
Even when the acute phase is survived, aortic dissection carries ongoing risks that require lifelong vigilance.
Acute Complications
- Aortic rupture: The most feared complication — the outer aortic wall (adventitia) tears completely, causing catastrophic hemorrhage into the chest, pericardium, or abdomen. Usually fatal within minutes without immediate surgical intervention.
- Cardiac tamponade: Hemopericardium from dissection into the pericardial sac compresses the heart (see Symptoms section).
- Myocardial infarction: Extension into the coronary ostia — right more commonly than left — causes acute STEMI. This creates a diagnostic and therapeutic dilemma: thrombolytics given for presumed STEMI can be catastrophic if the true diagnosis is dissection.
- Stroke: Carotid artery involvement causes ischemic stroke in 5–10% of Type A cases.
- Paraplegia: Spinal cord ischemia from intercostal artery occlusion; more common in Type B and after TEVAR (spinal drain placement reduces this risk).
- Acute mesenteric ischemia: The most ominous abdominal complication — bowel necrosis carries 50–80% mortality even with emergency surgery.
Late Complications
- False lumen expansion and aneurysm formation: The false lumen, if it remains patent (open), gradually enlarges over months to years. A false lumen diameter exceeding 5.5 cm is a threshold for elective repair. Serial aortic imaging is essential.
- Aortic regurgitation progression after Type A repair
- Re-dissection: The remaining native aorta is still abnormal and subject to new tears
- Endoleak after TEVAR: Persistent flow into the false lumen despite the stent graft
Prognosis
With modern surgical and endovascular care:
- Type A: In-hospital mortality 10–15% at experienced centers (vs. ~50% without surgery); 5-year survival approximately 60–70%
- Type B uncomplicated: In-hospital mortality under 10% with medical management; 5-year survival approximately 60–80%
- The most important determinants of long-term survival are blood pressure control, smoking cessation, and adherence to surveillance imaging
Living After Aortic Dissection: Long-Term Management
Surviving an aortic dissection is only the beginning. The underlying aortic vulnerability — whether from hypertension, a connective tissue disorder, or both — persists. Long-term management is intensive and requires a disciplined partnership between patient and physician.
Blood Pressure Control — Non-Negotiable
The target is SBP <130 mmHg (ideally <120 mmHg) at all times. Beta-blockers are the cornerstone medication: they reduce both blood pressure and the force and rate of each heartbeat. Common regimens include:
- Metoprolol succinate or carvedilol (beta-blockade)
- Amlodipine (calcium channel blocker — excellent aortic vasodilation)
- ACE inhibitor or ARB (for connective tissue disorder patients, ARBs such as losartan have additional benefit by blocking TGF-beta signaling in the aortic wall)
Blood pressure must be checked at home daily and at every medical visit. Uncontrolled blood pressure is the leading cause of late false lumen expansion and re-dissection.
Surveillance Imaging — A Lifelong Commitment
Serial imaging of the entire aorta is essential to detect false lumen expansion before it becomes life-threatening. The typical schedule:
- CT or MRI at 1 month post-discharge
- CT or MRI at 3 months
- CT or MRI at 6 months
- Annual CT or MRI thereafter for life
MRI is preferred for younger patients and those with connective tissue disorders (to reduce cumulative radiation exposure). When the false lumen diameter reaches 5.5 cm (or 5.0 cm in Marfan syndrome), elective surgical or endovascular repair is recommended before rupture risk becomes prohibitive.
Activity and Lifestyle
- Exercise: Moderate aerobic activity (walking, cycling, swimming) is encouraged. Heavy weightlifting, competitive contact sports, and isometric exercises that cause sudden blood pressure spikes (holding breath while straining — the Valsalva maneuver) should be avoided.
- Smoking: Complete cessation is mandatory — smoking accelerates medial degeneration and blood pressure dysregulation.
- Cocaine and stimulant drugs: Absolutely contraindicated for life.
- Pregnancy: Women who have had aortic dissection and wish to become pregnant require specialized high-risk obstetric and cardiology co-management. Pregnancy carries substantial risk of re-dissection, particularly in connective tissue disorder patients.
Genetic Testing and Family Screening
Patients under 60 who dissect without severe hypertension, and all patients with clinical features of connective tissue disorders, should be offered genetic evaluation. First-degree relatives of patients with heritable aortopathies (Marfan, Loeys-Dietz, vascular EDS) should be screened with echocardiography or MRI and, if indicated, genetic testing. Early identification allows prophylactic surgery before dissection occurs.
Emotional Recovery
Aortic dissection is psychologically traumatic. Many survivors experience post-traumatic anxiety, fear of re-dissection, and depression during the months of recovery. These are normal responses to a life-threatening event. Psychological support, peer support groups (such as the Aortic Dissection Awareness community), and honest conversation with your cardiology team are important parts of recovery.
Back to Table of ContentsResearch Papers
The following peer-reviewed studies form the evidence base for current aortic dissection diagnosis and management:
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Alfson DB et al. PMID 22800851 — Type A aortic dissections: current management and outcomes. Review of surgical approaches and perioperative strategies for ascending aortic dissection at high-volume centers.
- Search PubMed
Connections
- Cardiology
- Aortic Aneurysm
- Cardiac Tamponade
- Hypertension
- Aortic Regurgitation
- Cardiovascular Disease
- Abdominal Aortic Aneurysm
- Stroke
- Peripheral Artery Disease
- Chest Pain
- Syncope