Aortic Aneurysm: History and Discovery
The story of the aortic aneurysm is one of the longest and most dramatic in all of surgery. The word itself comes from the Greek aneurysma, meaning a widening or dilation, and the disease was recognized by the great physicians of antiquity — Galen described it in the second century, and his contemporary Antyllus devised a surgical treatment so well reasoned that it remained the standard for more than a thousand years. From a Renaissance anatomist's first glimpse of a swollen aorta in a cadaver, through the syphilis epidemics that made aneurysms a leading cause of sudden death, to the Dacron grafts and stent-grafts of the twentieth century, the history of the aortic aneurysm traces the entire arc of medicine's long struggle to repair the body's largest blood vessel. This page tells that history with care to distinguish ancient observation from modern cure, and to credit each milestone accurately.
Table of Contents
- What an Aortic Aneurysm Is, and Where Its Name Comes From
- Galen, Antyllus, and the Ancient World
- Vesalius and the Renaissance Anatomists
- Syphilis and the Aneurysm Before Antibiotics
- Ligation, Wiring, and the Limits of Early Surgery
- Rudolph Matas and Endoaneurysmorrhaphy
- Dubost, DeBakey, Cooley, and the Dacron Graft
- Parodi and the Endovascular Revolution
- Abdominal Versus Thoracic, and the Enduring Lesson of Rupture
- Research Papers and References
- Connections
- Featured Videos
What an Aortic Aneurysm Is, and Where Its Name Comes From
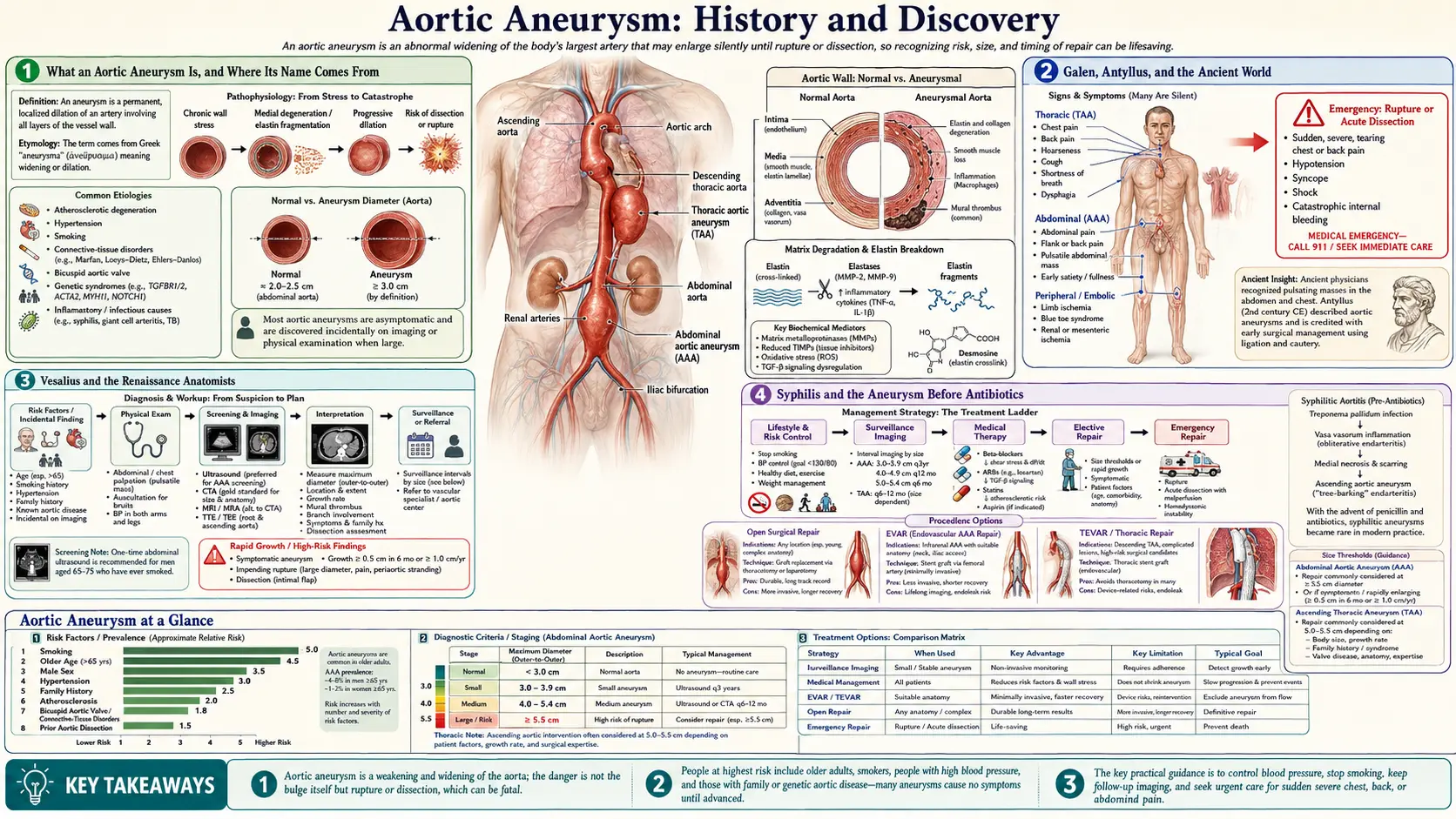
An aortic aneurysm is a permanent, localized ballooning of the aorta — the great vessel that carries blood out of the heart and down through the chest and abdomen. As the wall weakens and stretches, the swelling grows under the relentless pressure of every heartbeat, and the chief danger is that it may eventually tear or burst. Because the aorta carries the body's entire cardiac output, a rupture is a catastrophic, often fatal hemorrhage. That single, terrifying fact — a swelling that can kill in minutes — is what has driven physicians to study and attempt to repair these lesions for nearly two thousand years.
The name records the disease's most visible feature. Aneurysm derives from the Greek aneurysma, built from ana- (up, throughout) and eurys (wide), and most often translated as "a widening" or "a dilation." The word reaches back to the Greek medical tradition and was applied to exactly what an observer would see or feel: an abnormal, pulsating widening of an artery. The term has survived essentially unchanged from antiquity to the modern operating room, a rare instance of a single word carrying a medical idea intact across more than twenty centuries.
Aneurysms are classified by where they occur. An abdominal aortic aneurysm (AAA) affects the segment of aorta below the diaphragm and is the most common form; a thoracic aortic aneurysm affects the portion within the chest. As later sections describe, these two locations have very different historical associations — the thoracic aorta was for centuries the domain of syphilis, while the abdominal aorta became the proving ground for modern surgical and endovascular repair.
Galen, Antyllus, and the Ancient World
The aneurysm enters the written medical record in the classical Mediterranean. The Greek physician Galen of Pergamon (c. 129–c. 216 CE), the most influential medical authority of antiquity and of the long centuries that followed, is generally credited with giving the first clear description of an aneurysm. He characterized it as a localized, pulsatile swelling that diminished when pressed, and he warned of the consequence of injuring one: that the blood would gush out and be very difficult to stop. That description — a pulsating swelling, and a fountain of blood if breached — remains clinically accurate today.
Galen's contemporary, the Greek surgeon Antyllus (active in the second century CE), is the more remarkable figure for the history of treatment. Antyllus described a genuine surgical operation for aneurysm of the limbs: he placed ligatures on the artery both above (proximal to) and below (distal to) the swelling, then opened the sac, evacuated its clotted contents, and packed the cavity. This proximal-and-distal ligation with evacuation was a sophisticated, anatomically reasoned procedure — an attempt to isolate the lesion from the circulation before opening it — and it is justly celebrated as one of the earliest documented vascular operations. The original works of Antyllus do not survive intact; his method is known chiefly through later Byzantine medical compilers such as Oribasius and Aetius of Amida, who preserved and transmitted it.
The durability of the Antyllus method is one of the striking facts of surgical history: with refinements it remained the standard surgical approach to aneurysm for well over a millennium, into the nineteenth century. It is important, however, to be precise about its scope. Antyllus's operation was practical for accessible aneurysms of the limbs, not for the aorta deep within the chest or abdomen, which lay entirely beyond the reach of ancient surgery. Galen and Antyllus named, described, and even operated on aneurysms in general; surgery of the aorta itself would have to wait nearly two thousand years more. These ancient authors are cited here as historical figures whose work is documented in the surgical-history literature listed below.
Vesalius and the Renaissance Anatomists
For more than a millennium after Galen, anatomical knowledge of the aorta advanced little, in part because systematic dissection of the human body was rare. That changed in the sixteenth century with the work of Andreas Vesalius (1514–1564), the Flemish anatomist whose De Humani Corporis Fabrica (1543) overturned errors inherited from Galen and founded modern human anatomy. Working directly with cadavers in the new tradition of careful post-mortem dissection, Vesalius observed and described the diseased, dilated aorta.
Vesalius is widely credited as the first to diagnose and describe aortic aneurysm — both thoracic and abdominal — in the mid-sixteenth century, the recognition usually associated with his dissections around 1555. This was a milestone of understanding rather than of treatment: it placed the aneurysm of the aorta itself, deep in the body, on the anatomical map for the first time. Yet recognizing the lesion and being able to repair it were separated by an enormous gulf. As surgical historians often note, more than three centuries would pass between Vesalius's description of the abdominal aortic aneurysm and the first successful operation to remove one.
Vesalius worked in the same generation as the great French surgeon Ambroise Paré, and the two are sometimes mentioned together in the early aneurysm literature. The Renaissance anatomists could now see the disease in the body after death and reason about its location and danger, but the living aorta remained untouchable: there was no anesthesia, no antisepsis, no way to control the torrential bleeding that opening it would cause. The aneurysm of the aorta was, for the time being, a diagnosis without a cure.
Syphilis and the Aneurysm Before Antibiotics
To understand why aortic aneurysm loomed so large in the medicine of earlier centuries, one must understand its leading cause before the antibiotic era: syphilis. In its late, tertiary stage — typically fifteen to thirty years after the original infection — syphilis attacks the wall of the aorta in a process called syphilitic aortitis. The infection inflames and destroys the supporting tissue of the vessel wall, which then bulges outward, classically in the ascending thoracic aorta near the heart. In the pre-penicillin world, tertiary syphilis was the most commonly reported cause of thoracic aortic aneurysm, and cardiovascular syphilis was responsible for a substantial share of cardiovascular deaths.
The result was a disease that nineteenth- and early-twentieth-century physicians knew well and dreaded. A syphilitic thoracic aneurysm could grow until it pressed on the windpipe, the nerves to the voice box, or the breastbone, and could finally erode through the chest wall or burst — a feared and dramatic mode of sudden death described in many medical texts of the period. Because the underlying infection could not be cured, treatment was limited to managing symptoms and, in some hands, the desperate surgical experiments described in the next section.
The transformation came with effective antibacterial treatment of syphilis, above all the introduction of penicillin in the 1940s, which made it possible to treat the infection in its earlier stages before it ever reached the aorta. Within a generation, syphilitic aortic aneurysm went from a common, recognizable disease to a medical rarity in the developed world. Its near-disappearance also changed the very meaning of the diagnosis: the aortic aneurysm of the later twentieth century is overwhelmingly a disease of degeneration — of atherosclerosis, aging, smoking, and high blood pressure — rather than of infection, which is one reason the modern surgical story centers on the abdominal aorta rather than the syphilitic thoracic aorta of earlier eras.
Ligation, Wiring, and the Limits of Early Surgery
Between Vesalius and the modern operating room lies a long, often heroic, and frequently tragic chapter of attempts to treat aneurysms that surgeons could not safely cut out. For accessible aneurysms of the limbs, the refined heir to the Antyllus method was simple proximal ligation — tying off the feeding artery to thrombose the sac. The Scottish surgeon John Hunter famously advanced this principle in 1785 by ligating the femoral artery well above a popliteal (knee) aneurysm at a site that came to bear his name, allowing collateral vessels to maintain the limb. Hunter's operation was a landmark for peripheral aneurysms, but it could not be applied to the aorta, where there is no way to simply tie off the main trunk without stopping the circulation to the entire lower body.
The aorta therefore inspired more exotic and largely futile measures. Surgeons and physicians of the nineteenth and early twentieth centuries tried to induce clotting inside an aortic aneurysm by threading yards of fine wire into the sac (the "wiring" technique), sometimes combined with an electric current — the so-called wiring-and-electrothermic methods. Others attempted compression of the feeding vessels or injected various agents in the hope of provoking a protective clot. These approaches were inspired by genuine ingenuity and real desperation, but they were rarely effective and often dangerous, and none of them addressed the underlying problem: a fragile, expanding aorta that could not yet be opened and rebuilt.
The fundamental obstacles were the same ones that had frustrated Vesalius's successors — uncontrollable hemorrhage, the absence of anesthesia until the 1840s and of antisepsis until the 1860s–1880s, and, above all, the lack of any way to replace a removed segment of the aorta. Real aortic surgery would have to await the twentieth-century tools of blood transfusion, anticoagulation, vascular suture technique, and prosthetic grafts. The next three sections trace how each of those pieces fell into place.
Rudolph Matas and Endoaneurysmorrhaphy
The bridge from ancient ligation to modern reconstruction was built largely by one surgeon: Rudolph Matas (1860–1957) of New Orleans, often called the father of modern vascular surgery. In 1888, faced with a traumatic aneurysm of the brachial artery in a young man's arm that had resisted ligation, Matas opened the aneurysm sac and, working from inside it, sutured shut the openings of the vessels feeding the lesion. He named the operation endoaneurysmorrhaphy — literally, suture-repair from within the aneurysm — and it proved a decisive conceptual advance: instead of merely tying off the artery from outside and hoping the sac would clot, the surgeon directly controlled the bleeding points from within.
Over the following years Matas refined and classified the technique. In a landmark treatise of 1903 he distinguished an "obliterative" form (closing the sac entirely, as in his original 1888 case) from "restorative" and "reconstructive" forms that aimed to preserve or rebuild the flow channel through the vessel — a remarkably modern ambition to maintain circulation rather than simply sacrifice the artery. Across a long career he performed and reported a large personal series of these operations with mortality far lower than the alternatives of his day.
Matas's endoaneurysmorrhaphy was the most successful method available for many aneurysms in the decades before grafts, and his idea of repairing the vessel from within prefigured the reconstructive philosophy of all later aortic surgery. It is worth being precise about its place in the timeline: endoaneurysmorrhaphy was a triumph chiefly for peripheral and selected aneurysms, and applying any such technique to the abdominal aorta remained extraordinarily difficult. The decisive step — cutting out a segment of diseased aorta and replacing it — belonged to the next generation, building directly on Matas's reconstructive ideas.
Dubost, DeBakey, Cooley, and the Dacron Graft
The modern era of aortic surgery opened in Paris on 29 March 1951, when the French surgeon Charles Dubost performed the first successful resection of an abdominal aortic aneurysm, cutting out the diseased segment and bridging the gap with a preserved human aortic graft (a cadaveric homograft). For the first time in the long history of the disease, an aortic aneurysm had been removed and the aorta restored — the operation that Vesalius's description had implied was needed nearly four centuries earlier. Dubost's success proved that the aorta could be replaced, but human homografts were scarce and tended to degenerate, calcify, and fail over time, so the technique needed a better building material.
That material, and much of the surgical technique to use it, came from a celebrated pair of American surgeons in Houston: Michael E. DeBakey (1908–2008) and Denton A. Cooley (1920–2016). In the early 1950s, working at first with homografts, the Houston group reported successful resections of thoracic and abdominal aortic aneurysms. DeBakey then turned to synthetic fabric, and in 1958 DeBakey, Cooley, and Crawford reported the clinical use of a flexible knitted graft made of Dacron (a polyester fabric) — a durable, off-the-shelf, mass-producible artificial artery. A widely repeated account holds that DeBakey, unable to find the cloth he wanted, fashioned an early experimental graft on a sewing machine; whatever the precise details, the adoption of Dacron transformed aortic surgery from a procedure limited by the supply of human grafts into a reproducible operation that could be offered broadly.
With a reliable prosthetic conduit in hand, DeBakey, Cooley, and their contemporaries went on to develop the full repertoire of open aortic surgery — for aneurysms of the abdominal aorta, the thoracic aorta, and the aortic arch, and for aortic dissection. Surgical replacement of the aorta with a Dacron graft became, and for many patients remains, the definitive cure for an aortic aneurysm. To be accurate about credit: Dubost performed the first successful abdominal aortic aneurysm resection and graft in 1951, while DeBakey and Cooley, with the Dacron graft, did more than anyone to make aortic graft replacement practical, durable, and widespread. Open graft repair would stand essentially unchallenged for three decades — until a radically different idea arrived from Argentina.
Parodi and the Endovascular Revolution
Open repair is a major operation: it requires a large incision, clamping the aorta, and considerable physiologic stress — a serious undertaking for the older patients, often with heart and lung disease, in whom aneurysms are most common. The next revolution sought to repair the aorta from inside the bloodstream, without ever opening the abdomen or chest. The breakthrough belongs to the Argentine vascular surgeon Juan Carlos Parodi, working with the interventional radiologist Julio Palmaz.
In September 1990, in Buenos Aires, Parodi performed the first successful endovascular aneurysm repair (EVAR) of an abdominal aortic aneurysm in a human patient. Rather than cutting the aneurysm out, he guided a fabric-covered stent-graft up through the femoral artery in the groin and deployed it inside the aorta, so that blood flowed through the new graft channel while the aneurysm sac outside it was sealed off from the circulation and the pressure that threatened to burst it. The landmark case — Parodi, Palmaz, and Barone — was published in 1991 in the Annals of Vascular Surgery, the report through which the technique became known to the surgical world. The first such procedure in the United States followed in 1992.
EVAR transformed the treatment of aortic aneurysms. Because it avoids a major open operation, it dramatically reduced the immediate risks and recovery time of repair and made treatment possible for many frail patients who could not safely undergo open surgery; in much of the world it is now the most common way an abdominal aortic aneurysm is repaired. It is not a universal replacement — not every aneurysm is anatomically suitable, stent-grafts require lifelong imaging follow-up to watch for leaks around or through the device (endoleaks), and open Dacron repair remains essential for many cases — but the endovascular idea, barely three decades old, completed a two-thousand-year arc: from Antyllus reaching the limb aneurysm with a knife, to Parodi reaching the aortic aneurysm with a catheter.
Abdominal Versus Thoracic, and the Enduring Lesson of Rupture
Running through this entire history is the distinction between the two homes of the disease. The thoracic aortic aneurysm, high in the chest, was for centuries the signature lesion of syphilis and is also strongly linked to inherited disorders of connective tissue and to disease of the aortic valve and root. The abdominal aortic aneurysm, below the diaphragm, is the more common form today, tied to atherosclerosis, smoking, high blood pressure, male sex, and age — and it is the abdominal aorta that became the stage for the great surgical milestones of Dubost, DeBakey, and Parodi. Recognizing which segment is involved has always shaped both the danger and the treatment.
The single fact that gives this history its urgency, from Galen to the present, is rupture. An aneurysm is dangerous not because of the swelling itself but because the swelling can tear, and when the aorta tears the bleeding is massive and frequently fatal before help can arrive. Every milestone on this page — Antyllus's ligatures, Matas's sutures, Dubost's graft, Parodi's stent-graft — was ultimately an attempt to take the pressure off a fragile wall before it could burst. The whole point of modern repair, whether open or endovascular, is the same as it was two thousand years ago: to prevent the catastrophe.
That is also why the modern emphasis falls so heavily on finding aneurysms before they rupture. Many aortic aneurysms cause no symptoms at all until the moment of crisis, so they are often discovered by chance on imaging, or through deliberate ultrasound screening of higher-risk groups, and then watched and measured over time, with repair recommended once an aneurysm reaches a size or growth rate at which the risk of rupture outweighs the risk of the procedure. The history of the aortic aneurysm is, in the end, the history of turning a sudden, hidden killer into a condition that can be detected, monitored, and — thanks to a long line of physicians from antiquity to our own time — repaired.
Research Papers and References
The references below combine peer-reviewed historical reviews of aortic and aneurysm surgery with curated PubMed topic-search links into the historical and clinical literature. The ancient and Renaissance figures named in this article — Galen, Antyllus, and Vesalius — are documented through the surgical-history reviews listed here rather than through modern primary citations. Each external link opens in a new tab.
- Bobadilla JL. From Ebers to EVARs: a historical perspective on aortic surgery. Aorta (Stamford). 2013;1(2):89-95. — doi:10.12945/j.aorta.2013.13-004
- Matas R, Antyllus, and endoaneurysmorrhaphy (history of vascular surgery). Surgery, Gynecology & Obstetrics. — PubMed 2658180
- Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Annals of Vascular Surgery. 1991;5(6):491-499. — doi:10.1007/BF02015271
- Early history of aortic surgery (Vesalius, syphilis, ligation, and the first graft repairs). Journal of Vascular Surgery. — doi:10.1016/S0741-5214(98)70107-7
- Galen, Antyllus, and the ancient surgical treatment of aneurysm — PubMed: Antyllus and the history of aneurysm surgery
- Andreas Vesalius and the early description of aortic aneurysm — PubMed: Vesalius and aortic aneurysm
- Syphilis as a cause of thoracic aortic aneurysm (syphilitic aortitis) — PubMed: syphilitic aortitis and thoracic aneurysm
- Rudolph Matas and the development of endoaneurysmorrhaphy — PubMed: Matas and endoaneurysmorrhaphy
- Charles Dubost and the first abdominal aortic aneurysm resection (1951) — PubMed: Dubost and the first AAA resection
- DeBakey, Cooley, and the Dacron arterial graft — PubMed: DeBakey, Cooley, and the Dacron graft
- History and milestones of endovascular aneurysm repair (EVAR) — PubMed: history of EVAR
- John Hunter, proximal ligation, and the history of peripheral aneurysm surgery — PubMed: John Hunter and aneurysm ligation
- General history of aortic aneurysm surgery, past to present — PubMed: history of aortic aneurysm surgery
- Etymology and historical concepts of the term "aneurysm" — PubMed: history and definition of aneurysm
External Authoritative Resources
- NHLBI (National Heart, Lung, and Blood Institute) — Aneurysm
- MedlinePlus — Aortic Aneurysm
- PubMed — All research on the history of aortic aneurysm
Connections
- Cardiology
- Aortic Aneurysm
- Atherosclerosis
- Hypertension
- Peripheral Artery Disease
- Coronary Artery Disease
- Stroke
- All Conditions